










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Dental Journal
versión On-line ISSN 0375-1562
versión impresa ISSN 0011-8516
S. Afr. dent. j. vol.78 no.5 Johannesburg jun. 2023
http://dx.doi.org/10.17159/sadi.v78i05.16852
CASE REPORT
Retrieval of displaced dental implant in maxillary sinus by modified Caldwell Luc technique
Kruttika BhuseI; Tanay V ChaubalII; Ranjeet BapatIII
I.M.D.S (Periodontology and Oral Implantology) Affiliation: Private Practice, Houston, Texas, United States of America
IIM.D.S. (Periodontology and Oral Implantology) Division of Restorative Dentistry, School of Dentistry, International Medical University, 126, Jln Jalil Perkasa 19, Bukit Jalil, Kuala Lumpur, MY, 57000
IIIM.D.S. (Periodontology and Oral Implantology) Division of Restorative Dentistry, School of Dentistry, International Medical University, 126, Jln Jalil Perkasa 19, Bukit Jalil, Kuala Lumpur, MY, 57000
ABSTRACT
Displacement of dental implants into the maxillary sinus is an uncommon complication during implant placement. Here we present a case report of retrieval of dental implant displaced in the maxillary sinus with modification of Caldwell-Luc technique.
A 35-year-old man presented to our institution for replacement of the maxillary right first molar using dental implant. At the point of final tightening of the implant, it suddenly got displaced into the maxillary sinus. The displaced dental implant was retrieved by performing a modification of the Caldwell-Luc technique which utilises gravitational force, saline as a vehicle and a tight-fitting suction tip in the surgically created lateral window. He was also instructed in coughing and sneezing techniques. Medical and dental professionals can utilise this technique effectively when advanced equipment such as endoscopes are not available to retrieve dental implants displaced in the maxillary sinus and it also preserves significant amount of alveolar bone in comparison to the traditional Caldwell-Luc technique.
Keywords: Dental implants, maxillary sinus, modified Caldwell-Luc.
INTRODUCTION
The use of dental implants for replacement of missing teeth has become a mainstay in contemporary dental practice. Success of implant therapy depends on various factors, one being the quality and quantity of residual alveolar bone required; it is often inadequate in the posterior maxilla due to pneumatisation of the maxillary sinuses.1 Inadequate bone may be augmented by performing sinus lift procedures for dental implant placement.
During these procedures complications such as perforation of the sinus membrane, bleeding from the sinus cavity and displacement of implants into the maxillary sinus may arise.2 Displacement of dental implants into the maxillary sinus may lead to postoperative sinus infection.3,4 There are three methods available for retrieving displaced dental implants in the maxillary sinus: the Caldwell-Luc technique, the endoscopic method and modification of the Caldwell-Luc method.5,6 Here we present a case report of retrieval of a dental implant with this modification of the Caldwell-Luc technique.
Case description
A 35-year-old man reported to the dental office for replacement of the missing maxillary right first molar using dental implant. Preoperative cone beam computed tomography analysis revealed bone width of 5.5mm and height of 9mm with fine trabecular bone of density 200 HU (Misch bone density classification). The patient was systemically healthy with healthy periodontal condition and adequate oral hygiene. Prior to the implant placement procedure informed written consent was obtained from the patient. Local anesthesia in the form of buccal infiltration and greater palatine nerve block on the palatal aspect was administered with 2% lignocaine HCl and 1:80,000 adrenaline (ICPA health products, Mumbai, India). Following a crestal incision, a full thickness mucoperiosteal flap was elevated. A sequential undersized osteotomy was prepared with the final drill being 3.2mm x 8mm. An implant of size 3.75mm in width x 8mm in height (AlphaBio, Petach Tikva, Israel) was introduced into the osteotomy with the help of a fixture driver and torqued up to 30Ncm with a torque wrench. At the point when the implant got completely seated a quarter turn was given with the torque wrench and suddenly the implant got displaced into the maxillary sinus. Immediate aspiration attempts to retrieve the implant were unsuccessful. Multiple periapical radiographs showed that the implant kept changing its location with change in head position.
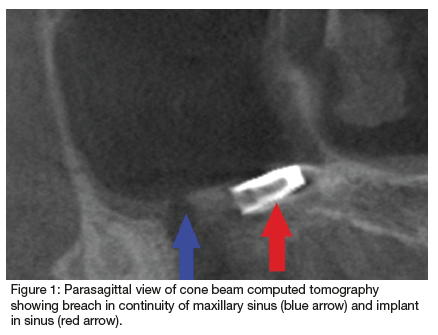
The osteotomy was then expanded to 6mm for further aspiration of the dental implant through the crestal osteotomy but the retrieval attempt failed. Parasagittal view of cone beam computed tomography revealed breach in the continuity of the maxillary sinus with the implant oriented towards the anterior wall of the maxillary sinus (Figure 1). The final position of the implant appeared to be in the anterior wall of the maxillary sinus. A modified
Caldwell-Luc approach was used wherein a round lateral maxillary osseous window was created into the sinus with the help of No. 8 diamond bur (Figure 2). A sterile plastic surgical suction tip was cut to fit exactly into the lateral osseous window and subsequently the sinus was filled with sterile saline via a 60ml syringe through the lateral window with the osteotomy blocked tightly with a sterile cotton pledget to facilitate one outlet for the implant; that is, through the lateral osseous window. Gravitational force was considered by placing the patient reclined on his right side, in the right lateral recumbent position so that the sinus was located on the underside. With the patient in this position the suction tip was introduced into the lateral window and then slowly withdrawn. The implant suddenly appeared through the window with the flow of saline. It was grasped with an Adson forceps (Salvin, Charlotte, NC, USA) and retrieved (Figure 3). The osteotomies were then covered with a resorbable collagen membrane (Biomend, Zimmer Dental, Warsaw, Ind, USA) and primary watertight closure was obtained with 4-0 mersilk suture material. Bone grafting was not performed because there was no intact sinus lining to contain the graft. The patient was prescribed an antibiotic (Amoxycillin 500mg) every 8 hours for 5 days, anti-inflammatory (Ketorolac 10mg) every 12 hours for 5 days and 0.12% chlorhexidine oral rinse for 2 weeks postsurgery. He was also instructed in coughing and sneezing
techniques. The patient was instructed to open his mouth during coughing to avoid any nasal-antral pressure that might disturb the oral-antral closure. Eight months later he reported no residual symptoms.
DISCUSSION
Maxillary sinuses are located bilaterally in the maxilla with an ostium for drainage which in the majority of the cases is in the superior portion of the medial wall and usually it drains into the middle meatus of the nose. Sinus drainage is accomplished by action of cilia and small foreign bodies are easily removed by this ciliary action. A foreign body as large as a dental implant is too large to be evacuated by this natural phenomenon. The average volume of a maxillary sinus is about 15ml (range between 4.5 and 35.2ml) so a lavage of 25-30ml saline can easily be performed of the maxillary sinus.
Dental implants displaced into the maxillary sinuses have a propensity to get infected.7 The bone in our case was not adequate to resist the implant advancement at the implant's fully seated position with the bone quality being fine trabecular. Immediate retrieval of the implant was performed in our case as delaying the retrieval could allow the implant to migrate into an adjacent contiguous sinus.8 There was one reported case in which the displaced dental implant migrated from a maxillary sinus to a sphenoid sinus due to delayed retrieval.9
The technique presented here utilises gravitational force, saline as a vehicle, tight-fitting suction tip in the surgically created lateral window and blockage of the crestal implant osteotomy which forces the implant only through the lateral window. This modified Caldwell-Luc technique preserves more bone by creating a smaller lateral window; also, the location of the window is more inferior to that of the traditional Caldwell-Luc which further aids in retrieving the displaced implant. The diameter of the window should be larger than the diameter of the displaced dental implant, taking care to prevent any damage to adjacent tooth roots. The use of this technique is a cost-effective way for management of the displaced dental implant in the sinus especially in dental operatories and countries where there is lack of sophisticated and expensive armamentarium such as an endoscope.
CONCLUSION
Although dental implants have become one of the predictable methods of teeth replacement, unavoidable complications during or after implant placement might occur. Clinicians should take all the necessary precautions to avoid untoward complications and still be prepared to manage complications should they arise. The present case report emphasises the management of displacement of the dental implant into the maxillary sinus in a cost-effective way.
Source of financial support or funding
None
Conflict of interest
None
Acknowledgement
None
REFERENCES
1. Hollinshead WH. The nose and paranasal sinuses. In: Hollinshead WH, editor Anatomy for Surgeons: The Head and Neck. Philadelphia: Lippincott Williams and Wilkins; 1982: 259-63 [ Links ]
2. Annibali S, Ripari MLA, Monaca G, Tonoli F, Cristalli MP. Local complications in dental implant surgery: prevention and treatment. Oral Implantol (Rome). 2008; 1: 21-33 [ Links ]
3. Cordioli G, Mazzocco C, Schepers E, Brugnolo E, Majzoub 3. Z. Maxillary sinus floor augmentation using bioactive glass granules and autogenous bone with simultaneous implant placement. Clinical and histological findings. Clin Oral Implants Res. 2001; 12: 270-8 [ Links ]
4. Van den Bergj JP, Ten Ruggenkate CM, Disch FJ, Tuinzing DB. Anatomical aspects of sinus floor elevations. Clin Oral Implants Res. 2000; 11: 256-65 [ Links ]
5. Nakamura N, Mitsuyasu T, Ohishi M. Endoscopic removal of a dental implant displaced into the maxillary sinus: technical note. Int J Oral Maxillofac Surg. 2004; 33: 195-7 [ Links ]
6. Dennis Flanagan. A method to retrieve a displaced dental implant from the maxillary sinus. J Oral Implantol. 2009; 35: 70-4 [ Links ]
7. Thevoz F, Arza A, Jaques B. Dental foreign body sinusitis. Schweiz Med Wochenschr Suppl. 2000; 125: 30S-4S [ Links ]
8. Guler N, Delilbasi C. Ectopic dental implants in the maxillary sinus. Quintessence Int. 2007; 38: 238-9 [ Links ]
9. Felisati G, Lozza P, Chiapasco M, Borloni R. Endoscopic removal of an unusual foreign body in the sphenoid sinus: an oral implant. Clin Oral Implants Res. 2007; 18: 776-80 [ Links ]
 Correspondence:
Correspondence:
Dr. Tanay V Chaubal,
Division of Restorative Dentistry, School of Dentistry
International Medical University, 126, Jln Jalil Perkasa 19
Bukit Jalil, Kuala Lumpur, MY, 57000.
Tel: +60142398279
E-mail: tanayvc@gmail.com


{kind=link}
{kind=link}