










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.78 n.5 Johannesburg Jun. 2023
http://dx.doi.org/10.17159/sadj.v78i05.16871
RADIOLOGY CORNER
Lené MerboldI; Chané SmitII; André UysIII
IBChD, PGDipDent (Radiology), MSc (Maxillofacial Radiology). Department of Oral and Maxillofacial Pathology, School of Dentistry, Faculty of Health Sciences, University of Pretoria, South Africa. ORCID: 0000-0003-4041-127X
IIBChD, MSc (Maxillofacial Radiology). Department of Oral and Maxillofacial Pathology, School of Dentistry, Faculty of Health Sciences, University of Pretoria, South Africa. ORCID: 0000-0003-4047-6356
IIIBSc, BChD, PGDipDent, MSc (Maxillofacial Radiology), PhD (Anatomy). Department of Anatomy, School of Medicine, Faculty of Health Sciences, University of Pretoria, South Africa. ORCID: 0000-0001-8250-7662
CASE
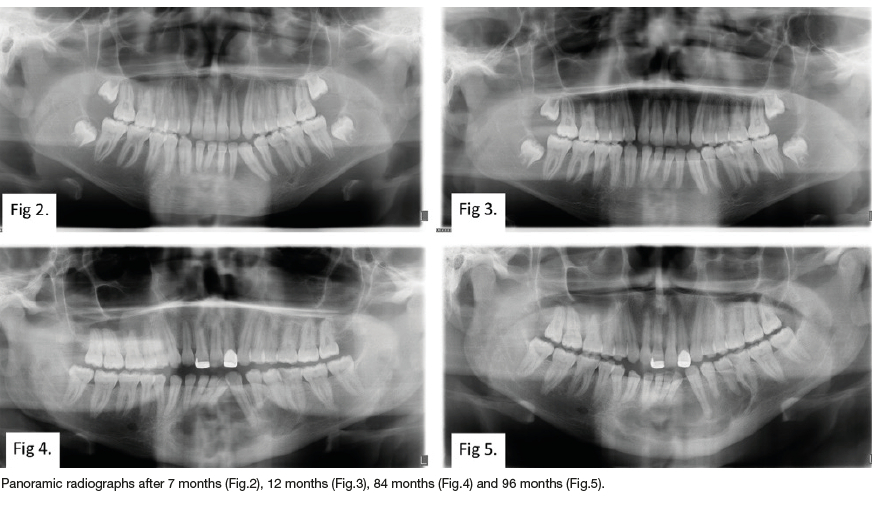
A 13-year-old male patient presented with a painless expansile swelling of the anterior mandible. Radiographic examination showed a unilocular radiolucent lesion resulting in bony expansion and teeth displacement (Figure 1). The lesion was biopsied and histological examination showed a conventional ameloblastoma. The lesion was marsupialised and was followed up over a period of 96 months (Figure 2-5). Subsequent signs of bone All and absence of the lesion was noted for the follow-up period of 12 months (Figure 3). The lesion, however, recurred after 68 months with greater amounts of expansion compared to the initial presentation (Figure 4, 5).
INTERPRETATION
Ameloblastoma (AB) is a benign odontogenic neoplasm arising from epithelial remnants of the dental lamina. ABs can be roughly divided into conventional and unicystic variants. Unicystic ABs present as a unilocular radiolucency on radiographic examination. Conventional ABs can appear as either uni- or multilocular radiolucent lesions.
The treatment of AB is controversial. There are two main surgical approaches, conservative and radical. The former involves marsupialisation/enucleation/curettage of the bony cavity, while radical surgery includes surgical resection with 1-2cm clear bony margins. The margin marked for resection is defined as the distance from the radiologic margin predicted to be disease-free. This is suggested due to the bony infiltration of neoplastic cells beyond the radiologic margins.
The luminal and intraluminal histological variants of unicystic ABs may be managed with conservative treatment. However, due to tumour infiltration beyond the radiological margins in mural unicystic and conventional ABs, treatment of choice is radical-wide surgical excision.
Patients who receive conservative treatment for conventional ABs have a higher propensity for recurrence (90%) than those who receive radical treatment (5%). Post-operative follow-up for all AB cases is critical as more than 50% of recurrences can occur five years post-treatment, with some presenting as early as two years after surgical intervention.
The current case highlights that histological diagnosis and subtyping is essential before the initiation of treatment.
Marsupialisation and enucleation of conventional ABs result in remnants of neoplastic cells even in the absence of radiological signs of disease. Due to the high recurrence rates and the possibility of malignant transformation, resection is advocated for conventional ABs.
Conflict of interest
All authors have indicated they have no potential conflict of interest and no financial relationships relevant to this article to disclose.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Ethics
The study was conducted following approval by the Faculty of Health Sciences Research Ethics Committee, University of Pretoria (571/2021). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. This article does not contain any studies with animal subjects performed by any of the authors.
REFERENCES
1. El-Naggar AK et al. World Health Organization Classification of Head and Neck Tumours. 4th ed. 2017 [ Links ]
2. De Santana Santos T, Piva MR, De Souza Andrade ES, Vajgel A, De Holanda Vasconcelos RJ, Martins-Filho PRS. Ameloblastoma in the Northeast region of Brazil: A review of 112 cases. Journal of Oral and Maxillofacial Pathology. 2014;18:66-71 [ Links ]
3. McClary AC, West RB, McClary AC, Pollack JR, Fischbein NJ, Holsinger CF, et al. Ameloblastoma: a clinical review and trends in management. European Archives of Oto-Rhino-Laryngology. Springer Berlin Heidelberg; 2016;273:1649-61 [ Links ]
4. Mendenhall WM, Werning JW, Fernandes R, Malyapa RS, Mendenhall NP. Ameloblastoma. American Journal of Clinical Oncology: Cancer Clinical Trials. 2007;30:645-8 [ Links ]
5. Li Y Han B, Li LJ. Prognostic and proliferative evaluation of ameloblastoma based on radiographic boundary. Int J Oral Sci. 2012;4:30-3 [ Links ]
6. Gardner DG. A pathologist's approach to the treatment of ameloblastoma. J Oral Maxillofac Surg. 1984 Mar;42(3):161-6. doi: 10.1016/s0278-2391(84)80026-9 [ Links ]
7. Hong J, Yun PY Chung IH, Myoung H, Suh JD, Seo BM, et al. Long-term follow up on recurrence of 305 ameloblastoma cases. Int J Oral Maxillofac Surg. 2007;36:283-8 [ Links ]
8. Milman T, Ying GS, Pan W, LiVolsi V Ameloblastoma: 25 Year Experience at a Single Institution. Head Neck Pathol. Springer US; 2016;10:513-20 [ Links ]
 Correspondence:
Correspondence:
Name: Lené Merbold
Tel: 0123192311
Email: lmerbold@gmail.com
Author's contribution
1 . Lené Merbold Primary author 50%
2 . Chané Nel Primary author 30%
3 . André Uys Secondary author 20%


{kind=link}
{kind=link}