










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.78 no.4 Johannesburg Mai. 2023
http://dx.doi.org/10.17159/sadj.v78i04.15177
RESEARCH
A pre and post-test assessment of an oral health intervention: caregivers' knowledge and attitudes at long-term care facilities in the eThekwini district, KwaZulu-Natal
S BalwanthI; S SinghII
IBChD, PG Dip Int Ortho (UWC), MMedSc (UKZN), Discipline of Dentistry, School of Health Sciences, University of KwaZulu-Natal, South Africa. E: sonambalwanth7@gmail.com ORCID: 0000-0003-2991-399X
IIPhD. B.OH, M.Sc (Dent), PhD (UWC), PG Dip Heal Res Ethics (Stellenbosch), PhD Clin and Res Ethics (Stellenbosch). Professor, Discipline of Dentistry, School of Health Sciences, University of KwaZulu-Natal, South Africa
ABSTRACT
INTRODUCTION: Oral health remains a neglected aspect of healthcare among vulnerable populations residing at long-term care (LTC) facilities. Routine oral health education and training for caregivers have the potential to improve oral health provision.
AIMS AND OBJECTIVE: To determine the effect of an oral health intervention on caregivers' knowledge and attitudes.
METHODS: This cross-sectional study utilised a pre/post-test assessment approach. A total of n=145 caregivers from n=7 LTC facilities in the eThekwini district, participated in a pretest questionnaire. An oral health education intervention in the form of a PowerPoint® presentation was implemented four weeks later. Six months later, a post-test questionnaire was administered. A Paired proportion test was used for statistical analysis. A p-value <0.05 was considered to be statistically significant.
RESULTS: A response rate of 77.1% was obtained. In the pre-intervention phase, caregivers (n=68; 46.9%) reported that loose teeth can be a sign of gum and bone disease, compared to 89% (n=129) of caregivers in the postintervention phase. Caregivers (n=124; 85.5%) in the pre-intervention phase felt that they should be trained in providing oral healthcare, compared to 93.8% (n=136) in the post-intervention phase.
CONCLUSION: The oral health intervention had a positive effect on caregivers' knowledge and attitudes. This finding necessitates routine oral health education and training for caregivers.
Keywords: Caregivers, long-term care facilities, institutionalised residents, oral health education, oral health training
INTRODUCTION
Oral disease is a major public health concern due to the high prevalence and debilitating social impact on individuals globally.1,2 The prevalence of oral disease is significantly higher in dependent populations with special needs, including the elderly population, vulnerable children and cognitively or physically impaired individuals residing at LTC facilities.3,4,5,6 Poor oral health among residents at LTC facilities, present with far reaching consequences and have implications on preventive, promotional and future dental treatment.3,7,8,9 Previous international studies have postulated that the higher incidence of oral disease among institutionalised residents could be attributed to barriers in accessing appropriate oral healthcare.7,10 These barriers include: cost of oral healthcare services, residents' impaired mental abilities or limited physical dexterity, low perceived need for oral care by residents and caregivers, and caregivers' lack of oral health knowledge.7,11 Caregivers are expected to play an important role in the prevention of oral disease and deliverance of appropriate and adequate oral healthcare to satisfy the special oral health needs of residents at LTC facilities. This, however, may not always be realised due to prioritisation of other caregiving duties resulting in a deficiency of time, a lack of knowledge and skills in oral healthcare, non-communicative and uncooperative residents, and a lack of understanding of the importance of oral health among caregivers.7,10
Numerous international studies have identified the lack of adequate oral health knowledge among caregivers as a recurrent contributing factor to poor oral health among institutionalised residents.1,7,1 Consequently, substantial international literature has highlighted the importance and effectiveness of oral health education in a variety of settings, including LTC facilities.1,6,7,10,12,13 It was found that the success of oral health education depends on the co-operation of caregivers and regular in-service training with frequent monitoring.7 Integration of oral healthcare services into routine healthcare services is another fundamental method in achieving better oral health outcomes and, in turn, better overall quality of life for individuals.1 This can be achieved through collaboration with nursing staff, and dental and medical professionals, in the provision of healthcare services for institutionalised residents.14 Additionally, incorporating oral examinations into routine care by caregivers has been reported by several authors as a useful tool in improving institutionalised residents' oral health.11,15 ,16
Caregivers are often the first healthcare providers and thus have a responsibility and duty in providing oral healthcare to the institutionalised residents.18 Caregivers' oral health related knowledge and skills may directly or indirectly affect the quality of care rendered to the residents. There is a paucity of information available in South Africa exploring the oral health related knowledge and attitudes among caregivers. Thus, the aim of this study was to evaluate the impact of an oral health education intervention among caregivers at LTC facilities in the eThekwini district. The scientific hypothesis of the study was that oral health education intervention for caregivers would result in an improvement in their oral health related knowledge, attitudes and, in turn, practices.
METHODS
The study utilised a cross-sectional, analytical and comparative research design and a pre/post-test assessment approach. Study sites included n=39 LTC facilities operated by non-profit organisations selected from "eThekwini health and well-being service provider directory 2018" and n=28 private or semi-privately operated LTC facilities from a website called "Senior service retirement places" on search engine company Google.19,20 Every facility from the above-mentioned directory and website were purposively included in the selection process. A total of seven (n=7) long-term care facilities participated in the study, which included six (n=6) old age homes and one (n=1) children's home in eThekwini, all of which offer long-term care. Caregivers at the participating LTC facilities were purposively sampled using a criterion and snowball sampling technique. A sample of one hundred and eighty-eight (n=188) questionnaires were distributed among voluntary participants of which one hundred and forty-five (n=145) were suitable for further analysis, yielding a response rate of 77.1%.
Prior to conducting the research, details of the study were explained and written permission was obtained from managers of each facility. Participants were invited to partake in the study and informed consent was obtained. Study participants were informed that the study was voluntary and were free to withdraw from the study at any stage, without any negative consequences.
In consultation with the gatekeepers of each facility, overseeing the completion of the questionnaires was not permissible due to the Covid-19 risk. In keeping with Covid-19 protocols and policy of each facility, in order to minimise contact with staff and caregivers the pre and post-test self-administered questionnaires were distributed to participating caregivers by the managers or nurses of each facility.
A pre-test self-administered questionnaire was distributed among participants and used to gather baseline quantitative data. An oral health education intervention in the form of a PowerPoint® presentation was implemented one month later. Six months later, a post-test self-administered questionnaire was distributed among the same participants to evaluate the effect of the oral health education intervention.
A 15-item questionnaire was developed in English to assess caregivers' oral health related knowledge and attitudes pre and post-intervention. The first section of the questionnaire included questions on participants' biographical information such as: gender, age, level of education and years of work experience. The second part included questions on knowledge such as: denture care, recognition and management of common oral conditions, recognition of oral side effects of medications, nutrition and diet, and paediatric dentistry in the form of a Likert scale with the format of responses: 1-strongly agree, 2-agree, 3-not sure, 4-disagree and 5-strongly disagree. Other questions included knowledge of oral hygiene, understanding of dental terms and mechanism of dental decay. The third part of the questionnaire focused on participants' attitudes regarding care for residents, recognition of residents' special oral health requirements, oral health training and existing oral health protocols, which was presented in the form of a Likert scale. Closed ended questions were used in this questionnaire. The oral health education intervention in the form of a PowerPoint® presentation, focused on the importance of the caregivers' role in maintaining adequate oral hygiene for the residents, which included management of common oral conditions, special oral health care practices for residents, diet and nutrition, and proper oral hygiene instructions such as brushing and flossing techniques. Video clips demonstrating proper oral hygiene and brushing techniques and utilising dental aids were also included. The oral health education intervention was based on guidelines outlined by the World Health Organisation.21 The researcher provided the participants with toothbrushes, toothpaste, flossing aids and pamphlets on oral hygiene education to enhance the effectiveness of the oral health education intervention.
Before commencing the study, a pilot study was conducted among (n=8) caregivers at a long-term care facility in eThekwini, who were excluded from the final questionnaire. Inconsistencies, ambiguity and grammatical errors were rectified before conduction of the study.
Pre and post-test evaluation of oral health scores were performed using the same semi-structured self-administered questionnaire. The collected data were entered into Microsoft Excel 2007 and subjected to statistical analysis using SPSS version 27.0 (IBM Statistics Inc, Chicago, Illinois, USA). The Paired proportion test was used to And the significance of change in proportion from pre to post-intervention. A p-value <0.05 was considered to be statistically significant.
The study was granted ethical clearance by the Biomedical Research Ethics Committee at the University of KwaZulu-Natal (BREC/00002633/2021). All other ethical issues, such as confidentiality and anonymity, were maintained.
RESULTS
Socio-demographic profile of caregivers
All participants were females with the majority being within the age group 37-42 years old (n=37; 25.5%), holding a secondary level of education (n=99; 68.3%), and having had 6-10 years of caregiving experience (n=69; 47.6%), as demonstrated in Table 1.

Pre and post-test evaluation of caregivers' oral health related knowledge
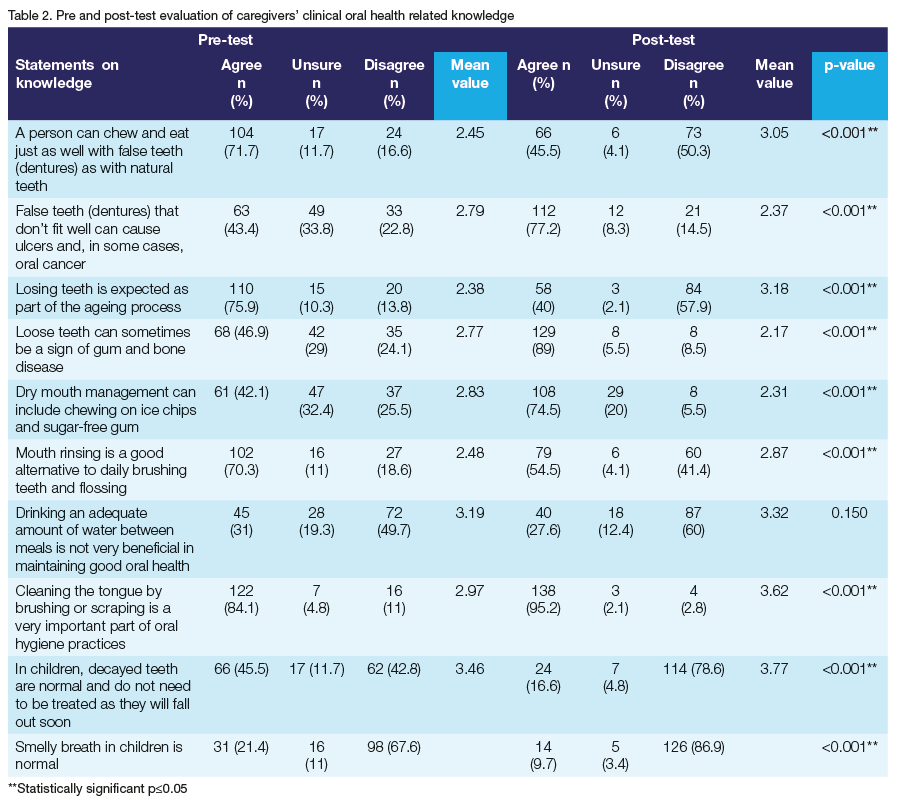
About 16.6% (n=24) of the caregivers disagreed with the statement that a person can chew and eat as well with false teeth (dentures) as with natural teeth in the pre-intervention phase, compared to 50.3% of the study sample (n=73) in the post-intervention evaluation who disagreed with the statement, as demonstrated in Table 2.
Before the oral health education intervention, less than half of the caregivers (n=63; 43.4%) agreed that false teeth (dentures) that do not fit well can cause ulcers and, in some cases, oral cancer. In the post-intervention evaluation, the majority of the caregivers (n=112; 77.2%) agreed with the statement.
With regard to the statement: "Losing teeth is expected as part of the ageing process", few caregivers (n=20; 13.8%) disagreed with the statement in the pre-intervention phase. In the post-intervention evaluation, 57.9% of the caregivers (n=84) disagreed with the statement. Less than half of the caregivers (n=68; 46.9%) in the pre-intervention phase agreed that loose teeth can sometimes be a sign of gum and bone disease, while 89% of caregivers (n=129) in the post-intervention agreed.
Some participants (n=61; 42.1%) in the pre-intervention phase indicated that dry mouth management can include chewing on ice chips and sugar-free gum, compared to n=108 caregivers (74.5%) in the post-intervention phase with the same response.
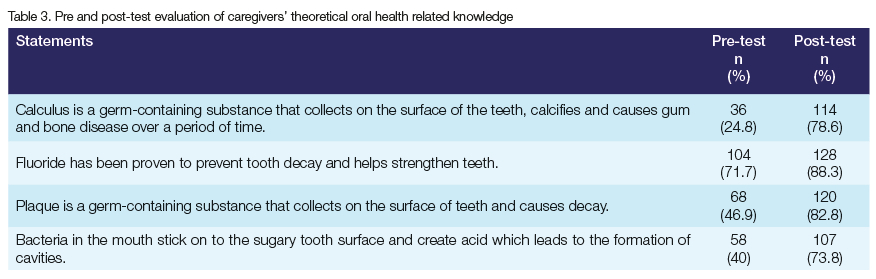
In the pre-intervention phase, 49.7% of the caregivers (n=72) disagreed with the statement: "Drinking an adequate amount of water between meals is not very beneficial in maintaining good oral health", compared to 60% of caregivers (n=87) in the post-intervention evaluation who disagreed. Caregivers' theoretical oral health related knowledge pre and postIntervention is demonstrated in Table 3.
ATTITUDES
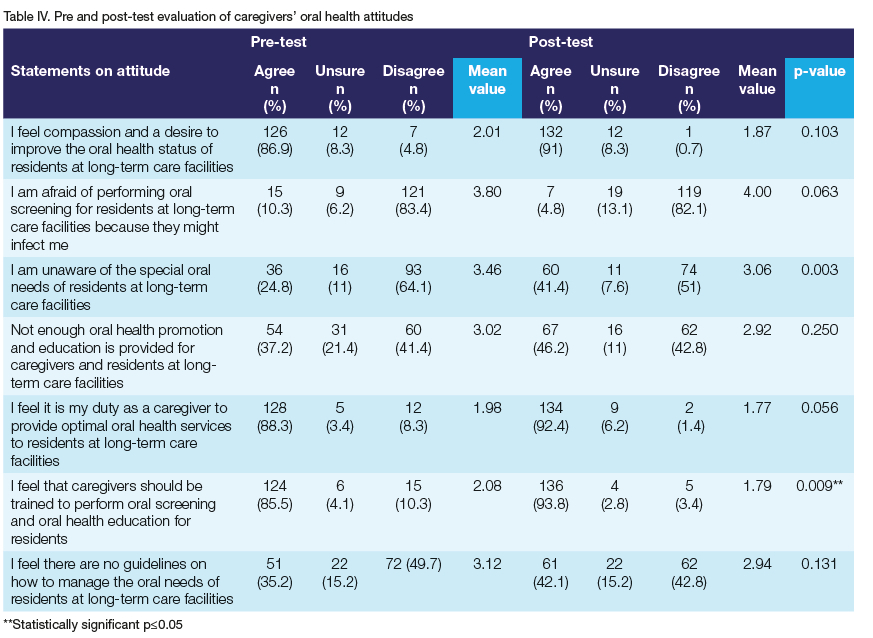
Less than half of the participants (n=54; 37.2%) in the pre-intervention phase reported that insufficient oral health promotion and education has been provided for caregivers and residents at LTC facilities. In the post-intervention evaluation, 46.2% of caregivers (n=67) had the same response, as illustrated in Table 4.
Most of the sample population (n=124; 85.5%) indicated to feel that caregivers should be trained to perform oral screening and provide oral health education for residents in the pre-intervention phase, compared to almost all participants (n=136; 93.8%) in the post-intervention evaluation who shared the same sentiment.
With regard to the statement: "I feel there are no guidelines on how to manage the oral needs of residents at long-term care facilities", before the oral health intervention, 35.2% of the caregivers n=51 agreed with the statement. In the postintervention evaluation, 42.1% of caregivers n=61 reported to feel the same.
DISCUSSION
All participants in the study were female, which coincides with several studies involving caregivers at LTC facilities.22,23,24 A possible reason for this could be attributed to the perceived cultural stereotype where jobs involving care and nurturing are reserved for females.24 The majority of the caregivers in the current study reported to hold a secondary level of education (68.3%). Similarly, a study evaluating the impact of an oral health educational programme for caregivers of institutionalised residents found that the majority of caregivers (64.3%) had only obtained elementary school education.12 Walid, Nasir and Naidoo, (2004) suggested that although not ideal, in developing and underresourced countries such as South Africa, non-healthcare workers can contribute to the promotion of oral health through training and education and, in turn, improve oral health outcomes for residents at LTC facilities. 25
Oral health related knowledge among caregivers
The results of the study indicated that caregivers' overall oral health knowledge increased from baseline to post-intervention. Similar studies have postulated that implementation of oral health interventions, regardless of the measured variables, may result in better oral health outcomes for institutionalised residents due to improved knowledge among caregivers.12,26
Due to physical and cognitive limitations, self-care oral hygiene practices may not be adequate, inevitably resulting in unmet oral health needs and reduced quality of life among residents.2 Thus, caregivers have a significant responsibility towards providing residents with optimal oral healthcare. However, numerous studies have reported that the oral health knowledge among caregivers is inadequate, perpetuating poor oral health among residents.1,3,7,12,27,2 Therefore, many authors have postulated that by improving oral health knowledge among caregivers through education and training, oral hygiene practices among care-dependent residents could improve.10,22,2 ,30
Caregivers (n=73; 50.3%) in the post-intervention phase acknowledged that individuals with dentures cannot chew as efficiently as those individuals with natural teeth. Hence, caregivers also play an important motivational role in advising and assisting denture wearing residents with proper denture education, including food selections, in order to avoid gastro-intestinal ailments and nutritional deficiencies.8 The majority of the caregivers (n=112; 77.2%) in the postintervention phase reported that ill-fitting dentures can cause ulcers and, in some cases, oral cancer. This finding concurs with a study conducted by Manoharan, Nagaraja and Eslick (2014), who found that the use of dentures -and more so ill-fitting dentures - increases the risk of developing cancer. It is thus imperative that caregivers' knowledge in denture care be optimal and that preventive measures such as oral screenings and checking of dentures are made mandatory at LTC facilities, in order to prevent denture related conditions such as denture stomatitis, oral candidiasis and ulcerations, which can manifest into more sinister conditions if left untreated.8,31
Vulnerable, abandoned and disadvantaged children form a socially marginalised population and therefore tend to experience more oral diseases.32 Khedekar et al. (2015) investigated the oral hygiene status of orphanage children in India and found that the majority of the orphaned children (59%) had experienced toothache and almost all children did not visit the dentist.32 In the current study, caregivers' knowledge regarding the importance of seeking professional dental treatment for decayed teeth in children in the pre-intervention phase was low (n=62; 42.8%). This finding highlights the fact that children's oral health is neglected and not deemed a priority by caregivers, which can be attributed to the lack of knowledge and expertise among caregivers in recognising symptoms of dental diseases. Khedekar et al. (2015) further found that bad breath and bleeding gums were a common finding among the children at the orphanage in India.32 Some caregivers (n=31; 21,4%) in the pre-intervention phase reported that smelly breath in children was normal, which raises a major concern with regard to a lack of oral hygiene reinforcement by caregivers and indicates a lack of paediatric dental knowledge. While this response decreased (n=14; 9.7%) following the oral health intervention, the documented high prevalence of dental caries and oral disease among children residing in orphanages necessitates more attention towards improving the knowledge and skills of caregivers and creating oral health awareness at LTC facilities. Likewise, both authors Khedekar et al. (2015) and Bushra and Othman (2022) noted significant improvement in caregivers' knowledge, attitudes and practices following an oral health education programme involving oral health provision for orphaned children.32, 33
Oral health related attitudes among caregivers
Almost all caregivers (n=132; 91%) in the post-intervention phase expressed compassion and optimism to improve the oral health status of the residents under their care and felt that providing optimal oral healthcare to the institutionalised residents was their desire and duty (n=134; 92.4%). Conversely, Cornejo-Ovalle et al. (2013) found that approximately one third of caregivers felt obligated to work at a LTC facility for the elderly because of necessity.24
Additionally, Wardh, Andersson and Sorensen (1997) found that caregivers were not keen on cleaning the residents' mouths and preferred conducting other nursing duties, in effect neglecting the residents' oral health.34 Encouraging was the finding that the majority of caregivers (n=119; 82.1%) in the current study's post-intervention phase were not afraid to examine the residents' mouths and perform oral screenings. The post-intervention results indicated that many caregivers (n=67; 46.2%) felt that insufficient oral health promotion and education programmes were conducted at LTC facilities, and 42.1% of the caregivers (n=61) reported to feel that there were no guidelines on how to manage the special oral needs of residents. These findings are significant as they highlight the lack of oral health prioritisation at LTC facilities and indicate the dire need for clear oral health guidelines and protocols.
Almost all caregivers in the post-intervention phase of the current study (n=136; 93.8%) strongly felt that they should be trained to perform oral screenings and oral health education for residents. Similarly, studies conducted by Lago et al. (2017) and Cornejo-Ovalle et al. (2013) found that caregivers at LTC facilities reported to request more training in oral health.12,24 The finding of the current study necessitates the implementation of oral health education for caregivers as a means to prioritise and promote oral health and, in turn, provide adequate oral health services to the residents at LTC facilities. Petrovski et al. (2019), proposed that oral health education programmes must include evaluation of the oral health status of the institutionalised residents, oral health education tailored towards the integral role caregivers play in heeding to the special oral health needs of residents, and planning of oral hygiene practices for the residents, so as to meet the basic criteria for prevention of oral diseases and appropriate management thereof.10
STUDY LIMITATIONS
Due to the Covid-19 pandemic and the subsequent regulations on lockdown, the number of participating LTC facilities were limited to seven n=7 from a total sample of n=67. Access to study sites was prohibited to visitors, including the researcher, which resulted in a delay of the data collection. The use of self-reported questionnaires may have resulted in over or underreporting by reason of social desirability, thereby not necessarily demonstrating the current situation35,36 The study was limited to the eThekwini district and cannot be generalised to other regions of KwaZulu-Natal. Further research on a larger scale is required to explore the effect of an oral health education intervention on the oral health related knowledge, attitudes and practices of caregivers at long-term care facilities in South Africa.
RECOMMENDATIONS
The results of this study can be used to make recommendations to oral health planners and stakeholders to develop clear and comprehensive oral health policies within LTC facilities, and on a national level. More emphasis needs to be placed on oral health promotion during the planning process of oral health policies to address the special needs of individuals residing at LTC facilities. Additionally, the nursing curriculum should be more inclusive of oral health education to ensure better oral disease management and appropriate referral pathways are followed, thereby facilitating prompt treatment and improving overall quality of life among residents. Regular in-service oral health training can equip caregivers with the necessary knowledge and skills to provide preventive and promotional activities, such as oral screenings, to the residents under their care. Furthermore, a multidisciplinary and multisectoral approach can be formed with dental professionals, dental students and other healthcare professionals and sectors, to provide oral screenings to the residents as a means of increasing access and improving the oral and overall health of residents.37
CONCLUSION
The results of the study showed that there was an improvement in the oral health knowledge and attitudes among the caregivers in the post-intervention phase. The study revealed the importance and effectiveness of an oral health education intervention and therefore highlights the need for a scale up in oral health education and training at LTC facilities.
Conflict of interest
The authors declare they have no financial or personal relationships that may have inappropriately influenced them in writing this article. The authors consent to publication and declare there are no conflicting interests.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
REFERENCES
1. Khanagar S, Kini P, Kumar A, Rajanna V, Badiyani B, Jathanna V Oral health care education and its effect on caregivers' knowledge, attitudes, and practices: A randomized controlled trial. J Int Soc Prev Community Dent [serial online]. 2014 [cited 2020 Nov 12];4(2):122. Available from: /pmc/articles/ PMC4170545/?report=abstract. https://doi.org/10.4103/2231-0762.139843 [ Links ]
2. World Health Organisation. Oral Health [Homepage on the internet]. 2022 [cited 2022 Jul 20]. Available from: https://www.who.int/news-room/fact-sheets/detail/oral-health [ Links ]
3. Abullais SS, Al-Shahrani FMF, Al-Gafel KMS, Saeed A-HA, Al-Mathami SA, Bhavikatti SK, et al. The knowledge, attitude and practices of the caregivers about oral health care at centers for intellectually disabled, in southern region of Saudi Arabia. Healthcare. 2020;8(4):416. https://doi.org/10.3390/healthcare8040416 [ Links ]
4. Shah AF, Tangade P, Ravishan, Tirth A, Pal S, Manu B. Dental caries status of institutionalised orphan children from Jammu and Kashmir, India. Int J Clin Pediatr Dent. 2016;9(4):364-71. https://doi.org/10.5005/jp-journals-10005-1392 [ Links ]
5. Nqcobo C, Ralephenya T, Kolisa YM, Esan T, Yengopal V. Caregivers' perceptions of the oral health related quality of life of children with special needs in Johannesburg, South Africa. Heal SA Gesondheid [serial online]. 2019 [cited 2020 Nov 12];24. Available from:/pmc/articles/PMC6917375/?report=abstract. https://doi.org/10.4102/hsag.v24i0.1056 [ Links ]
6. Manchery N, Subbiah G, Nagappan N, Premnath P. Are oral health education for carers effective in the oral hygiene management of elderly with dementia? A systematic review. Dent Res J. 2020;17(1):1-9. PMID: 32055287 [ Links ]
7. Simons D, Baker P, Jones B, Kidd EAM, Beighton D. An evaluation of an oral health training programme for carers of the elderly in residential homes. Br Dent J. 2000;188(4):206-10. https://doi.org/10.1038/sj.bdj.4800432 [ Links ]
8. Gil-Montoya JA, de Mello ALF, Barrios R, Gonzalez-Moles MA, Bravo M. Oral health in the elderly patient and its impact on general well-being: A nonsystematic review. Clin Interv Aging [serial online]. 2015 [cited 2020 Oct 27];10:461-7. Available from: / pmc/articles/PMC4334280/?report=abstract. https://doi.org/10.2147/CIA.S54630 [ Links ]
9. Hans R, Thomas S, Dagli R, Bhateja GA, Sharma A, Singh A. Oral health knowledge, attitude and practices of children and adolescents of orphanages in Jodhpur city Rajasthan, India. Journal Clin Diagnostic Res [serial online]. 2014;8(10):ZC22-5. Available from: https://doi.org/10.7860/JCDR/2014/9026.4948 [ Links ]
10. Petrovski M, Terzieva-Petrovska O, Kovecevska I, Minovska A, Ivanovski K, Papakoca K. Oral health education of staff in long-term care institutions. Balk J Dent Med. 2019;23(2):63-7. https://doi.org/10.2478/bjdm-2019-0012 [ Links ]
11. Hoad-Reddick G. Summary. Bristish Dent J. 1998;184:288. [ Links ]
12. Lago JD, Fais LMG, Montandon AAB, Pinelli LAP. Educational program in oral health for caregivers on the oral hygiene of dependent elders. Rev Odontol da UNESP [serial online]. 2017 [cited 2020 Nov 12];46(5):284-91. Available from: http://dx.doi.org/10.1590/1807-2577.23916 [ Links ]
13. Wu SJ, Wang CC, Kuo SC, Shieh SH HY. Evaluation of an oral hygiene education program for staff providing long-term care services: A mixed methods study. Int J Environ Res Public Health. 2020;17:4429. https://doi.org/10.3390/ijerph17124429 [ Links ]
14. Thema LK, Singh S. Integrated primary oral health services in South Africa: The role of the PHC nurse in providing oral health examination and education. African J Prim Health Care Fam Med. 2013;5(1):1-4. http://dx.doi.org/10.4102/phcfm.v5i1.413 [ Links ]
15. Sampson P, Page C, Shepard G. Oral hygiene: the mouth trap. Nursing Times. 1987;19. PMID: 3299280. [ Links ]
16. Griffiths J, Boyle S. Oral assessment in color guide to holistic oral care: a practical approach. Mosby Year Book Europe Ltd; 1993. 87-98. [ Links ]
17. Hoad-Reddick G. Assessment of elderly people on entry to residential homes and continuing care arrangements. J Dent. 1992;20:199-201. http://doi.org/10.1016/0300-5712(92)90073-l [ Links ]
18. Thomas B, Ciliska D, Dobbins M, Micucci S. A process for systematically reviewing the literature: providing the research evidence for public health nursing interventions. Worldviews Evid Based Nurs. 2004;1:176-84. http://doi.org/10.1111/j.1524-475X.2004.04006.X [ Links ]
19. Senior service retirement places. Comprehensive directory of retirement facilities in South Africa [homepage on the internet]. 2021 [cited 2021 May 18]. Available from: https://www.seniorservice.co.za/advanced-search/?province=Kwa+Zulu + Natal&city=DURBAN + -+Greater+Durban&property_ type=Old+Age+Homes§ion=properties [ Links ]
20. eThekwini municipality. eThekwini municipality health and wellbeing service provider directory 2018 [homepage on the internet]. 2018 [cited 2021 May 19]. Available from: http://www.durban.gov.za/Documents/HWDirectory2018.pdf [ Links ]
21. Petersen PE, Yamamoto T. Improving the oral health of older people: the approach of the WHO global oral health programme. Community Dent Oral Epidemiol [serial online]. 2005 [cited 2020 Dec 2];33:81-92. Available from: https://www.who.int/oral_health/publications/orh_cdoe05_vol33.pdf. http://doi.org/10.1111/j.1600-0528.2004.00219.x [ Links ]
22. Stancic I, Popovac AJ, Vasovic M, Petrovic M. Caregivers' attitudes, knowledge and practices of oral care at nursing homes in Serbia. Mil Pharm Rev [serial online]. 2016 [cited 2020 Nov 12];73(00):65-65. Available from: https://www.researchgate.net/publication/301703786_Caregivers'_attitudes_knowledge_and_ practices_of_oral_care_at_nursing_homes_in_Serbia. http://doi.org/10.2298/VSP141001065S [ Links ]
23. Urrutia C, Ormazábal F, Santander I, Salvo D. Oral health practices and beliefs among caregivers of the dependent elderly. Gerodontology. 2011;29(2):742-7. http://doi.org/10.1111/j.1741-2358.2011.00553.x [ Links ]
24. Cornejo-Ovalle M, Costa-de-Lima K, Pérez G, Borrell C, Casals-Peidro E. Oral health care activities performed by caregivers for institutionalised elderly in Barcelona-Spain. Med Oral Patol Oral Cir Bucal. 2013;18(4):e641-e649. http://doi.org/10.4317/medoral.18767 [ Links ]
25. Walid E, Nasir F, Naidoo S. Oral health knowledge, attitudes and behavior among nursing staff in Lesotho. SADJ. 2004;59(7):288,290-92. PMID: 15537032. [ Links ]
26. Munoz N, Touger-Decker R, Byham-Gray L, Maillet J. Effect of an oral health assessment education program on nurses' knowledge and patient care practices in skilled nursing facilities. Spec Care Dent. 2009;29(4):179-85. http://doi.org/10.1111/j.1754-4505.2009.00084.x [ Links ]
27. Wong F, Yannies T, Leung W. Oral health and its associated factors among older institutionalised residents-a systematic review. Int J Env Res Public Heal. 2019;16(21):4132. http://doi.org/10.3390/ijerph16214132 [ Links ]
28. Shah A, Naseem M, Khan M, Asiri F, AlQarni I, Gulzar S, et al. Oral health knowledge and attitude among caregivers of special needs patients at a comprehensive rehabilitation centre: an analytical study. Ann Stomatol. 2018;8(3):110-6. http://doi.org/10.11138/ads/2017.8.3.110 [ Links ]
29. Liu HY, Chen JR, Hsiao SY, Huang S Te. Caregivers' oral health knowledge, attitude and behaviour toward their children with disabilities. J Dent Sci. 2017;12(4):388-95. http://doi.org/10.1016/j.jds.2017.05.003 [ Links ]
30. Saarela RKT, Hiltunen K, Kautiainen H, Roitto HM, Mäntylä P PK. Oral hygiene and health-related quality of life in institutionalised older people. Eur Geriatr Med. 2022;13(1):213-20. http://doi.org/10.1007/s41999-021-00547-8 [ Links ]
31. Manoharan S, Nagaraja V Eslick G. Ill-fitting dentures and oral cancer: a meta-analysis. Oral Oncol. 2014;50(11):1058-61. http://doi.org/10.1016/j.oraloncology.2014.08.002 [ Links ]
32. Khedekar M, Suresh K V, Parkar MI, Malik N, Patil S, Taur S, et al. Implementation of oral health education to orphan children. J Coll physicians Surg. 2015;25(12):856-9. PMID: 26691356. [ Links ]
33. Bushra R, Othman ZY. Initial impact of an educational programme for the orphans in Erbil city. Eurasian J Sci Eng. 2022;8(1):180-6. [ Links ]
34. Wardh I, Andersson L, Sorensen S. Staff attitudes to oral health care. A comparative study of registered nurses, nursing assistants and home care aides. Gerodontology. 1997;14:28-32. http://doi.org/10.1111/j.1741-2358.1997.00028.x [ Links ]
35. Ahamed S, Moyin S, Punathil S, Patil NA, Kale VT, Pawar G, et al. Evaluation of the oral health knowledge, attitude and behaviour of the preclinical and clinical dental students. J Int Oral Heal. 2015;7:65-70. PMID: 26124603. [ Links ]
36. Singh S, Pottapinjara S. Dental undergraduate students' knowledge, attitudes and practices in oral health self-care: A survey from a South African university. African J Heal Prof Educ. 2017;9(2):83-7. http://doi.org/10.7196/AJHPE.2017.v9i2.800 [ Links ]
37. Thema LK, Singh S. Integrated primary oral health services in South Africa: The role of the PHC nurse in providing oral health examination and education. African J Prim Health Care Fam Med. 2013;5(1):1-4. http://dx.doi.org/10.4102/phcfm.v5i1.413 [ Links ]
 Correspondence:
Correspondence:
Name: S Singh
Tel: +27 31 2428591
Email: singhshen@ukzn.ac.za
Author's contribution:
1 . S Balwanth Primary author 70%
2 . S Singh Secondary author 30%


{kind=link}
{kind=link}
{kind=link}