










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Dental Journal
versión On-line ISSN 0375-1562
versión impresa ISSN 0011-8516
S. Afr. dent. j. vol.78 no.6 Johannesburg jul. 2023
http://dx.doi.org/10.17159/sadj.v78i06.16944
RESEARCH
A correlation between the timing of skeletal maturity and dental development in black South African Patients
RT OppermanI; MPS SethusaII; DM LetsholoIII
IBChD, PDD, MDS, Registrar, Department of Orthodontics, Sefako Makgatho Health Sciences University, South Africa. ORCID: 0009-0006-4663-7260
IIB Rad, BDS, M Dent (Orthodontics), Orthodontic Specialist, Private Practice, Pretoria, South Africa. ORCID: 0000-0002-0884-3008
IIIDip OH, BDS, PDD, M Dent (Orthodontics), Orthodontic Consultant, Sefako Makgatho Health Sciences University, South Africa. ORCID: 0000-0003-3256-4022
ABSTRACT
INTRODUCTION: The growth potential of patients has a significant influence on the timing of orthodontic intervention and treatment modalities. Skeletal maturity and dental development are biological maturity indicators which can be used to determine the growth status of an individual
OBJECTIVES: To correlate the dental maturational stages of black South African individuals with the stages of skeletal maturation and to determine the diagnostic accuracy of using dental developmental stages to identify an individual's skeletal maturity
DESIGN: Retrospective, cross-sectional study
METHODS: Skeletal maturity and dental development of 224 subjects were assessed using lateral cephalograms and panoramic radiographs, respectively. Statistical analyses included descriptive statistics, Spearman's correlation coefficient and positive likelihood ratios (LHR
RESULTS: The highest (rs=0.759, p<0.001) correlation with skeletal maturity was identified for the second molar and the lowest correlation (rs=0.662, p<0.001) for the canine. Positive LHR>10 combined with sensitivity and specificity testing revealed that the second premolar (stage E), second molar (stage F) and second molar (stage H) have the most significant diagnostic reliability to identify the pre-pubertal, pubertal and post-pubertal growth phases, respectively
CONCLUSION: Dental development is a valuable diagnostic tool to assess skeletal maturation. The calcification of the second molar (stage F) is predictive of the pubertal growth phase
Keywords: Skeletal growth, dental development, skeletal maturity, dental calcification, CVM
INTRODUCTION
Timing of orthodontic intervention is fundamental during the treatment planning process, with special regard to growing individuals requiring growth modification treatment.1 Dental as well as skeletal disharmonies may be corrected or improved by orthodontic treatment and initiating treatment at the ideal time in young patients has revealed favourable outcomes in the correction of skeletal discrepancies.2
The craniofacial structures experience a growth acceleration which is similar to other parts of the body during the pubertal growth spurt.3 It is therefore essential that the orthodontist determines the growth status of young patients and in particular their proximity to the peak of the adolescent growth spurt for optimal treatment planning and utilisation of the patient's growth potential, before performing growth modification procedures. Furthermore, timeous referral of patients to orthodontists by general practitioners is critical to initiate orthodontic treatment at the most ideal time.1 Chronological age is not a reliable method to estimate the skeletal growth status or physiological maturity of a young patient and should not be used to ascertain a patient's maturational state.4,5 Instead of focusing on chronological age, the physiological maturity or biological age of a patient should be assessed.
The left hand-wrist analysis6 has been reliably used in orthodontics to determine a patient's skeletal maturity; however, this method requires extra cost and radiation, and so does the median phalanx index (MP3) introduced by Hãgg and Taranger in 1982.7
In view of the limitation of the hand-wrist and MP3 analyses, Hassel and Farman8 introduced the cervical vertebrae maturation (CVM) analysis as an alternative method to assess skeletal maturation. Although this method has been found to be as reliable as the hand-wrist analysis9, a lateral cephalogram is required to evaluate the maturation of the cervical spine and general dental practitioners may not have access to the requisite radiographic machine to acquire this image.
Apart from skeletal maturity, other biological indicators such as an increase in body height10, voice changes, menarche11 and dental development12 can also be used to determine an individual's growth status; however, these are not popularly used in dentistry and the available literature focuses predominantly on skeletal maturity indicators to assess growth.
Dental development, similar to skeletal maturation, has been investigated in the past as a method to determine physiological maturity12 and although individual variations among different populations were identified, high correlations have been demonstrated between dental calcification stages and skeletal maturity indicators.13-16 The advantage of this method is that dental development can be analysed from a panoramic radiograph which is routinely used in orthodontics and general dental practice to evaluate a patient's oral health status and should be readily available for the majority of patients.17-19 No additional radiographs are necessary, limiting radiation and cost to the patient.
The objectives of this study were to correlate the skeletal maturation stages of black South African patients to the stages of dental calcification as viewed on a panoramic radiograph and to determine whether dental calcification stages can be used accurately to determine a patient's physiological age.
MATERIALS AND METHODS
Ethics approval
The study protocol was approved by Sefako Makgatho University Research Ethics Committee (SMUREC) with ethics reference number SMUREC/D/114/2022: PG. The researcher was granted access to patient records by the CEO of Sefako Makgatho University Oral Health Centre and the Department of Maxillofacial and Oral Radiology to collect data for this research project.
Study sample
Lateral cephalograms and panoramic radiographs of patients who have visited the Orthodontic Department at Sefako Makgatho Health Sciences University in Ga-Rankuwa, South Africa were collected for this study.
Overall, 523 patient records were searched for patients who satisfied the eligibility criteria for this study and the resulting sample consisted of 224 patients in total. The sample consisted of 104 males and 120 females with a mean age of 11.7 years (age range 9.7-16 years). This sample size satisfies the requirements to calculate the Spearman rank order correlation as proposed by Bonett and Wright20 and is in line with similar studies.4,21,22
Individuals who fulfilled the following criteria were included in this study:
• Male and female patients from 7 to18 years of age, following the sampling criteria of similar studies;3,14,22
• Black South African descent;
• Panoramic as well as a lateral cephalometric radiograph available, taken within the same month;
• Radiographs which exhibit high clarity, good contrast and without any noticeable distortions;
• No craniofacial or systemic anomalies or history of facial trauma; and
• No dental anomalies (caries, impactions or congenitally absent teeth).
Methodology
Demographic information, panoramic and lateral cephalometric radiographs of the study sample were collected from patient records. All radiographs were taken using a Carestream Kodak 8000C0 digital panoramic and cephalometric X-ray machine. The radiographs were taken by a radiographer, or a senior undergraduate dentistry student supervised by a radiographer, within the Department of Maxillofacial and Oral Radiology at Sefako Makgatho Health Sciences University. Digital as well as printed radiographs were collected - the hard copies were used for tracing purposes, whereas the digital copies were used to enhance the contrast or brightness of the radiographs when necessary to assist with the evaluation. Magnification errors were not significant in this study because proportional relationships between skeletal or dental structures were used instead of actual lengths.
Radiographs were separated and the principal researcher was blinded to the patient's demographic details. This ensured the investigator was not influenced by the patient's age, gender or other radiograph. Patient demographics were collected from patients' hospital files; gender, ethnicity and date of birth were recorded for each study participant. The date of radiographic exposure was also noted, enabling the researcher to calculate the age of each participant at the time when the radiographs were taken. The selected age range covered the adolescent growth period and data from prepubertal, pubertal and postpubertal skeletal maturational stages were collected.
Assessment of skeletal maturity
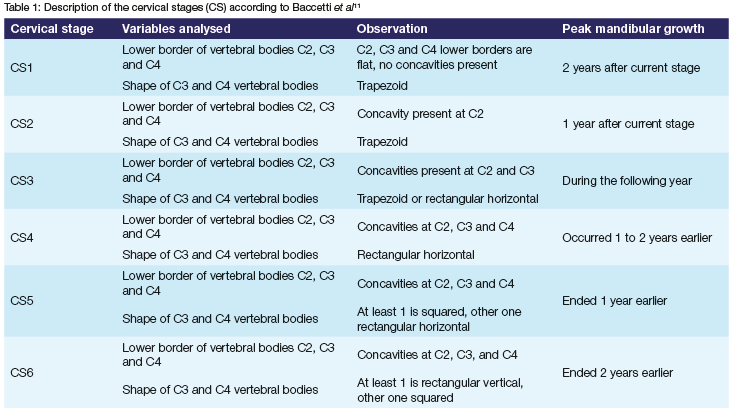
The morphology of the second (C2), third (C3) and fourth (C4) cervical vertebrae bodies were evaluated from the collected lateral cephalograms and the skeletal maturity of each patient was determined using the cervical vertebral maturation stage (CVMS) method of Baccetti et al.11 (Table 1). The validity and reliability of this technique to determine the skeletal maturity of an individual is well established within the literature.9,23,24 For this study, participants were grouped into three groups of potential clinical interest according to their skeletal stage of maturation.21,22,25
Group 1: Prepubertal (CS 1)
Group 2: Pubertal (CS 2 and 3)
Group 3: Postpubertal (CS 4, 5 and 6)
Assessment of dental development
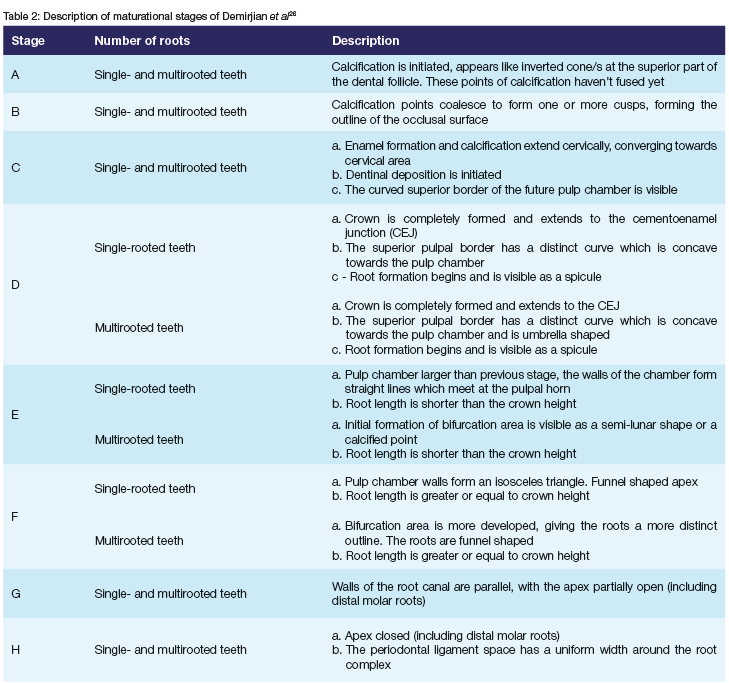
The stage of dental development was determined from the panoramic radiographs by using the Demirjian et al.26 calcification stages (Table 2). Similar to comparable studies, this study only evaluated the permanent lower left canine, first premolar, second premolar and second molar and noted their stage of calcification (Stages A-H).21,22 The assessment was restricted to teeth on the left side only because contralateral teeth have been found to develop symmetrically.26 As with similar studies, the maxillary teeth were not examined for this study because superimpositions of maxillary structures can result in incorrect assessments.15,22 Furthermore, the permanent incisors and first molars were excluded from this study because it is expected that root formation of these teeth should be complete or close to completion in the age range of the current population group21 and third molars were not examined either due to their late development and high tendency of being congenitally absent.27
Statistical analysis
Descriptive and inferential statistics were performed using SAS (SAS Institute Inc, Cary, NC, USA), Release 9.4. Spearman rank order correlation coefficients were calculated between the CVM growth phases and dental calcification stages for each of the four individual teeth. Positive likelihood ratios with 95% confidence intervals were calculated for each individual tooth as measures of dental maturation stages for identifying growth phases. Sensitivity and specificity values, with 95% confidence intervals, were calculated for all the cases where the likelihood ratio was >10.
Intra-examiner as well as inter-examiner analyses were performed to determine the reliability and reproducibility of the study results.28 The principal researcher assessed all the radiographs of the study population at two different occasions under the same conditions to establish the intra-examiner reliability. To evaluate the inter-examiner reliability, 10 sets of radiographs were randomly selected and assessed by another clinician of equal training as the principal researcher. The Spearman rank correlation coefficients between the overall first and second assessments, and between the two examiners, were calculated to measure intra- and inter-examiner reliability.
RESULTS
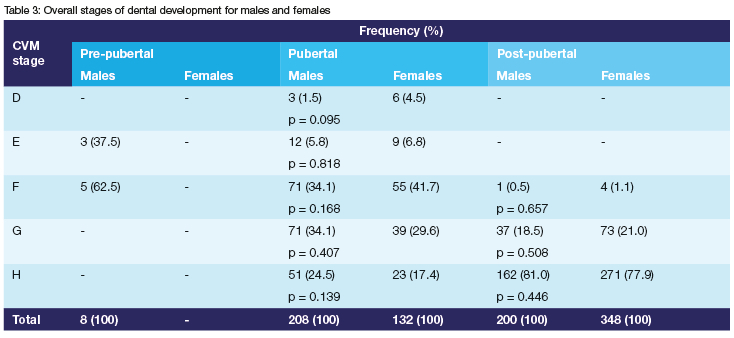
The assessments of the stages of dental calcification of males and females were statistically compared per CVM stage (Table 3) and no significant difference was found between genders and, as such, the further analyses in this study are presented as a single collective sample of 224 cases. Correlation analyses were performed to determine the reliability and reproducibility of this study. The Spearman rank correlation coefficient between the overall first and second assessments and between two examiners were calculated. The results for intra-examiner (rs=0.99) as well as inter-examiner (rs=0.98) measurements were highly significant (p<0.001), suggesting strong correlations for intra- and inter-examiner reliability and an almost perfect reproducibility of findings. The overall first assessments were used for the statistical analysis of this study.
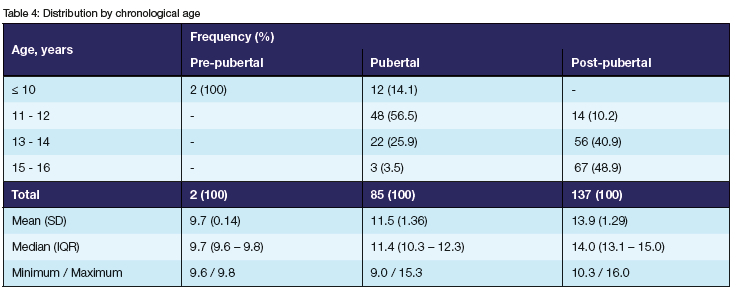
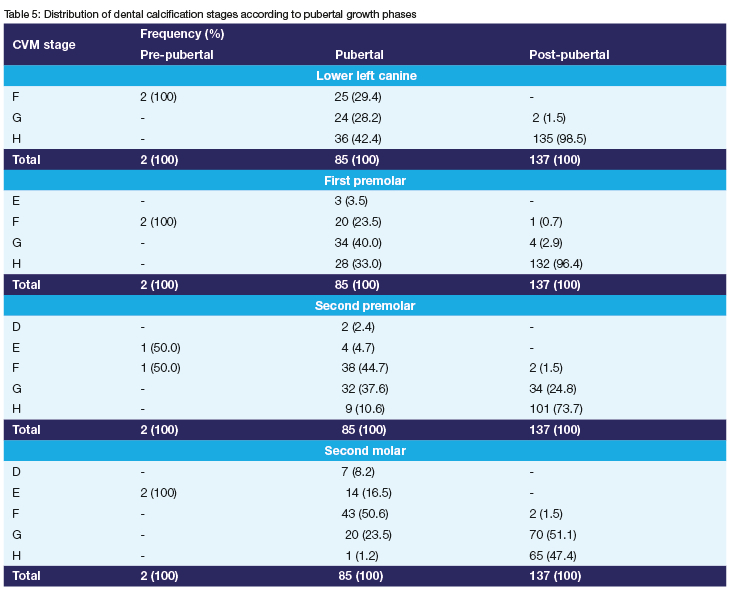
Table 4 illustrates the distribution of participants by chronological age and the distribution of dental calcification stages per tooth according to the skeletal maturation stages are presented in Table 5.
Correlations between skeletal growth phases and dental calcification stages
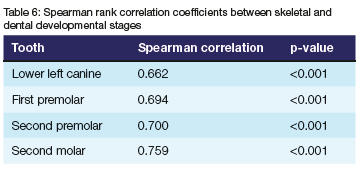
Spearman rank order correlation coefficients were calculated between the CVM growth phases and dental calcification stages for each of the four individual teeth and the results are presented in Table 6. The correlation coefficients are all highly significant (p-values<0.001), with a maximum value for the second molar (rs=0.759). The canine (rs=0.662) revealed the lowest correlation.
Likelihood ratios
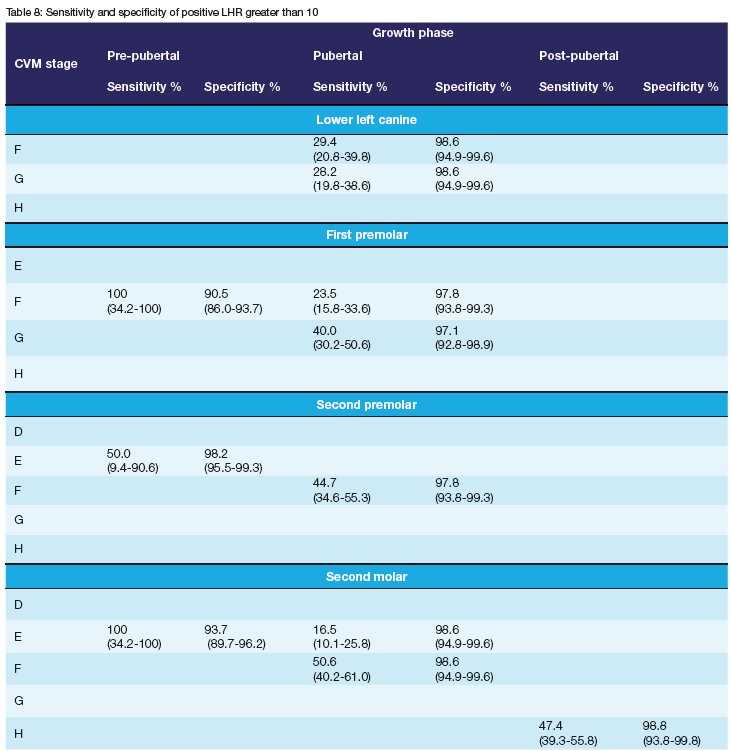
Positive likelihood ratios (LHR) with 95% confidence intervals were calculated for each individual tooth as measures of the diagnostic accuracy of using dental calcification stages to identify skeletal growth phases. The results are summarised in Table 7, likelihood ratios of 10 or greater are bolded. In Table 8, sensitivity and specificity values, with 95% confidence intervals, were calculated for all LHR>10.
A positive LHR>10 identified the pre-pubertal growth phase associated with the first premolar (stage F, positive LHR of 10.6; 95% CI 7.0-15.9), second premolar (stage E, positive LHR of 27.8; 95% CI 5.1-150.7), and second molar (stage E, positive LHR of 15.9; 95% CI 9.6-26.3). Following sensitivity and specificity testing (Table 8), the second premolar (stage E) revealed the greatest diagnostic reliability to identify the pre-pubertal growth phase, with a specificity of 98.2%. The small sample size within the pre-pubertal group should be noted.
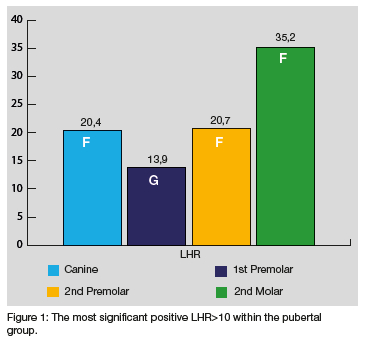
The pubertal growth phase (Figure 1) was identified by a positive LHR greater than 10 which was found to be associated with the canine (stage F, positive LHR of 20.4; 95% CI 5.0-84.1 and stage G, positive LHR of 19.6; 95% CI 4.8-80.9), first premolar (stage F, positive LHR of 10.9; 95% CI 3.3-35.6 and stage G, positive LHR of 13.9; 95% CI 5.1-37.8), second premolar (stage F, positive LHR of 20.7; 95% CI 6.6-65.0), and second molar (stage E, positive LHR of 11.4; 95% CI 2.7-49.1 and stage F, positive LHR of 35.2; 95% CI 8.7-141.4). The second molar (stage F) revealed the most significant diagnostic reliability to identify the pubertal growth phase with a LHR of 35.2 and specificity of 98.6%.
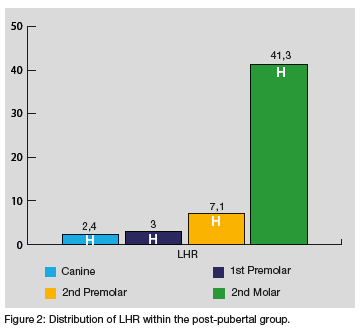
A positive LHR>10 of the second molar (stage H, positive LHR of 41.3; 95% CI 5.8-292.1) is indicative of the post-pubertal growth phase. The specificity is 98.8% which suggests high diagnostic reliability (Figure 2).
DISCUSSION
In this study the objectives were to correlate the dental maturational stages of black South African individuals with the stages of skeletal maturation and to determine the diagnostic accuracy of using dental developmental stages to identify the skeletal maturity of individuals within this population. Dental calcification stages, as described by Demirjian et a/.26, were identified from panoramic radiographs and correlated with the skeletal maturity of each participant, which was determined by the maturational status of their cervical vertebrae as observed from a lateral cephalogram.11 The methodology of the present study was validated and considered to be reliable by similar previous studies21,22,29; however, the focus of this study was on black South African individuals.
In accordance with similar studies, the results from analyses carried out in this study yielded no statistically significant difference between genders and the results in this study were presented as a single combined sample.22,25
Despite an adequate sample size, this study was restricted to black South African individuals presenting for treatment at a single centre. This may limit the generalisability of the results to other populations and ethnic groups. Variability in the timing of skeletal maturation as well as dental calcification between different ethnic groups have been reported by previous studies and should be considered when interpreting the results from this study.4,13,14,30 Ideally, population-specific data should be gathered and implemented for different ethnic groups.
Correlation between dental calcification stages and stages of cervical vertebral maturation
Spearman rank correlation coefficient values were calculated for each tooth to determine whether there is an association between dental development and skeletal maturity. In general, the correlation coefficients between the stages of dental calcification of the four individual teeth and the three CVM growth phases were found to be high, varying from 0.662 to 0.759 (p<0.001) in this study. These findings are indicative of a significant correlation between dental calcification stages and skeletal maturation and agree with comparable studies. 4,13,14,21,22,25,30 A systematic review and meta-analysis by Bittencourt et al,31 however, reported that although the literature suggests a significant association between skeletal maturity and dental development, there is a great heterogeneity among studies and they concluded that standardised observational studies are necessary to strengthen the evidence and to confirm the use of dental calcification stages to accurately estimate the pubertal growth spurt.
In this study, the tooth which provided the highest correlation between its calcification stages and phases of CVM was the lower second molar. Uysal et al,14 Litsas et al22 and Lecca-Morales and Carruitero32 reported similar results in Turkish, Greek and Peruvian subjects, respectively. An Italian study by Perinetti et al.25 was also in agreement with these results. In contrast with the current findings, Valizadeh et al.30 found the first premolar to have the highest correlation, whereas Krailassiri et al.13 reported that the second premolar had the highest correlation with skeletal maturity among Thai individuals.
A South African study by Chertkow4 in 1980 found that the lower canine had the highest correlation with skeletal maturity in caucasian subjects; however, his findings in black South African individuals were inconclusive due to earlier dental development in this population which led to most of the root development being complete by the time he studied them. Uys et al.33 confirmed that racial differences exist during dental maturation and that black South African individuals mature earlier than caucasian individuals.
High correlation coefficients, however, only suggest a strong association between two variables and, despite the high correlations found by this and previous studies, further analyses are necessary to determine the diagnostic accuracy of dental calcification stages to predict the pubertal growth status of an individual. The majority of the previous studies4,13,14,30,32 didn't comprehensively analyse the true diagnostic potential of dental calcification stages.
Diagnostic accuracy of using dental calcification stages to estimate skeletal maturity
Likelihood ratios (LHR), together with 95% confidence intervals (CI), were calculated for each of the calcification stages observed in the four teeth evaluated in this study to determine the clinical reliability of individual dental calcification stages to diagnose skeletal maturity and thereby estimate the pubertal growth status of an individual. A positive LHR is an estimate of the extent to which a specific dental calcification stage improves the odds of being present in a certain growth phase and LHR greater than 10 were considered to be significant.34 Sensitivities and specificities were also calculated for the stages of dental calcification which had LHR>10 to comprehensively analyse the diagnostic performance of these stages.
Pre-pubertal phase of skeletal maturation
In the current study, the first premolar, second premolar and second molar revealed positive LHR greater than 10 to identify the pre-pubertal growth period. For the first premolar stage F and for the second premolar and second molar,
stage E showed LHR>10. The canine didn't have a positive LHR>10 in the pre-pubertal group. The second premolar stage E presented the highest LHR (LHR 27.8) and together with a specificity value of 98.2%, this is suggestive of high diagnostic capability for the pre-pubertal growth phase. The reliability of the current results is, however, compromised by an inadequate number of participants (n=2) within this group. Further research focused on the pre-pubertal population will be necessary to obtain sufficient data to be analysed in this population. Data collection in this group is challenging because the available subjects who meet all the inclusion criteria is limited because it is not as common for patients this young, compared to adolescent patients, to present for orthodontic treatment.
Although the current pre-pubertal group had an inadequate sample size, some of the findings are consistent with similar studies. Perinetti et al.25 and Litsas et al.22 reported LHR>10 for the second premolar stage E (LHR 12.8 and LHR 11.1, respectively) as well. This study and that of Litsas et al.22 didn't have any positive LHR>10 for the canine; however,
Perinetti et al.25 reported LHR>10 for the canine stage F (LHR 14.9). Contrary to the current findings, for the first premolar Litsas et al.22 found LHR>10 for stages D (LHR 16) and E (LHR 20) and for the second molar, stage D (LHR 14.4). Results from Perinetti et al.25 regarding the first premolar and second molar corresponded closely with that of Litsas et al.22
Pubertal phase of skeletal maturation
All four of the teeth evaluated in this study revealed positive LHR>10 within the pubertal group: Stages F and G for the canine and first premolar, stage F for the second premolar, and stages E and F for the second molar. The highest LHR was identified for the second molar stage F (LHR 35.2), which has a specificity of 98.6%. Although the large confidence interval (8.7-141.4) should be noted, these results are highly suggestive that second molar stage F of dental calcification (well-developed bifurcation area, funnel shaped roots, with the root length being equal or greater than the crown height) is a reliable diagnostic tool to identify the pubertal growth phase. These results correspond with the high correlation coefficient observed in this study between development of the second molar and skeletal maturation.
The current findings agree with results from Litsas et al.22 Litsas et al.22 similarly reported a positive LHR>10 for second molar stage F (LHR 13.6), finding it to be an accurate diagnostic parameter for identifying the pubertal growth period. Several other studies have also found a positive relationship between the second molar calcification stage F and various skeletal maturity indicators of the adolescent growth phase.13,14,35 A recent study, based on patient records from the Burlington Growth Centre, reported gender differences and concluded that the pubertal growth phase can potentially be identified by second molar calcification stage F in females and stage G in males.36 Most of the other studies were, however, limited by only considering the distribution of the dental calcification stages during skeletal maturation or by restricting their statistical analyses to correlation coefficients. Accurate diagnostic testing is necessary in addition to high correlation coefficients.
Contrary to this study, Perinetti et al.25 didn't find any positive LHR>10 for any of the four teeth in the pubertal group, leading them to doubt the diagnostic capability of
dental calcification stages. Methodological differences may be responsible for the variations between this study and the findings by Perinetti et al.25
Post-pubertal phase of skeletal maturation
According to the current results, only one tooth, the second molar, revealed a positive LHR>10 in identifying the post-pubertal growth phase. The second molar's stage H proved to have reliable diagnostic performance to accurately identify the post-pubertal growth period by yielding a LHR of 41.3 with a specificity of 98.8%. Findings by Litsas et al.22 are comparable to these results: they also reported a positive LHR (LHR 18.9) for the second molar stage H during the post-pubertal phase. A LHR close to 10 (LHR 9.1) was found for second molar stage H by Perinetti et al.25: although their value was <10, it was significantly greater than other finding within the post-pubertal group. These results confirm that the completion of root formation of the second molar (stage H) is an indication that the pubertal growth peak has passed and the subject is in the post-pubertal period.
In summary the overall results from the current study are in line with similar studies.14,22,25,35 A significant correlation was found between dental calcification stages and skeletal maturity. The second molar's stage F demonstrates diagnostic reliability to identify the peak adolescent growth phase within the population studied, whereas the second molar's stage H is an accurate indication that an individual is within the post-pubertal phase of growth. Certain characteristics of the second molar may be beneficial for using it as an indicator for skeletal maturity; for example, the second molar is generally not affected by dental irregularities, it develops around the time of puberty in most individuals and it can easily be assessed from a panoramic radiograph.36 Determining the growth status of patients is essential for timely orthodontic referrals and for initiating orthodontic treatment at the most appropriate time.11,21
STUDY LIMITATIONS
Generalisability of the current study results is limited by: The focus of this study was on black South African individuals only and due to ethnic differences observed during growth and development, these results may not be accurate for other ethnic groups.
The study population was sampled from one centre only, therefore the results cannot be generalised to the entire black South African population.
The sample size within the pre-pubertal group was insufficient and the results could not be used to draw a conclusion within this group.
CONCLUSION
The correlation between skeletal maturity and dental development was investigated within a black South African population and from the results it can be concluded that a significant correlation exists between these variables. Dental maturation of the lower left second molar (stage F), as visible on a panoramic radiograph, can accurately be used as a diagnostic tool to predict the pubertal growth phase for the study population. Completion of root formation (stage H) of the second molar is predictive of the post-pubertal phase.
The clinical relevance of this study enables clinicians to identify the pubertal and post-pubertal growth phases of patients from an intra-oral or a panoramic radiograph as a first diagnostic tool. This will contribute to timely orthodontic referrals and appropriate timing of orthodontic intervention.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
No funding was applied for nor received for this research project.
REFERENCES
1. Franchi L, Baccetti T, De Toffol L, Polimeni A, Cozza P. Phases of the dentition for the assessment of skeletal maturity: a diagnostic performance study. Am J Orthod Dentofacial Orthop. 2008;133(3):395-400 [ Links ]
2. McNamara JA, Brudon WL, Kokich VG. Orthodontics and dentofacial orthopedics, 3rd ed. Ann Arbor, Michigan: Needham Press, 2001:78-80 [ Links ]
3. Al-Balbeesi HO, Al-Nahas NW, Baidas LF, Bin Huraib SM, Alhaidari R, Alwadai G. Correlation between skeletal maturation and developmental stages of canines and third molars among Saudi subjects. Saudi Dent J. 2018;30(1):74-84 [ Links ]
4. Chertkow S. Tooth mineralization as an indicator of the pubertal growth spurt. Am J Orthod. 1980;77(1):79-91 [ Links ]
5. Buschang PH, Roldan RI, Tadlock LP. Guidelines for assessing the growth and development of orthodontic patients. Semin Orthod. 2017;23(4):321-35 [ Links ]
6. Grave KC, Brown T. Skeletal ossification and the adolescent growth spurt. Am J Orthod. 1976;69(6):611-9 [ Links ]
7. Hãgg U, Taranger J. Maturation indicators and the pubertal growth spurt. Am J Orthod. 1982;82(4):299-309 [ Links ]
8. Hassel B, Farman AG. Skeletal maturation evaluation using cervical vertebrae. Am J Orthod Dentofacial Orthop. 1995;107(1):58-66 [ Links ]
9. Gandini P, Mancini M, Andreani F. A comparison of hand-wrist bone and cervical vertebral analyses in measuring skeletal maturation. Angle Orthod. 2006;76(6):984-9 [ Links ]
10. Petrovic AG, Stutzmann JJ. New ways in orthodontic diagnosis and decision-making: physiologic basis. J Japan Orthod Soc. 1992;51:3-25 [ Links ]
11. Baccetti T, Franchi L, McNamara JA Jr. The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopaedics. Semin Orthod. 2005;11(3):119-29 [ Links ]
12. Nolla, CM. The development of permanent teeth. J Dent Child. 1960;27:254-66 [ Links ]
13. Krailassiri S, Anuwongnukroh N, Dechkunakorn S. Relationships between dental calcification stages and skeletal maturity indicators in Thai individuals. Angle Orthod. 2002;72(2):155-66 [ Links ]
14. Uysal T, Sari Z, Ramoglu SI, Basciftci FA. Relationships between dental and skeletal maturity in Turkish subjects. Angle Orthod. 2004;74(5):657-64 [ Links ]
15. Basaran G, Ozer T, Hamamci N. Cervical vertebral and dental maturity in Turkish subjects. Am J Orthod Dentofacial Orthop. 2007;131(4):447.e13-20 [ Links ]
16. Rózyfo-Kalinowska I, Kolasa-Raczka A, Kalinowski P. Relationship between dental age according to Demirjian and cervical vertebrae maturity in Polish children. Eur J Orthod. 2011;33(1):75-83 [ Links ]
17. Osman F, Scully C, Dowell TB, Davies RM. Use of panoramic radiographs in general dental practice in England. Community Dent Oral Epidemiol. 1986;14(1):8-9 [ Links ]
18. Maeda N, Hosoki H, Yoshida M, Suito H, Honda E. Dental students' levels of understanding normal panoramic anatomy. J Dent Sci. 2018;13(4):374-77 [ Links ]
19. Tanna NK, AlMuzaini AAAY Mupparapu M. Imaging in Orthodontics. Dent Clin North Am. 2021;65(3):623-41 [ Links ]
20. Bonett DG, Wright TA. Sample size requirements for estimating Pearson, Kendall and Spearman correlation. Psychometrika. 2000;65:23-8 [ Links ]
21. Paschoini VL, Nunes DC, Matias M, Nahás-Scocate ACR, Feres MFN. Accuracy of dental calcification stages for the identification of craniofacial pubertal growth spurt: proposal of referral parameters. Eur Arch Paediatr Dent. 2023;24(1):75-83 [ Links ]
22. Litsas G, Ari-Demirkaya A. Growth indicators in orthodontic patients. Part 1: comparison of cervical vertebral maturation and hand-wrist skeletal maturation. Eur J Paediatr Dent. 2010;11(4):171-5 [ Links ]
23. Wong RW, Alkhal HA, Rabie AB. Use of cervical vertebral maturation to determine skeletal age. Am J Orthod Dentofacial Orthop. 2009;136(4):484.e1-6 [ Links ]
24. McNamara JA Jr, Franchi L. The cervical vertebral maturation method: A user's guide. Angle Orthod. 2018;88(2):133-43 [ Links ]
25. Perinetti G, Contardo L, Gabrieli P, Baccetti T, Di Lenarda R. Diagnostic performance of dental maturity for identification of skeletal maturation phase. Eur J Orthod. 2012;34(4):487-92 [ Links ]
26. Demirjian A, Goldstein H, Tanner JM. A new system of dental age assessment. Hum Biol. 1973;45(2):211-27 [ Links ]
27. Engströrn C, Engström H, Sagne S. Lower third molar development in relation to skeletal maturity and chronological age. Angle Orthod. 1983;53(2):97-106 [ Links ]
28. Petrie A, Sabin C. Medical statistics at a glance, 4thed. Oxford: Blackwell Publishing, UK, 2019:119-23 [ Links ]
29. Cericato GO, Franco A, Bittencourt MA, Nunes MA, Paranhos LR. Correlating skeletal and dental developmental stages using radiographic parameters. J Forensic Leg Med. 2016;42:13-8 [ Links ]
30. Valizadeh S, Eil N, Ehsani S, Bakhshandeh H. Correlation between dental and cervical vertebral maturation in Iranian females. Iran J Radiol. 2012;10(1):1-7 [ Links ]
31. Bittencourt MV, Cericato G, Franco A, Girão R, Lima APB, Paranhos L. Accuracy of dental development for estimating the pubertal growth spurt in comparison to skeletal development: a systematic review and meta-analysis. Dentomaxillofac Radiol. 2018;47(4):20170362 [ Links ]
32. Lecca-Morales RM, Carruitero MJ. Relationship between dental calcification and skeletal maturation in a Peruvian sample. Dental Press J Orthod. 2017;22(3):89-96 [ Links ]
33. Uys A, Bernitz H, Pretorius S, Steyn M. Estimating age and the probability of being at least 18 years of age using third molars: a comparison between Black and White individuals living in South Africa. Int J Legal Med. 2018;132(5):1437-46 [ Links ]
34. Deeks JJ, Altman DG. Diagnostic tests 4: likelihood ratios. BMJ. 2004;17;329(7458):168-9 [ Links ]
35. Kumar S, Singla A, Sharma R, Virdi MS, Anupam A, Mittal B. Skeletal maturation evaluation using mandibular second molar calcification stages. Angle Orthod. 2012;82(3):501-6 [ Links ]
36. Oyonarte R, Sánchez-Ugarte F, Montt J, Cisternas A, Morales-Huber R, Ramirez-Lobos V, Janson G. Diagnostic assessment of tooth maturation of the mandibular second molars as a skeletal maturation indicator: A retrospective longitudinal study. Am J Orthod Dentofacial Orthop. 2020;158(3):383-90 [ Links ]
 Correspondence:
Correspondence:
Dr R Opperman
Tel: +27 12 521 4854
Email: rozanneopperman@gmail.com
Author's contribution
1. Rozanne Opperman 60%
2. Peter Sethusa 30%
3. Dikeledi Letsholo 10%


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}