










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Dental Journal
versión On-line ISSN 0375-1562
versión impresa ISSN 0011-8516
S. Afr. dent. j. vol.78 no.5 Johannesburg jun. 2023
http://dx.doi.org/10.17159/sadj.v78i05.16887
RESEARCH
Final-year oral hygiene and dental therapy students' perceptions of teaching and learning at a South African university
H PillayI; R MoodleyII
IBChD, MMedSc, Discipline of Dentistry, University of KwaZulu-Natal. ORCID: https://orcid.org/0009-0001-7455-5506
IIPhD, Senior Lecturer, Discipline of Dentistry, University of KwaZulu-Natal. ORCID: https://orcid.org/0000-0003-2703-9370
ABSTRACT
INTRODUCTION: Dental students may provide insightful course evaluation and feedback due to their direct engagement with theoretical.
and clinical instruction during their training. According to the literature, student feedback may enhance dental education. This study investigated students' perceptions of teaching and learning, the various aspects of which will be discussed further.
AIMS AND OBJECTIVES: The study aimed to determine the perceptions of the final-year dental therapy and oral hygiene students regarding teaching and learning at a South African university. Topics such as teaching methods, suitable attributes of academic staff, potential barriers to learning, clinical quotas, effects of the pandemic and recommendations to enhance teaching and learning were investigated.
METHODS: A cross-sectional study was conducted during the 2021 and 2022 academic years. Quantitative and qualitative data was captured via an online questionnaire. Participants were asked to rate their perceptions of teaching and learning via a five-point Likert scale and respond to open-ended questions.
RESULTS: Sixty-nine students participated in this study, yielding a response rate of 65.09%. The findings demonstrated students' preference for contact teaching methods such as clinical observation (80%; n=55) and clinical demonstrations (78%; n=54) compared to online lectures (54%; n=37). Stress (78%; n=54) and insufficient feedback (88%; n=61) were identified as learning barriers. Increased clinical training was among the suggestions to enhance learning.
CONCLUSION: Students should be encouraged to provide feedback regarding teaching and learning as this may positively influence curriculum design and development.
Keywords: Dental education, teaching and learning, dental students, oral hygiene, dental therapy, teaching methods, academic staff attributes, clinical supervision, clinical quotas, barriers to teaching and learning.
INTRODUCTION
Despite undergoing various changes throughout the decades, most recently due to the COVID-19 pandemic, dental education has strived to produce proficient dental professionals. Dental curricula characteristically consist of three aspects1, one of which is the delivery of theoretical content via various didactic teaching methods such as lectures, tutorials and problem- and case-based learning.2 Preclinical training is usually conducted through simulations and other technologically-advanced techniques before clinical training.2 The latter prepares students for the responsibilities, procedures and working environment they will encounter as professionals. It also enables students to develop further and refine their clinical skills. Globally, this aspect of training was most adversely affected by the pandemic as dental institutions in the US, Australia, Japan and Switzerland, among others, temporarily postponed all clinical activities.1,3
The role of the student within a dental institution is no longer regarded as that of a passive learner. The existing literature describes the valuable insight and feedback that students may provide regarding their educational experiences, personal interactions and involvement with the course content.4,5 This vital information may significantly influence an institution's assessment principles, curriculum review and development, and also provide quality assurance. Students' perceptions of teaching methods, modules and clinical training, among others, may assist in identifying institutional successes and challenges. The feedback can also potentially incite changes and encourage renewed dental education strategies.6,7
At the study site, the Dental Therapy and Oral Hygiene programmes are accredited by the Health Professions Council of South Africa (HPCSA) on a five-yearly basis. As part of this process, feedback is obtained from the students, and quality assurance is maintained. The latter is also monitored by the quality assurance unit at the institution.
Students' perceptions of teaching and learning may be influenced by the educational environment which, as cited by Bhayat et al. (2018), includes the infrastructure of an institution, clinical activities, clinical supervision and the atmosphere that is created by staff and students.8 Academic staff may be involved in training either as a lecturer, clinical supervisor or both. While the primary role of such an individual is to facilitate learning effectively, staff may also use the opportunity to instil positive attributes and values in students.
The pandemic introduced unprecedented challenges for students and academic institutions. Several dental schools implemented online learning to deliver course content.1,9 Other institutions implemented a hybrid learning model, combining online learning with preclinical and clinical contact teaching.10 While e-learning ensured that teaching and learning continued, several associated challenges have been reported in the literature.10-12 In addition, the changing curriculum and implementation of home-based learning meant that students were required to adapt to a new environment and adopt new learning strategies. Previous perception-based studies identified various barriers that affected learning, such as graded assessments13,14, the limited number and availability of clinical staff13, and the dissociation between theory and clinical training.15
This mixed-methods study aimed to determine dental therapy and oral hygiene students' perceptions of teaching and learning, at the respective training site, via an online questionnaire. The results of this study may contribute to the current understanding of students' preferences, challenges and suggestions to enhance dental education.
METHODS
Research setting and context
This study was conducted at a South African dental school. The Social Sciences and Humanities Ethics Committee granted ethical approval (HSSREC/00002902/2021). Gatekeeper permission was received from the registrar of the university.
Research design
A mixed-methods study was conducted during the 2021 and 2022 academic years. An online questionnaire consisting of open and closed-ended questions enabled the collection of quantitative and qualitative data. Students rated their perceptions of teaching and learning via a five-point Likert scale. For section 1, participants were requested to rate the influence of various teaching methods on their academic performance from 1 to 5, which represented "least influence" to "most influence" respectively. The remaining sections, namely characteristics of a lecturer, clinical supervision, barriers to learning and clinical quotas, required a rating of 1-5 which represented "strongly disagree" to "strongly agree" respectively. The open-ended questions related to the effects of the pandemic, strategies that may enable continued learning and recommendations to enhance teaching and learning. In 2021, a pilot study was conducted among nine second-year dental therapy students. The participants successfully completed the questionnaires on Google forms and clearly understood the various sections.
Participants
All final-year dental therapy and oral hygiene students (n=106) were invited to participate in the cross-sectional study, of which (n=69) agreed. Participants consisted of three cohorts: the dental therapy classes of 2021 and 2022 and the oral hygiene class of 2022. The oral hygiene class of 2022 were the first graduates of the restructured programme, which is currently being offered as a degree at the study site.
Data collection and analysis
Data was collected between August 2021 and September 2022. An information sheet and consent form were made available to all students. All participating students consented to their involvement in the study. Anonymity was maintained throughout the study as participant names were not requested.
An online questionnaire on Google forms was accessed via a link. Quantitative and qualitative data were analysed using statistical and thematic methods, respectively.
RESULTS
Demographic details
The mean age of participants was 21 years old. The participants' ages ranged from 19 to 25 years old, most of whom were 20 years old (39%; n=27).
Most participants were female (71%; n=49), followed by males (28%; n=19) and 1% (n=1) who preferred not to disclose their gender.
According to the Kruskal-Wallis tests, which were conducted to investigate the relationship between each student cohort and the various sections of the questionnaire, no statistically significant associations were reported except that the oral hygiene students preferred digital notes compared to handwritten notes (p=0.05).
Perceptions of teaching methods
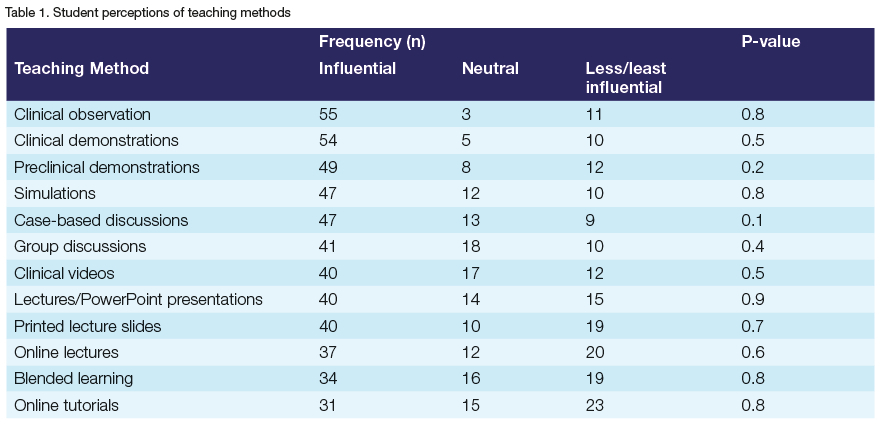
Participants were asked to rate the influence of various teaching methods on their academic performance via a five-point Likert scale. To represent the data in Table 1, the frequencies of responses were combined for the most and least influential teaching methods. More than 50% of the participants (57%; n=39) regarded preclinical demonstrations as the "most influential" teaching method. The teaching method with the overall highest rating was the clinical observation of a supervisor (80%; n=55). According to the participants, online tutorials (33%; n=23), online lectures (29%; n=20) and blended learning (28%; n=19) had the least influence on academic performance.
Suitable attributes of a lecturer
Participants were presented with various statements regarding the attributes of a lecturer and requested to rate their perceptions of each one. Respondents strongly agreed that a lecturer should be organised (81%; n=56), allow students to ask questions during or after a lecture (78%; n=54), present content interestingly and engagingly (83%; n=57), and promote student interaction in class (68%; n=47). Most participants believed that learning was enhanced when a lecturer possessed a wide range of knowledge (77%; n=53) and considered rapport between a student and lecturer to be important (75%; n=52).
Clinical supervision
Participants rated several statements relating to clinical supervision. Most participants strongly agreed that a clinical supervisor should be enthusiastic (72%; n=50), available when required by the students (68%; n=47) and possess good interpersonal/communication skills (77%; n=53). Participants also strongly agreed that a supervisor with good clinical skills motivated students to be better clinicians (77%; n=53) and that effective learning occurred by regarding the supervisor as a role model (59%; n=41).
Students were also strongly in favour of assessing clinical performance according to objective assessment standards (71%; n=49) and receiving constructive feedback about their clinical performance (74%; n=51).
Potential barriers to teaching and learning
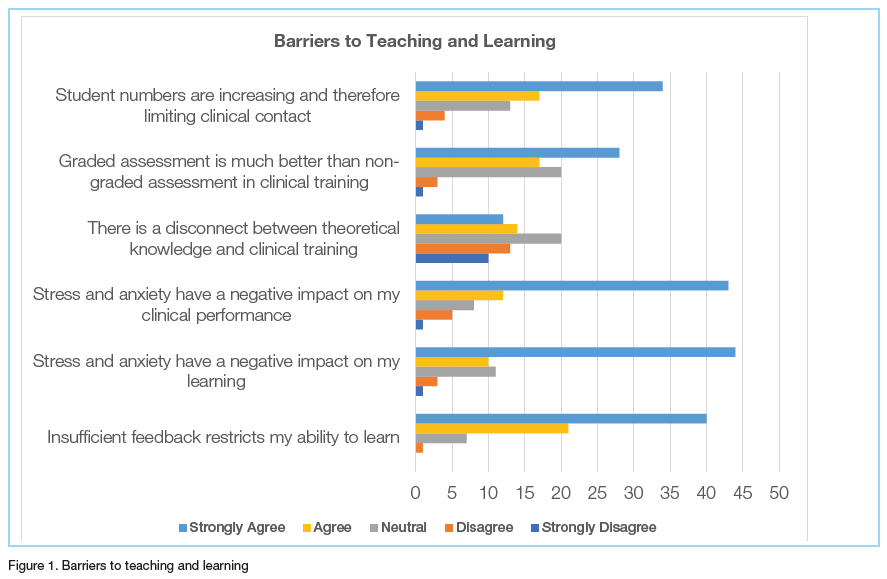
Students were requested to rate their perceptions of potential barriers to learning (Figure 1). Participants agreed that insufficient feedback restricted their learning (88%; n=61). Stress was reported as a hinderance to students' learning (78%, n=54) and clinical performance (80%, n=55). Only 38% (n=26) of participants reported a disconnect between theoretical knowledge and clinical training. More than half of the oral hygiene participants (55%; n=6) remained neutral. Participants preferred graded to non-graded continuous assessments (65%; n=45) and agreed that increased student numbers limited clinical contact (74%; n=51).
Regarding various statements concerning e-learning, 77% (n=53) of participants had access to a computer or laptop, while 62% (n=43) had access to data or the internet. Most participants did not encounter difficulties with the e-learning website (61%; n=42). Students preferred written/printed notes compared to digital notes (54%; n=37), although 55% (n=6) of the oral hygiene students disagreed with this statement (p=0.05).
Clinical quotas
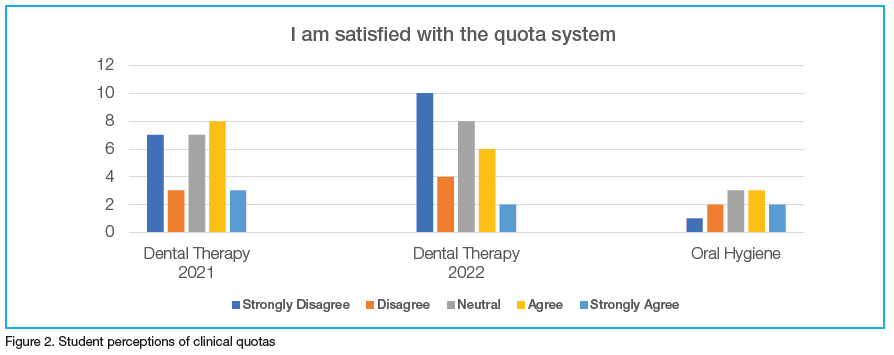
The final section required participants to rate their satisfaction with the clinical quota system (Figure 2). In compliance with the course requirements, a minimum number of procedures, or quotas, were to be completed by students. In contrast to the other sections of the questionnaire, various opinions were reported. Participants were generally unsatisfied with the quota system (39%; n=27) compared to 35% (n=24), who were satisfied and 26% (n=18) who remained neutral.
Qualitative data analysis
Open-ended questions formed part of the questionnaire, enabling further insight into students' perceptions of teaching and learning. The results were analysed using thematic analysis. Questions 1-7 appear with participants' supporting quotes.
Question 1: What is the best method to deliver theoretical knowledge to students and why?
Participants favoured contact lectures as this teaching method provided a distinct understanding of content, enabled students to focus on the lecture content, and promoted student-lecturer engagement.
"It's easy to understand. Whenever something isn't clear, you are able to ask questions and ... revise your work with full understanding." (P32)
"It is easier to focus and understand a person when seeing them live compared to a screen." (P51)
"Lectures (are) more personal and interactive." (P21)
". it gives learners the information that they are looking for, without any external interruptions such as connection issues you get during loadshedding with online learning." (P38)
Demonstrations were regarded to be effective as students were able to grasp and retain knowledge easily. Students also supported group and case-based discussions.
"Demonstrations on the topic discussed also help in better understanding as students have different learning methods." (P65)
"Allows us to use our minds in an environment where it is easy to remember." (P47)
"I understand the theory better when I am doing the practicals and discussing case studies." (P18)
Videos were considered to enhance learning by providing a visual representation of the notes. "I engage better with my work when it is taught using this approach. Audiovisual aids help a lot in the learning process rather than simply reading off lecture slides." (P27)
"They better explain or demonstrate what we have learnt and make it easier to understand the notes and what exactly is expected from me as a student." (P30)
Question 2: In your opinion, what are the characteristics of a suitable lecturer?
Students were in favour of a lecturer who encouraged interactive learning.
"A good lecturer allows students to express their opinions and ask questions." (P30)
Participants also valued attributes such as being supportive and understanding.
"A good lecturer for me is someone who's understanding ... someone who's able to take the concerns of learners into consideration, not for him/her to dismiss them easily without even looking into the matter." (P64)
"Being... understanding to the different circumstances that the students may be faced with." (P38)
Punctuality and organisation were also regarded as important attributes of a lecturer.
"A good lecturer is well organised, manage(s) time very well." (P24)
According to participants, an approachable lecturer created an environment that promoted learning.
"He/she is one who is friendly kind and approachable. Having that kind of a lecturer provides a comfortable space, and teaching and learning becomes easier." (P55)
"One who is easy to ask if you have questions or need clarity We shouldn't be afraid to ask. The environment should be free, so we can engage." (P3)
Participants favoured a knowledgeable lecturer who was capable of teaching and sharing their knowledge.
"A person who is knowledgeable and is able to teach and share their knowledge with others." (P39)
"A teacher who shows interest... efficient teaching skills ... strong knowledge." (P67)
Question 3: What are the factors that hinder your learning?
Participants reported several barriers that affected clinical training, such as a limited number of patients, inadequate clinical training time and clinical sessions, quality and delivery of feedback, and increased student enrolment.
"Limited numbers of patients in the clinic." (P14)
"Time constraints in the clinical setting." (P28)
"Not enough exposure to clinical training." (P59)
"Lack of academic feedback." (P63)
"Getting criticised about my work instead of being advised on how to do it right and correct my mistakes." (P65)
Not being equally exposed to clinical sessions because of the increase in student numbers." (P2)
Stress, anxiety and depression were also reported as barriers by the study participants. Stress was most associated with the clinical setting and workload.
"Sometimes the environment at the clinic is too stressful for learning." (P24)
"Too much work at once produces too much anxiety and stress, which makes me unable to cope with school." (P30)
Students identified several barriers to e-learning, such as limited student-lecturer interaction and external factors, such as unstable internet connectivity or power outages.
"The interaction between lecturer and student is severely hindered due to the lack of engagement in e-learning." (P4)
"The Wi-Fi at my res is bad even though I've complained for three years, so I use the data that our university provides us with, but the network is bad, it's worse with loadshedding." (P18)
"Networkissues." (P59)
"Poor internet connectivity." (P30)
Question 4: Why are you satisfied, neutral or unsatisfied with regard to the clinical quota system?
Unsatisfied participants attributed their perceptions of the system to clinical barriers that hindered the achievement of their quotas.
"It increases stress for learners to see a certain number of patients just for a mark instead of working at our own pace and focusing on areas we think we need to do more in." (P22)
"With the restricted times in the clinic and the number of students and patients who don't show up for recalls or patients who have to be deferred due to complications, it is difficult to reach quotas." (P34)
"During certain days, some students leave the clinic without having seen a patient due to patient shortage, and only two days in a week of going to the hospital might not be sufficient in the achievement of all those quotas." (P55)
Participants who were satisfied with the clinical quotas reported that meeting the requirements assisted in their preparation for independent practice and acquiring clinical competency.
"It is only sensible to do so much as final year students. I understand we need to be fully prepared for the outside world and its demands." (P66)
"I think the given number . does make us competent at the end." (P64)
". I will get more exposure and experience regarding the clinical training process." (P33)
Students who expressed neutral views acknowledged the existing challenges and possible enhancements that could be made.
"The quotas are fair but very difficult to attain when we don't have enough working units and patients coming in." (P36)
"Only if they make sure that students see patients equally and fairly." (P53)
Question 5a: How has the pandemic affected how you approach learning?
A decrease in contact teaching and clinical training were observed during the pandemic.
"I didn't get much exposure to contact learning and other resources at campus." (P63)
"I have had too little exposure in terms of practical... My big worry is that when I go out there, I will be expected to know everything and do it perfectly despite me not having the adequate training and exposure." (P56)
Students' motivation to study was also affected during this time.
"Learning has become dreadful and exhausting." (P2)
"It has made my work ethic bad, I have trouble finding the motivation to learn or even go over work." (P7)
"I used to love learning, now it's a struggle, just about passing my assessments and getting this degree done." (P65)
Students reported the various ways in which they adapted to the challenges.
"I had to adapt to doing everything on the computer and attend online classes, which at first was very difficult, and I'd even fall asleep while attending." (P41)
"It made me realise things can change anytime and we need to be able to adapt in different situations." (P54)
"I learned to study hard and go an extra mile for all my modules because it all about theory now." (P14)
Question 5b: Which strategies can assist students in continuing their studies during such times?
According to participants, self-discipline and students' commitment to learning were essential in continuous learning.
"Dedication, prioritising school work and putting in the needed and required efforts in order to succeed." (P66)
"Self-discipline is key." (P49)
Interactive e-learning, tutorials and group discussions were identified as suitable teaching methods that would support continued learning.
"More interactive online learning." (P39) "Recorded lectures." (P36) "More tutorials." (P38)
"Have tutorial sessions besides from the lecture classes." (P55)
"... discussing clinical cases as groups." (P58)
'Vocal or (other) ways to allow students to interact as a group." (P57)
Participants favoured various types of non-graded assessments, which were supplemented with feedback from their lecturers.
"A lecturer can structure a default activity for learners to complete ... and mark it." (P4)
"After the students have participated in the lecture, they should be given quizzes every week on the work and given appropriate feedback." (P7)
"More self-assessment given to students so that they can understand more." (P6)
Question 6: How can clinical training be enhanced at your institution?
Participants reported that clinical training should be introduced at an earlier stage in the course.
"To be engaged in clinical work earlier in the degree." (P4)
"More training please... starting to extract teeth at third year is not okay. We need to start at least the second semester of the second year." (P53)
An increase in clinical sessions and exposure to patients was also suggested by participants.
"Giving students more clinical sessions." (P60)
"We need more practicals." (P17)
"Creating a system that will ensure each learner gets to see at least one patient a day" (P68)
"To be exposed to more patients so that we can get more clinical experience." (P65)
According to participants, the provision of robust feedback, an increase in the number of clinical supervisors and improved student-lecturer interaction were potential enhancements to teaching at the institution.
"Receive more feedback about my performance after clinical session." (P64)
"Supervisor that can give feedback in a well-mannered and constructive way, not just criticise." (P54)
"The ratio of supervisor to students should also be kept to a minimum to ensure adequate attention to each student." (P27)
"Having more clinical supervisors for the supervision of quite a number of students." (P55)
"By improving communication between students, lecturers and supervisors." (P67)
"Engage with students and know more about their challenges." (P37)
"Ensure that lecturers or supervisors are approachable so students can freely approach them instead of being afraid to do so." (P41)
Question 7: As a student, what suggestions or changes would you like to see being implemented to enhance your educational experiences?
Participants noted that an association should exist between theory and clinical training. Furthermore, students reported that the curriculum should include more practical training than theoretical content.
"Theory must correspond with clinical practice." (P56)
"To have more practical work than theory." (P24)
Blended learning was suggested as a teaching method to enhance students' educational experiences.
"Using both online and contact learning can help students in understanding their work." (P30)
"A blended approach to learning with both online and physical lessons is a less stressful way to learn." (P46)
Participants suggested a decrease in the number of quotas or a change to the existing system.
"... reduce clinical quotas." (P42)
"A more accommodative quotas system." (P38)
"...issue of quotas must be addressed because this degree is quota-driven." (P65)
DISCUSSION
Overall scores, as represented by Table 1, indicated that the largest frequency of participants regarded the clinical observation of a supervisor to be an influential teaching method. Students who participated in the study by Gerzina et al. (2005) regarded the observation of a clinical supervisor "as one of the best forms of clinical teaching".2 Most participants rated preclinical demonstrations as the "most influential" teaching method on their academic performance. The overall scores for section 1 of the questionnaire also revealed that participants favoured clinical demonstrations. The qualitative data of the current study supported students' preference for demonstrations and indicated that videos, case-based and group discussions were also associated with effective teaching. Despite the primary implementation of online learning during the pandemic, participants of the current study regarded online tutorials, online lectures and blended learning as the least influential teaching methods. The qualitative results of the current study further corroborated these findings, as almost half of the respondents favoured contact lectures in delivering theoretical knowledge. Similar results were observed by Bourzgui et al. (2020), as 53.8% of participants were in favour of face-to-face teaching.16 Noor et al. (2022) reported that 73.8% of participants in their study regarded contact teaching as a "better mode of learning" than e-learning.17 Quinn et al. (2020) concurred with these findings.18
Students valued the opportunity to ask questions and feel understood regarding their academic needs and challenges. Respondents of this study strongly agreed that class participation should be encouraged by a knowledgeable, organised, punctual and approachable lecturer. These attributes are also featured in the qualitative findings of this study. The lecturer's delivery of information was important to students of the current study. Participants also noted that the ability to teach and share knowledge were essential skills for the role. According to Hussein (2017), students identified attributes such as patience, approachability and enthusiasm in their own lecturers and regarded these as favourable.19
Most students regarded good interpersonal and communication skills, enthusiasm and availability as important attributes of a clinical supervisor. Learning was positively influenced by a supervisor who was regarded as a role model, and students were motivated by the demonstration of effective clinical skills by the supervisor. According to Ansary et al. (2011)4, students associate attributes such as commitment, good teaching skills, approachability, being knowledgeable and having a positive attitude with effective learning in a clinical environment. Schönwetter et al. (2006) identified seven ideal attributes of teaching, of which individual rapport, organisation and enthusiasm were most frequently associated with effective clinical and classroom teaching.20 Similar results were observed in the current study. Furthermore, both groups of participants valued fair assessments, insightful feedback and interactive learning where students were encouraged to participate and ask questions.
Participants were in support of constructive feedback concerning their clinical performance. Despite this, most students reported that learning was affected by insufficient feedback. The qualitative data supported this finding, as insufficient feedback and unconstructive criticism were considered barriers to learning. According to respondents of the current study, learning could be enhanced through consistent and constructive feedback that motivated students and helped them learn from their mistakes. Ansary et al. (2011) and Ebbeling et al. (2018) similarly observed students' support of feedback that was insightful, provided guidance and enabled them to identify improvements to their clinical performance.4,10 As cited in Nerali et al. (2021), inadequate and inconsistent feedback negatively affects learning.21-23 Ebbeling et al. (2018) reported students' concerns regarding the quality of feedback from their supervisors. The same authors cited studies by Anderson et al. (2011), Fugill (2005) and Henzi (2006), where dental students described clinical feedback as "sparse, non-useful or demeaning".10,24-26
In the clinical environment, students preferred graded rather than non-graded assessments. Furthermore, participants strongly supported using objective assessment standards to evaluate their clinical performance. In contrast to the results observed by Gerzina et al. (2005), students were neutral with regard to grading.2 Studies by Nerali et al. (2021) and Alves De Lima (2008) reported similar findings to the current study, where students preferred feedback that could be compared to "an established range of standards".21,28 A further finding of this study reported that inconsistent teaching among clinical supervisors hindered learning.
Stress and anxiety were considered barriers to learning and clinical performance. This finding was reflected in the quantitative and qualitative data of this study. According to students of the current study, stress resulted from negative encounters with clinical supervisors, the clinical environment, the required work volume and personal issues. Wilson et al. (2015) cited various studies that acknowledged the high incidence of stress among dental students due to possible causes such as "heavy workload", "challenging relationship with academic staff" and "the learning environment".28-42 Participants of the study by Wilson et al. (2015) regarded factors relating to the dental environment and theory as being more stressful than those relating to clinical aspects.28 These findings are in contrast to the current study.
The dental therapy students in this study reported that increased student numbers limited clinical exposure. The qualitative data confirmed this finding. A scoping review by McGleenon and Morison (2021) reported that dental schools across the UK raised concerns about increased student enrolment as the quality of training was negatively impacted by the unfavourable ratio of staff to students.43
Participants of the current study also expressed concerns regarding the limited clinical training and time to complete the course's practical aspect. This was attributed to various factors such as COVID-19, the insufficient number of clinical units, the inadequate number of functional dental chairs and the limited number of patients that presented for dental treatment. Current study participants stated that treatment was often deferred due to the patient's medical history and that recall appointments were often unattended. According to McGleenon and Morison (2021), dental schools across the UK experienced a scarcity of patients for various reasons, such as a lack of patient compliance and unpredictable appointments.43 McGleenon and Morison (2021) further noted that students' clinical experience was adversely affected by the limited number of patients.43
Most students had access to a computer/laptop and the internet/data. The majority of participants did not experience difficulties with the e-learning website. The most commonly reported barriers that students encountered were poor network and connectivity in addition to the Wi-Fi at students' residences, loadshedding and access to data. According to participants of the current study, e-learning negatively impacted interaction and communication between the lecturer and students. The study by Varvara et al. (2021) in Italy also expressed concerns regarding the "low-quality internet connections".9 A study conducted in Pakistan by Noor et al. (2022) reported that 77.7% of students strongly disagreed with the continued implementation of e-learning, possibly due to the absence of face-to-face engagement, impaired concentration over a prolonged period and "poor or interrupted internet connectivity".17 In contrast to this finding, a study by Mamattah (2016) in Ghana reported that students supported e-learning.44 An additional result of the current study is that most students prefer handwritten notes to digital notes on a screen.
The way students approached learning was significantly affected by the pandemic. Students adapted their learning style and became accustomed to online learning, assessments and electronic devices supporting this. However, the participants noted they no longer enjoyed learning and were unmotivated to study. Despite the challenges, several participants were encouraged to commit more to their studies and maximise their available time. Conversely, the losif et al. (2021) study in Romania reported that students' motivation remained "unaffected" during the pandemic.3 Students also reported a decrease in contact teaching, clinical training and the number of patients at the training site, which affected students' exposure to various procedures. Students' access to study materials, activities and resources on the main campus was also affected during this time.
Participants suggested strategies that may enable learning to continue under circumstances similar to the pandemic. The implementation of teaching methods such as e-learning, tutorials and group discussions was considered beneficial by the students. Participants also supported assessments such as quizzes and other activities in combination with feedback from their lecturers, all of which would help them evaluate what they understood. Respondents also identified the importance of their role in the continuation of learning by prioritising their studies, practising efficient time management and exercising self-discipline.
Most participants were unsatisfied with the clinical quota system. Various challenges influenced the attainment of quotas, including increased student numbers that limited patient access. Limited clinical training was a concern as students presented to the clinic twice a week and often did not treat a patient despite attending all the sessions. An insufficient number of patients presented for dental treatment, especially during the pandemic, and appointments were often not attended. Students also stated that they did not receive equal opportunities to treat patients, yet the number of quotas was standard for all students. Participants who were satisfied with the system reported that it enabled students to gain clinical experience in preparation for their professional careers. In pursuit of the quotas, students of the current study were encouraged to work hard and achieve a higher level of competence with each new procedure. Participants who expressed neutral views considered the quota system fair but acknowledged that various challenges, some of which were not within the control of students, affected whether the requirements would be met. McGleenon and Morison (2021) cited studies by Lynch et al. (2010), Davey et al. (2015), Clark et al. (2011) and Gilmour et al. (2016), which stated that students' clinical experience was limited in the absence of achieving minimum requirements.43-48
The participants of all three cohorts noted that increasing clinical training and re-introducing contact teaching, either in isolation or in combination with online learning, would benefit students. The dental therapy participants suggested that clinical training should be introduced earlier in the course rather than in the final year. According to Mullins et al. (2003), as cited by Gerzina et al. (2005), early exposure to the clinical environment benefits students as this aids in creating an association between basic and clinical sciences and introducing students to contextual learning.2,49
Participants of the current study suggested that more supervisors should be present in the clinic as this would enhance the efficiency of clinical training. South African dental students (46.7%) who participated in the study by Wilson et al. (2015) reported that the ratio of supervisors to students was a cause of stress.28 According to Ebbeling et al. (2018), students reported the limited number of clinical training staff and, in turn, their unavailability during the clinical sessions.10 This was similarly conquered by Henzi et al. (2007) and Pyle et al. (2006).26,50
The qualitative and quantitative data revealed that, according to students, a disconnect existed between theory and clinical training. Participants stated that both aspects of the curriculum should correspond and that more emphasis should be placed on clinical training rather than the theoretical component. In contrast, students who participated in the Gerzina et al. (2005) study agreed that a link existed between theory and clinical practice.2 The oral hygiene cohort of participants favoured clinical supervision being conducted by oral hygienists who would be more familiar with the scope of practice.
Further suggestions included introducing an additional training site, improved engagement between the academic staff and students, regular exposure to patients, implementing modern technology at the institution and a more accommodating quota system.
RECOMMENDATIONS
This study may potentially provide insight into students' experiences at the study site and ways in which the course structure and delivery may be enhanced. The current study may also contribute to the existing literature on dental education during the pandemic. Opportunities for future research may include participants from other institutions and disciplines.
CONCLUSION
This study highlights the various perceptions of dental therapy and oral hygiene students regarding teaching methods, suitable attributes of academic staff, potential barriers to learning, clinical quotas, effects of the pandemic, strategies that may enable continued learning and recommendations to enhance teaching and learning. Possible limitations are the use of a single study site and the small sample size. The results of this study cannot be generalised due to these limitations. The study was also extended into the 2022 academic year due to the effects of COVID in 2021. The use of student perceptions in dental education, especially regarding curriculum design, is highlighted in this study. Institutions should regularly engage with students by providing a platform to discuss successes, challenges, recommendations and other relevant topics. This will promote students' involvement in their learning process and may lead to impactful changes within dental education.
DECLARATIONS
Acknowledgements
The authors would like to thank all participants for their involvement in the study.
Funding
Financial support was received from the College of Health Sciences through a scholarship.
Ethics approval
Ethical approval was granted by the Humanities and Social Sciences Research Ethics Committee (HSSREC/00002902/2021). All participants consented to their participation in this study.
Competing interests
The authors declare they have no competing interests.
REFERENCES
1. Chang TY Hong G, Paganelli C, Phantumvanit P, Chang WJ, Shieh YS, et al. Innovation of dental education during COVID-19 pandemic. J Dent Sci. 2021;16(1):15-20. doi: 10.1016/j.jds.2020.07.011 [ Links ]
2. Gerzina TM, McLean T, Fairley J. Dental clinical teaching: perceptions of students and teachers. J Dent Educ. 2005;69(12):1377-84. Available from https://onlinelibrary.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=0022-0337&date=2005&volume=69&issue=12&spage=1377 [ Links ]
3. losif L, Tâncu AMC, Didilescu AC, Imre M, Galbinasu BM, Ilinca R. Self-Perceived Impact of COVID-19 Pandemic by Dental Students in Bucharest. International Journal of Environmental Research and Public Health. 2021;18(10):5249. Available from: http://dx.doi.org/10.3390/ijerph18105249 [ Links ]
4. Ansary JA, Ara I, Talukder HK, Alam ASMM, Amin S & Rahman SMH (2011). Views of students regarding effective clinical teaching and learning in dental education. Bangladesh Journal of Medical Education 2(1):1-5. Available from: https://www.banglajol.info/index.php/BJME/article/download/18129/12665. [ Links ]
5. Aamer S, Khan RA, Saleem A, Zia AU, Hassan F, Afzal A. Undergraduate dental students' perceptions of educational strategies at Foundation university college of dentistry. 2019;11(1):39-44. Available from: https://poj.org.pk/index.php/poj/article/view/264 [ Links ]
6. Divaris K, Barlow PJ, Chendea SA, Cheong WS, Dounis A, Dragan IF, et al. The academic environment: the students' perspective. Eur J Dent Educ. 2008;12 Suppl 1:120-30. doi: 10.1111/j.1600-0579.2007.00494.x [ Links ]
7. Subramanian J, Anderson V, Morgaine K, Thomson W. The importance of "student voice" in dental education. European Journal of Dental Education. 2013;17:e136-e141. Available from: https://www.deepdyve.com/lp/wiley/the-importance-of-student-voice-in-dental-education-bB4qhJh7ZH#bsSignUpModal [ Links ]
8. Bhayat A, Barrie R, Motloba P, Yengopal V. The South African Dental Schools' Educational Environment: Final Year Students' Perceptions at Four Dental Schools. JCDL. 12; 12:40-44. doi:10.7860/JCDR/2018/37507.12418 [ Links ]
9. Varvara G, Bernardi S, Bianchi S, Sinjari B, Piattelli M. Dental Education Challenges during the COVID-19 Pandemic Period in Italy: Undergraduate Student Feedback, Future Perspectives, and the Needs of Teaching Strategies for Professional Development. Healthcare (Basel). 2021;9(4):454. doi: 10.3390/healthcare9040454 [ Links ]
10. Hassan MG, Amer H. Dental Education in the Time of COVID-19 Pandemic: Challenges and Recommendations. Front Med (Lausanne). 2021;8:648899. doi:10.3389/fmed.2021.648899 [ Links ]
11. Mohamed N, Peerbhay F. Introducing Dental Students to E-learning at a South African University. African Journal of Health Professions Education. 2012;4(2):123-127. https://doi.org/10.7196/ajhpe.179 [ Links ]
12. Tadesse S, Muluye, W. The Impact of COVID-19 Pandemic on Education System in Developing Countries: A Review. Open Journal of Social Sciences. 2020;8:159-170. doi: 10.4236/jss.2020.810011 [ Links ]
13. Ebbeling S, Adam L, Meldrum A, Rich A, McLean A, Aitken W. Oral Health and Dental Students' Perceptions of Their Clinical Learning Environment: A Focus Group Study. J Dent Educ. 2018;82(10):1036-1042. doi: 10.21815/JDE.018.102 [ Links ]
14. Victoroff KZ, Hogan S. Students' perceptions of effective learning experiences in dental school: a qualitative study using a critical incident technique. J Dent Educ. 2006;70(2):124-32. Available from: https://doi.org/10.1002/J.0022-0337.2006.70.2.TB04068.X [ Links ]
15. Wilkinson DM, Smallidge D, Boyd LD, Giblin L. Students' Perceptions of Teaching Methods That Bridge Theory to Practice in Dental Hygiene Education. J Dent Hyg. 2015;89(5):330-7. Available from: https://jdh.adha.org/content/jdenthyg/89/5/330.full.pdf [ Links ]
16. Bourzgui F, Alami S, Diouny S. A Comparative Study of Online and Face-to-Face Learning in Dental Education. EC Dental Science. 2020; 19(3):1-11. Available from: https://www.researchgate.net/publication/339948717_A_Comparative_Study_of_Online_and_Face-to-Face_Learning_in_Dental_Education [ Links ]
17. Noor R, Singh D, Agarwal A, Mansoori S, Ansari MI. Perception of dental students towards the online method of dental education during the COVID-19 pandemic. J Oral Biol Craniofac Res. 2022;12(2):223-227. doi: 10.1016/j.jobcr.2022.02.002 [ Links ]
18. Quinn B, Field J, Gorter R, Akota I, Manzanares MC, Paganelli C, et al. COVID-19: The immediate response of European academic dental institutions and future implications for dental education. Eur J Dent Educ. 2020;24(4):811-814. doi: 10.1111/eje.12542 [ Links ]
19. Hussein KS. Perceptions of an integrated curriculum among dental students in a public university in Saudi Arabia. Electron Physician. 2017;9(7):4828-4834. doi: 10.19082/4828 [ Links ]
20. Schönwetter DJ, Lavigne S, Mazurat R, Nazarko O. Students' perceptions of effective classroom and clinical teaching in dental and dental hygiene education. J Dent Educ. 2006 Jun;70(6):624-35. https://doi.org/10.1002/j.0022-0337.2006.70.6.tb04118.x [ Links ]
21. Nerali J, Pishipati VKC, Telang L, Telang A. Dental Students' Perceptions towards Feedback during Clinical Training. Archives of Medicine and Health Sciences. 2021;9(1):62-67. Available from: https://www.amhsjournal.org/article.asp?issn=2321-4848;year=2021;volume=9;issue=1;spage=62;epage=67;aulast=Nerali;type=2 [ Links ]
22. Adam L, McLean A, Meldrum A, Rich A. Guidelines for providing feedback in the clinical dental setting. Available from: http://www.otago.ac.nz/council/committees/otago611272.pdf [ Links ]
23. Mitchell JK, Gillies RA, Mackert R. Setting Expectations About Feedback in Dental Education. MedEdPORTAL. 2017;13:10580. doi: 10.15766/mep_2374-8265.10580 [ Links ]
24. Anderson VR, Rich AM, Seymour GJ. Undergraduate dental education in New Zeal and: 2007-2009 final-year student feedback on clinical learning environments. N Z Dent J. 2011 Sep;107(3):85-90. PMID: 21957835 [ Links ]
25. Fugill M. Teaching and learning in dental student clinical practice. Eur J Dent Educ. 2005 Aug;9(3):131-6. doi: 10.1111/j.1600-0579.2005.00378.x [ Links ]
26. Henzi D, Davis E, Jasinevicius R, Hendricson W. North American dental students' perspectives about their clinical education. J Dent Educ. 2006 Apr;70(4):361-377. doi:10.1002/j.0022-0337.2006.70.4.tb04091.x [ Links ]
27. Alves de Lima AE. Devolución constructiva. Una estrategia para mejorar el aprendizaje [Constructive feedback. A strategy to enhance learning]. Medicina (B Aires). 2008;68(1):88-92. Spanish. [ Links ]
28. Wilson VJ, Rayner CA, Gordon NA, Shaikh AB, Crombie K, Yasin-Harnekar S. Perceived stress among dental students at the University of the Western Cape. S. Afr. dent. j. 2015;70(6):255-259. Available from: http://www.scielo.org.za/scielo.php?script=sci_arttext&pid=S0011-85162015000600007&lng=en [ Links ]
29. Al-Saleh SA, Al-Madi EM, Al-Angari NS, Al-Shehri HA, Shukri MM. Survey of perceived stress-inducing problems among dental students, Saudi Arabia. Saudi Dent J. 2010;22(2):83-88. doi: 10.1016/j.sdentj.2010.02.007 [ Links ]
30. Alzahem AM, van der Molen HT, Alaujan AH, Schmidt HG, Zamakhshary MH. Stress amongst dental students: a systematic review. Eur J Dent Educ. 2011;15(1):8-18. doi: 10.1111/j.1600-0579.2010.00640.x [ Links ]
31. Birks Y, McKendree J, Watt I. Emotional intelligence and perceived stress in healthcare students: a multi-institutional, multi-professional survey. BMC Med Educ.2009;9:61. doi: 10.1186/1472-6920-9-61 [ Links ]
32. Dahan H, Bedos C. A typology of dental students according to their experience of stress: a qualitative study. J Dent Educ. 2010;74(2):95-103. https://doi.org/10.1002/j.0022-0337.2010.74.2.tb04858.x [ Links ]
33. Gorter R, Freeman R, Hammen S, Murtomaa H, Blinkhorn A, Humphris G. Psychological stress and health in undergraduate dental students: fifth year outcomes compared with first year baseline results from five European dental schools. Eur J Dent Educ. 2008;12(2):61-68. doi: 10.1111/j.1600-0579.2008.00468.x [ Links ]
34. Heath JR, Macfarlane TV, Umar MS. Perceived sources of stress in dental students.Dent Update. 1999;26(3):94-98, 100. doi: 10.12968/denu.1999.26.3.94 [ Links ]
35. Hendricks SJH, Joshi A, Crombie K, Moola MH. Perceived sources of stress among black dental students in South Africa. J Dent Educ 1994;58(6): 406-410. https://doi.org/10.1002/j.0022-0337.1994.58.6.tb02867.x [ Links ]
36. Humphris G, Blinkhorn A, Freeman R, Gorter R, Hoad-Reddick G, Murtomaa H, O'Sullivan R, Splieth C. Psychological stress in undergraduate dental students: baseline results from seven European dental schools. Eur J Dent Educ. 2002;6(1):22-29. doi:10.1034/j.1600-0579.2002.060105.x [ Links ]
37. Kumar S, Dagli RJ, Mathur A, Jain M, Prabu D, Kulkarni S. Perceived sources of stress amongst Indian dental students. Eur J Dent Educ. 2009;13(1):39-45. doi:10.1111/j.1600-0579.2008.00535.x [ Links ]
38. Naidu RS, Adams JS, Simeon D, Persad S. Sources of stress and psychological disturbance among dental students in the West Indies. J Dent Educ 2002;66:1021-1030. https://doi.org/10.1002/j.0022-0337.2002.66.9.tb03569.x [ Links ]
39. Polychronopoulou A, Divaris K. Dental students' perceived sources of stress: a multi- country study. J Dent Educ 2009; 73(5):631-639. https://doi.org/10.1002/j.0022-0337.2009.73.5.tb04738.x [ Links ]
40. Polychronopoulou A, Divaris K. Perceived sources of stress among Greek dental students. J Dent Educ 2005;69(6):687-692. https://doi.org/10.1002/j.0022-0337.2005.69.6.tb03952.x [ Links ]
41. Sanders AE, Lushington K. Effect of perceived stress on student performance in dental school. J Dent Educ 2002;66(1):75-81. https://doi.org/10.1002/j.0022-0337.2002.66.1.tb03510.x [ Links ]
42. Silverstein ST, Kritz-Silverstein DA. A longitudinal study of stress in first-year dental students. J Dent Educ 2010;74(8):836-848. https://doi.org/10.1002/j.0022-0337.2010.74.8.tb04940.x [ Links ]
43. McGleenon EL, Morison S. Preparing dental students for independent practice: a scoping review of methods and trends in undergraduate clinical skills teaching in the UK and Ireland. Br Dent J. 2021;230(1):39-45. doi: 10.1038/s41415-020-2505-7 [ Links ]
44. Mamattah RS. Students' Perceptions of E-Learning. Masters Thesis (Linköping University), 2016. Available from: http://www.diva-portal.org/smash/get/diva2:925978/FULLTEXT01.pdf [ Links ]
45. Lynch CD, Singhrao H, Addy LD, Gilmour AS. The teaching of fixed partial dentures in undergraduate dental schools in Ireland and the United Kingdom. J Oral Rehabil. 2010;37(12):908-15. doi: 10.1111/j.1365-2842.2010.02106.x [ Links ]
46. Davey J, Bryant ST, Dummer PM. The confidence of undergraduate dental students when performing root canal treatment and their perception of the quality of endodontic education. Eur J Dent Educ. 2015;19(4):229-34. doi: 10.1111/eje.12130 [ Links ]
47. Clark RK, Radford DR, Juszczyk AS. Current trends in removable partial denture teaching in British dental schools. Br Dent J. 2011;211(11):531-5. doi: 10.1038/ sj.bdj.2011.1003 [ Links ]
48. Gilmour AS, Welply A, Cowpe JG, Bullock AD, Jones RJ. The undergraduate preparation of dentists: Confidence levels of final year dental students at the School of Dentistry in Cardiff. Br Dent J. 2016;221(6):349-54. doi: 10.1038/sj.bdj.2016.686 [ Links ]
49. Mullins G, Wetherell J & Robbé I. Learning in the clinical environment. In Effective Learning and Teaching in Medical, Dental and Veterinary Education, 1st edition, Routledge, London, 2002. Available from: https://doi.org/10.4324/9780203416860 [ Links ]
50. Pyle M, Andrieu SC, Chadwick DG, Chmar JE, Cole JR, George MC, Glickman GN, Glover JF, Goldberg JS, Haden NK, Hendricson WD, Meyerowitz C, Neumann L, Tedesco LA Valachovic RW, Weaver RG, Winder RL, Young SK, Kalkwarf KL; ADEA Commission on Change and Innovation in Dental Education. The case for change in dental education. J Dent Educ. 2006 Sep;70(9):921-4. PMID: 16954413 [ Links ]
 Correspondence:
Correspondence:
Name: Dr R Moodley
Email: moodleyra@ukzn.ac.za


{kind=link}
{kind=link}
{kind=link}