










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.78 n.2 Johannesburg Mar. 2023
RESEARCH
Supernumerary teeth in a sample of South African dental patients
E ThomasI; AC OettléII; PJ BeckerIII
IBDS (India), MSc Dent (Wits), MDS (India) PhD student, Department of Orthodontics, University of Western Cape Tel: 072 836 5149 Address: Post Net Suite 1007, Private Bag X9, Benmore 2010 Email address: lizathomas67@gmail.com; ORCID: 0000-0003-4351-2850
IIMBBCh, DTE, MSc, PhD; Professor, Department of Anatomy and Histology, Sefako Makgatho Health Sciences University, Tel: 083 870 2379; Address: Department of Anatomy and Histology, Registry P.O Box 60, Medunsa 0204 Email: profoettle@gmail.com; ORCID: 0000-0002-9389-057X
IIIMSc, PhD; Professor, Research Office, School of Medicine, University of Pretoria. Phone: 083 293 0065. Address: Research Office, School of Medicine, University of Pretoria, Pretoria 0002. Email: piet.becker@up.ac.za; ORCID: 0000-0002-9384-6472
ABSTRACT
INTRODUCTION: Supernumerary teeth (SNT) are often associated with malocclusions. Data on SNT in the South African population are not well documented
OBJECTIVE: To determine the prevalence, distribution of characteristics and any associated complications of SNT in a South African sample of dental patients
DESIGN: The study was retrospective, cross-sectional and descriptive
METHOD: Orthopantomographs of 12,005 dental patients were reviewed for the presence of SNT. The number, morphology, location, eruption status and orientation of SNT were assessed. Associated orthodontic problems were noted
RESULTS: The prevalence rate was 2.48%. No sexual dimorphism in the distribution of SNT was noted. Types of SNT tabulated were: supplementary, conical, tuberculate and odontoma. Maxilla demonstrated a higher predilection for SNT. Variation in the distribution of SNT in the anterior, premolar and molar regions in each jaw and across jaws was statistically significant. Relationship of eruption status to the morphology and orientation of SNT was of significance. Malocclusions noted were displacement and impaction of adjacent teeth
CONCLUSION: From an orthodontic perspective, presence of SNT may compromise tooth movement and space closure in patients. Additionally, as majority of SNT in this population were in the maxillary molar and mandibular premolar regions, caution is advised when planning the placement of orthodontic implants in these regions
Keywords: Supernumerary tooth, panoramic radiographs, prevalence, morphology, location, eruption status, orientation, orthodontic complications.
INTRODUCTION
Supernumerary teeth (SNT) are defined as teeth in excess of the normal dental complement (more than 32 permanent teeth or more than 20 primary teeth),1 and present as developmental anomalies that may be responsible for malocclusion in an individual. Many theories have been put forward to explain this developmental abnormality, including atavism (evolutionary throwback), hyperactivity of the dental lamina, tooth germ dichotomy, and genetic and environmental factors.2 Knowledge about the prevalence, characteristics and effects of SNT in a given population helps clinicians to improve their diagnostic acumen and efficiently streamline treatment strategies.
Supernumerary teeth (SNT) can occur singly or in multiples, unilaterally or bilaterally, erupted or unerupted and within a single jaw or in both jaws.3 SNT are classified according to their morphology as either conical, supplemental, tuberculate, or as an odontoma.4,5
Conical supernumerary teeth are peg-shaped small teeth with root development concurrent or ahead of the adjacent permanent teeth. The most common type of conical SNT, found between the central incisors in the premaxillary region and known as the mesiodens, may cause many orthodontic problems such as displacement, rotation or impaction of adjacent teeth.6,7
Supplemental SNT are usually found at the end of a tooth series as duplications of teeth in the normal dentition. The most common type of supplemental SNT is the maxillary lateral incisor. Additionally, supplemental premolars and molars have also been reported.8,9 In some cases, these supplemental premolars and molars develop after the formation of the permanent dentition and are thought to be representative of a third dentition.2
Tuberculate SNT are large and barrel-shaped with multiple cusps or tubercles. The root development is delayed when compared with adjacent teeth. They are mostly found unerupted in the palatal aspect of the maxillary central incisors and are known to cause impaction of those teeth.10 Odontomas are described as an additional category of SNT.4,5 An odontoma is usually considered to be a hamartomatous malformation of enamel, dentin, cementum and pulpal tissue, rather than a neoplasm. Odontomas rarely erupt into the oral cavity.11
Not only the morphology but also the orientation of SNT appear to play a role in their eruption.10 It was noted that approximately 25% of SNT erupt into the oral cavity while the rest remain unerupted.11 Regardless of their eruption status, supernumerary teeth may be associated with many complications such as spacing, ectopic eruption and/or root resorption of adjacent teeth, formation of pathologic cysts, or root dilacerations.4,5,12,13 Conversely, SNT may remain asymptomatic without any clinical manifestations and are often discovered by chance during a routine radiographic examination.10
A literature survey disclosed a paucity of data on SNT in the South African population. A publication that could have some relevance in this topic was that of Van der Merwe and Steyn14 who reported on the incidence of SNT in the skeletal remains of a 19th-century mining community from Kimberley, South Africa. Historical and standard anthropometric records indicated that these were predominantly male migrant workers suffering from a myriad of medical conditions and traumatic injuries who had died around 1897 and 1900 and were given pauper burials outside the fenced-off Gladstone cemetery in Kimberley. It is noteworthy that not a single individual in the Gladstone cemetery sample presented with the commonly observed anterior SNT.
The study of Van der Merwe and Steyn14 on their limited (n=89) and more than a century-old, sample, demonstrated a distribution pattern of SNT atypical to what has previously been reported.5,6,7 Anecdotal and unpublished observations by clinicians of patients in various hospitals in the Gauteng province of South Africa further support the view that the distribution of SNT in this population group follow a different pattern. The observations indicated that whilst SNT were often noted in the posterior regions, they also occurred in the premaxilla.
The aim of this study, therefore, was to determine the prevalence, characteristics and effects of SNT in South African dental patients. The district hospital where this study was conducted is one of the three main government hospitals that cater for the dental needs of the general South African population. Therefore, the sample drawn from this pool may be considered representative of the local dental population inhabiting north-western Gauteng and the adjacent Northwest province. The results of this study may alert clinicians to the possible presence of SNT and influence the diagnosis and treatment planning of affected individuals. The data may contribute to future research projects on the phenomenon.
MATERIALS AND METHOD
SNT were assessed using panoramic radiographs, a standard diagnostic radiographic tool used at the tertiary general dental hospital in the Gauteng province where this study was conducted. The orthopantomographic method of assessing SNT was chosen because the majority of SNT fail to erupt and may not cause any dental problems in affected individuals and are often discovered as an incidental pathologic finding in initial diagnostic radiographs of patients presenting with an entirely different chief complaint.
Panoramic radiographs of South African dental patients who had presented for general dental treatment during the time interval December 2018 to July 2020, were scrutinised for the presence of SNT. The inclusion criteria for the sample were as follows: 1) good quality panoramic radiographs, clearly portraying the dentition and adjoining structures, and 2) the age range of the subjects ranging from the first decade to the fourth decade of life. Exclusion criteria were: 1) radiographs of patients with syndromes that exhibited a known predilection to SNT e.g. cleft lip and palate; an exclusion criteria that was followed to get a true representation of the prevalence of SNT in this study population and a protocol supported in other epidemiological studies of SNT1,3,15,16 and 2) individuals without the full complement of teeth expected at their respective ages. The patient's hospital files were evaluated to ensure that the inclusion/exclusion criteria were met. Overall, 12,005 panoramic radiographs of patients were screened. A total of 298 patients with 473 SNT were catalogued.
The prevalence of SNT in the sample was determined by noting the number of individuals affected by this anomaly. Associated variables such as the number of SNT, the morphology of SNT, distribution in males and females of the selected population, the affected jaw and region, the eruption status, morphology of SNT, relationship between morphological characteristics and the orientation of SNT to eruption status, as well as any complications associated with the presence of SNT, were also recorded, as listed and described (where needed) in Table I.
Statistical analysis of the data was performed using the Stata Release 16 package (Copyright 1985-2019, StataCorp, Texas, USA). Pearson's chi-square test was utilised to compare categories of one variable with respect to the distribution over the categories of a second variable. Differences between variables were assessed using Pearson's chi-squared test at the 0.05 level of confidence. Patients signed a pre-treatment disclaimer consenting to the use of their records for research purposes.
This study was approved by the Research Ethics Committee of the Sefako Makgatho Health Sciences University (SMUREC/D/306/2018) and was conducted following the Declaration of Helsinki principles. The study design was retrospective and cross-sectional in nature.
RESULTS
A total of 298 patients with 473 SNT were catalogued. The prevalence of SNT in this sample population was 2.48% (298/12005) with a 95% confidence interval (2.21%; 2.78%). For practical purposes, the gender distribution of patients presenting with this anomaly was equal (50.32% males and 49.68% females).
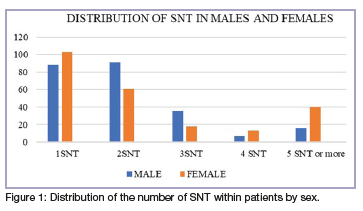
Males and females did not differ significantly (p=0.1265) concerning the distribution of the number of SNT (1,2,3,4, 5 or more SNT) as illustrated in Figure 1.
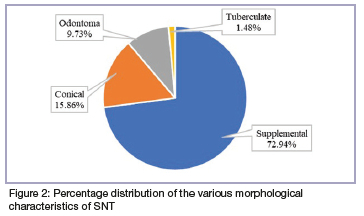
Supplemental morphology was found to be the most common type of SNT (72.94%). SNT with conical morphology accounted for 15.86% of cases. The tuberculate variety of SNT (1.48%) was the most uncommon. All SNT cases that did not fall into the above three categories were grouped into the category: Odontoma, which accounted for 9.73% of the total sample. Figure 2 displays the morphological distribution of SNT in this study sample.
The distribution of SNT of varying morphology in both sexes was investigated. A design-based analysis which took into consideration that an individual within the sample may present with single or multiple numbers of SNT with varying morphology, revealed that the distributions of SNT with different morphologies in males and females were not statistically significant (p=0.9158).
The variance in the location of SNT in each jaw was also investigated. It was found that the upper jaw presented with a higher incidence of SNT when compared with the lower jaw; Maxilla: 317 vs Mandible: 156.
The distributions of SNT differed statistically significantly (p=0.0000) with regard to the various locations within each jaw (see Figure 3). In the maxilla, the molar region had the highest number of SNT (66.56%) followed by the anterior region (23%). The maxillary premolar region recorded the lowest number of SNT (10.41%). In the mandible, this distribution pattern was altered with the premolar region recording the highest number of SNT (64.74%), followed by the molar region (26.28%). The anterior region recorded the lowest number of SNT (8.97%).
The distribution of SNT also varied statistically significantly (p=0.0000) according to the various regions (see Table II). In the anterior region, the maxillary jaw (83.91%) presented with an increased number of SNT when compared with the mandible (16.09%).
In the premolar region, this condition was reversed with the mandible (75.37%) demonstrating a higher percentage of SNT than the maxilla (24.63%). The presence of SNT was again higher in the region of the molar teeth in the upper jaw (83.73%) when compared with the same region in the lower jaw (16.27%).
Only 27% of the SNT in this sample had erupted into the oral cavity. The relationship between the morphology of SNT and the variation in eruption status was explored (see Figure 4) and yielded significant results (p=0.0000). When the morphologies of the erupted SNT versus non-erupted SNT were examined, it was found that 69.53% of the erupted SNT were of the supplementary type. The conical type accounted for 25%, while the tuberculate and SNT of indeterminate shape (category: odontoma) combined, made up the remaining 5.47%.
The relationship between the orientation of the long axis of SNT and variation in eruption status was explored and shown to be statistically significant (p=0.0000). It was found that the highest number of erupted SNT (63.28%) had vertical orientations, followed by SNT with oblique orientations (33.59%). SNT with inverted orientations failed to erupt into the oral cavity. In this sample, only 3.13% of SNT with no discernible long axes, such as those found in the odontoma category, erupted into the oral cavity.
Regardless of their status of eruption, 45.88% of the SNT was associated with local aberrations in the dentition of the affected subjects (p=0.0551). The various problems catalogued were the spacing of teeth, displacement of teeth, impactions, and complications such as the formation of cysts.
Displacement of teeth (p= 0.0002) and impaction of adjacent teeth (p=0.0006) were the most significant problems encountered.
The age distribution of subjects diagnosed with SNT was also recorded. It was seen that the maximum number of SNT were recorded in patients belonging to the third (f=194) decade of life.
Region-wise (anterior, premolar and molar regions) there was a difference in the age ranges of subjects in whom SNT was detected (see Table III). In the anterior regions of the jaws, the maximum number of SNT (Maxillary:36 vs Mandibular:9) was recorded in subjects whose ages belonged to the second decade of life (11-20years)
From the frequency table it can be seen that the highest number of SNT (f=38) seen in the mandibular premolar region was distributed equally in the second and third decades of life, whereas for maxillary premolars the highest frequency(f=17) of SNT was in the third decade of life. In the molar regions, the frequency of SNT was highest in the third decade for the maxillary molars (f=103) although for the mandibular molars the highest frequency of SNT (f=20) was seen in the second decade of life.
Inter- and intra-examiner reliability
To assess the intra-reader strength of agreement, 60 radiographs were randomly selected and re-evaluated using Cohen's kappa statistic value. The kappa statistic value of 0.96 demonstrates an excellent strength of agreement. To determine inter-examiner reliability, 10 radiographs were reassessed by another researcher and compared. The kappa value of 0.75 revealed that the inter-rater agreement was also excellent.
DISCUSSION
A panoramic radiograph is a two-dimensional (2D) radiograph that can detect pathologies or abnormalities in the dental arches and associated structures and has been used as an essential diagnostic tool for more than half a century. 17.Despite its various limitations such as magnification and superimposition of images, panoramic radiographs are still generally used in almost all dental specialities for overall screening.18 In orthodontics, panoramic radiographs are taken routinely to detect malocclusions, gather information about the present, missing or additional number of teeth, assess axial inclinations, evaluate mesiodistal root angulations, and as a guide in establishing proper root position 6,19-22
The rationale of this retrospective panoramic radiographic study was to provide some understanding of the prevalence and characteristics of SNT in a contemporary, living cross-sectional sample of the South African population. The role of SNT played in the malocclusion of an individual was also explored by noting the various orthodontic problems in affected individuals.
Malocclusions caused by SNT such as delayed eruption, impacted teeth, crowding or a diastema in the anterior region6 may negatively affect the aesthetics, mastication and speech of children. Furthermore, supernumerary teeth are associated with many complications such as ectopic eruption and/ or root resorption of adjacent teeth, formation of pathologic cysts or root dilacerations.4,5,12,13 Early detection and orthodontic and/or surgical interventions are of significant value in reducing future clinical problems and establishing proper occlusion of adjacent permanent teeth.23
The prevalence of SNT in this sample was 2.48%. This was comparable to the prevalence rate of 0.1-3.8% quoted in studies on Caucasian populations 4,10 and less than the 2.73.4% recorded for Asian and Japanese populations.9,24 The prevalence was also lower than the rate of 6.7% found in the skeletal remains of a mining community in Kimberley, South Africa.14 Differences in prevalence among populations may be attributed to variations in sampling method and sample sizes, age of subjects, diagnostic tools used and geographic area.
Based on their morphology, SNT were broadly classified into four different types in this study. It was found that most of the SNT were of the supplementary type (72.94%), followed by conical (15.86%), odontoma (10%) and the tuberculate (1.48%) types. This finding was not in congruence with other published reports3,6,25,26 on SNT in which the most prevalent morphology recorded for SNT was of the conical type.
The distribution of SNT in this study did not demonstrate any sexual dimorphism. This finding is at variance with many studies published in the literature, which indicate that males were more affected than females, with a relative frequency of around 1.5:1 or higher.1,10,27,28
A predilection of SNT for the maxillary jaw, as reported by Khandelwal29 among others3,30 was also noted in this study. When considering specific sites within the jaws, the tendency of the majority of SNT to occur in the posterior sections of the jaws, mainly the maxillary molar region and the mandibular premolar region in this study, was a finding similar to the results reported by Hajmohammadi et al,.8 in an Iranian sample. In stark contrast, many studies on other populations in various geographical regions reported the premaxillary or anterior region as the most common site for the occurrence of SNT. 4,7,31
Our results resonate with the findings of other researchers in the literature studied, who state that the majority of supernumerary premolars (75%) are found in the mandible.31,32 Similarly, a high incidence of SNT in the mandibular premolar region was noted in the Nigerian population.33,34 The question arises whether predilection of SNT for the mandibular premolar regions of the jaws is a tendency seen predominantly in population groups within a specific geographic area. Only future research within the African continent could provide some clarity on this matter.
Many reports in the literature testify to the presence of late-developing supernumerary premolars in patients.34,35 In our study the majority of SNT in the mandibular premolar regions were detected in the second and third decades while in the maxillary premolar region, the majority were detected in the third decade. The presence of SNT in the premolar region may compromise orthodontic attempts at tooth movement and space closure. In such instances, it is advisable to extract these extra teeth. The inter-radicular spaces between the maxillary second premolar and first molar, the maxillary first molar and second molar and the mandibular first and second premolars, and the mandibular first molar and second molars are cited as good implant sites for the placement of orthodontic mini-implants when additional orthodontic anchorage is needed.36,37 The high incidence of SNT in the maxillary molar and mandibular premolar regions of the South African population may jeopardise orthodontic mini-implant placement in these areas. Clinicians should proceed with caution in such instances, as the stability of the implant may be compromised due to insufficient inter-radicular clearance owing to the presence of extra teeth.
The majority of the SNT recorded in this study remained unerupted, an observation supported in other studies as well.3,8,30 In agreement with the findings of a Taiwanese study,38 the highest number of erupted SNT belonged to the supplemental category. The majority of the erupted SNT (63.28%) had a normal orientation, an observation supported in other studies as well.28,39
SNT may be associated with dental malocclusions and complications.6,40
Many studies support the use of panoramic radiographs as an initial screening tool to identify dental anomalies and related orthodontic complications16,20-22,41. Accordingly, this radiographic study looked at dental malocclusions6,13,23,40 and orthodontic complications38,39 related to SNT such as displacement, impaction, spacing of affected teeth and formation of dentigerous cysts that are readily assessed on panoramic radiographs. However, it is important to note that, panoramic radiographs have limitations and should be used in conjunction with other diagnostic tools such as a clinical examination, dental history and study models to fully evaluate and form a comprehensive diagnosis of a patient's orthodontic problems and needs.
Displacement and impaction of adjacent permanent teeth were the most pertinent problems encountered in this study population. When it has been established that SNT is the main cause for the impaction of teeth, removal of the SNT is warranted. This may be performed in isolation or in conjunction with surgical exposure of the impacted tooth. If there is adequate space in the dental arch, spontaneous eruption and alignment of the impacted tooth may occur, while in some cases, orthodontic intervention may be necessary. Early diagnosis of SNT plays an important role in this regard, as teeth with more advanced root development are less likely to erupt spontaneously. Therefore, when such clinical problems are seen in patients, it would be advisable to conduct a radiological examination to determine whether SNT is the cause and to determine the extent of root development.
It is interesting to note that the majority of SNT in the anterior region was recorded in subjects in their second decade (1120 years) of life. Anecdotal observations by orthodontists indicate that this is the typical age range (11-20 years) when most individuals seek orthodontic treatment for matters affecting their dental appearance and function. The highest number of SNT in the posterior regions was detected in the third decade of life. Perhaps this might have been due to the fact any malocclusion caused by SNT in the posterior region is of less importance to an affected individual when compared to the anterior regions, where aesthetics play an important role. There are also reports of late developing supernumerary teeth that develop much later than the normal dentition; these are usually found in the premolar region.31,35 These factors might account for the older age range of subjects detected with posterior SNT. Future research on SNT may help to provide greater insight into this observation.
The authors acknowledge that the under-representation of SNT may have occurred in this sample due to various factors. For instance, patients might have undergone a supernumerary tooth extraction or had a normal tooth mistakenly extracted as a supernumerary tooth in the past. Consequently, they may have presented to the hospital with a "normal" complement of teeth, leading to an underestimation of the prevalence of SNT in the sample It is critical to consider these potential sources of bias when interpreting the study's findings.
Nevertheless, the current study provides important insights into the prevalence and distribution of SNT in a contemporary South African patient population and contributes to important information in the field of SNT research.
CONCLUSION
Although the prevalence of SNT was similar to those data generally recorded in the literature for other populations, the distribution of SNT within the jaws showed a distinct departure from other studies, in that the majority of the SNT were in the maxillary molar and mandibular premolar regions.
Only 27% of the SNT had erupted in the oral cavity which again highlights the importance of diagnostic radiographs to detect the presence of SNT. The relationship between morphology and orientation of SNT on eruption status revealed associations of significance. In this study, the majority of the erupted SNT were of the supplemental type. SNT with vertical orientation were more likely to erupt into the oral cavity, while SNT with inverted orientation did not erupt at all.
Common dental problems associated with this developmental defect were displacement of teeth and impaction of adjacent permanent teeth. The role of SNT must therefore be included in the differential diagnosis of such cases. During the treatment phase, the presence of SNT may hinder orthodontic tooth movement and space closure. In addition, due to the increased incidence of SNT in the maxillary molar and mandibular premolar region, caution is advised when planning the placement of implants for anchorage reinforcement in this population group.
Conflict of interest
None.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
REFERENCES
1. McBeain M, Miloro M. Characteristics of supernumerary Teeth in nonsyndromic population in an urban dental School Setting. J Maxillofac Surg. 2018; 76(5): 933-8. https://doi.org/10.1016/j.joms.2017.10.013 [ Links ]
2. Wang XP, Fan J. Molecular genetics of supernumerary tooth formation. Genesis 2011; 49(4): 261-77. https://onlinelibrary.wiley.com/doi/10.1002/dvg.20715 [ Links ]
3. Chou ST, Chang HP, Yang YH, et al,. Characteristics of supernumerary teeth among nonsyndromic dental patients. J Dent Sci. 2015; 10(2): 133-8. https://linkinghub.elsevier.com/retrieve/pii/S1991790214000063 [ Links ]
4. Garvey MT, Barry HJ, Blake M. Supernumerary teeth - an overview of classification, diagnosis and management. J Can Dent Assoc. 1999; 65: 612-6. [ Links ]
5. Mossaz J, Kloukos D, Pandis N, Suter VGA, Katsaros C, Bornstein MM. Morphologic characteristics, location, and associated complications of maxillary and mandibular supernumerary teeth as evaluated using cone beam computed tomography. Eur J Orthod. 2014; 36(6): 708-18 [ Links ]
6. Pérez IE, Chávez AK, Ponce D. Prevalence of supernumerary teeth on panoramic radiographs in a non-adult Peruvian sample. Int J Odontostomat. 2014; 8(3): 37783. DOI.10.4067/s0718-381x2014000300010 [ Links ]
7. Amini F, Rakhshan V, Jamalzadeh S. Prevalence and pattern of accessory teeth (hyperdontia) in permanent dentition of Iranian orthodontic patients. Iran J Public Health. 2013; 42(11): 1259-65. [ Links ]
8. Hajmohammadi E, Najirad S, Mikaeili H, Kamran A. Epidemiology of supernumerary teeth in 5000 radiography films: investigation of patients referring to the clinics of Ardabil in 2015-2020. Int J Dent. 2021; (2021): 1-7. DOI: 10.1155/2021/6669436 [ Links ]
9. Niswander JD, Sujaku C. Congenital anomalies of teeth in Japanese children. Am J Phys Anthropol. 1963; 21(4): 569-74. [ Links ]
10. Rajab LD, Hamdan MAM. Supernumerary teeth: Review of the literature and a survey of 152 cases. Int J Paediatr Dent. 2002; 12(4): 244-54. [ Links ]
11. McKibben DR, Brearley LJ. Radiographic determination of the prevalence of selected dental anomalies in children. J Int Assoc Dent Child. 1971; 38: 390-8. [ Links ]
12. Asaumi JI, Shibata Y, Yanagi Y, et al,. Radiographic examination of mesiodens and their associated complications. Dentomaxillofac Radiol. 2004; 33(2): 125-7. [ Links ]
13. Hattab F, Yassin O, Rawashdeh M. Supernumerary teeth: Report of three cases and review of the literature. ASDC J Dent Child. 1994; 61(5-6): 382-93. [ Links ]
14. Van der Merwe AE, Steyn M. A report on the high incidence of supernumerary teeth in skeletal remains from a 19th century mining community from Kimberley, South Africa. S Afr Dent J. 2009; 64(4): 162-6. [ Links ]
15. Kumar DK, Gopal KS. An epidemiological study on supernumerary teeth: A survey on 5,000 people. J Clin Diagnostic Res. 2013;7(7): 1504-7. DOI: 10.7860/ JCDR/2013/4373.3174 [ Links ]
16. Wagner VP, Arrué T, Hilgert E, Arús NA, da Silveira HL, Martins MD, et al,. Prevalence and distribution of dental anomalies in a paediatric population based on panoramic radiographs analysis. Eur J Paediatr Dent. 2020;21(4): 292-8. DOI: 10.23804/ejpd.2020.21.04.7 [ Links ]
17. Hallikainen D. History of panoramic radiography. Acta radiologica. 1996; 37(3):441-5. [ Links ]
18. Pittayapat P, Willems G, Alqerban A, Coucke W, Ribeiro-Rotta RF, Souza PC, et al,. Agreement between cone beam computed tomography images and panoramic radiographs for initial orthodontic evaluation. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014; 117(1): 111-9. DOI: 10.1016/j.oooo.2013.10.016 [ Links ]
19. Stramotas S, Geenty PJ, Petocz P, Darendeliler MA. Accuracy of linear and angular measurements on panoramic radiographs taken at various positions in vitro. Eur J Orthod. 2002; (24): 43-52. [ Links ]
20. Goncalves-Filho AJ, Moda LB, Oliveira RP, Ribeiro AL, Pinheiro JJ, Alver-Junior SM. Prevalence of dental anomalies on panoramic radiographs in a population of the state of Pará, Brazil. Indian J Dent Res. 2014; 25(5): 648-52. DOI: 10.4103/09709290.147115 [ Links ]
21. Pallikaraki G, Sifakakis I, Gizani S, Makou M, Mitsea A. Developmental dental anomalies assessed by panoramic radiographs in a Greek orthodontic population sample. Eur Arch Paediatr Dent. 2020; 21(2): 223-8. DOI: 10.1007/s40368-019-00476-y [ Links ]
22. Hlongwa P, Moshaoa MAL, Musemwa C, Khammissa RAG. Incidental Pathologic Findings from orthodontic pretreatment panoramic radiographs. Int J Environ Res Public Health. 2023; 20(4): 3479. DOI: 10.3390/ijerph20043479 [ Links ]
23. Celikoglu M, Kamak H, Oktay H. Prevalence and characteristics of supernumerary teeth in a non-syndrome Turkish population: associated pathologies and proposed treatment. Med Oral Patol Oral Cir Bucal. 2010; 15(4). 575-578. DOI: 10.4317/medoral.15.e575 [ Links ]
24. Davis PJ. Hypodontia and hyperdontia of permanent teeth in Hong Kong schoolchildren. Community Dent Oral Epidemiol. 1987; 15(4): 218-21. [ Links ]
25. Anthonappa RP, Omer RSM, King NM. Characteristics of 283 supernumerary teeth in southern Chinese children. Oral Surg Oral Med Oral Pathol Oral Radiol. 2008; 105(6): 48-54. DOI: 10.1016/j.tripleo.2008.01.035 [ Links ]
26. Yassin OM, Hamori E. Characteristics, clinical features and treatment of supernumerary teeth. J Clin Pediatr Dent. 2009; 33(3): 247-50. [ Links ]
27. Chalakkal P, Krishnan R, De Souza N, Da Costa GC. A rare occurrence of supplementary maxillary lateral incisors and a detailed review on supernumerary teeth. J Oral Maxillofac Pathol. 2018; 22(1): 149-156. DOI: 10.4103/jomfp.JOMFP_213_15 [ Links ]
28. Anegundi R, Tegginmani V, Battepati P, et al,. Prevalence and characteristics of supernumerary teeth in a non-syndromic South Indian pediatric population. J Indian Soc Pedod Prev Dent. 2014; 32(1): 9-12. DOI: 10.4103/0970-4388.127041 [ Links ]
29. Khandelwal P, Rai AB, Bulgannawar B, Hajira N, Masih A, Jyani A. Prevalence, characteristics, and morphology of supernumerary teeth among patients visiting a dental institution in Rajasthan. Contemp Clin Dent. 2018; 9(3): 349-56. DOI: 10.4103/CCD.CCD_31_18 [ Links ]
30. Leco Berrocal M, Martín Morales JF, Martinez Gonzalez JM. An observational study of the frequency of supernumerary teeth in a population of 2000 patients. Med Oral Patol Oral Cir Bucal. 2007; 12(2): 96-100. [ Links ]
31. Yusof WZ. Non-syndrome multiple supernumerary teeth: Literature review. J Can Dent Assoc. 1990; 56(2): 147-9. [ Links ]
32. Hyun HK, Lee SJ, Ahn BD, et al,. Nonsyndromic multiple mandibular supernumerary premolars. J Oral Maxillofac Surg. 2008; (66): 1366-9. DOI: 10.1016/j.joms.2007.08.028 [ Links ]
33. Umweni AA, Osunbor GE. Nonsyndrome multiple supernumerary teeth in Nigerians. Odontostomatol Trop. 2002; 25(99): 43-8. [ Links ]
34. Bello S, Olatunbosun W, Adeoye J, Adebayo A, Ikimi N. Prevalence and presentation of hyperdontia in a nonsyndromic, mixed Nigerian population. J Clin Exp Dent. 2019; 11(10): 930-6. DOI: 10.4317/jced.55767 [ Links ]
35. Paduano S, Rongo R, Lucchese A, Aiello D, Michelotti A, Grippaudo C. Late-developing supernumerary premolars: analysis of different therapeutic approaches. Case Rep Dent. 2016;2016. DOI: 10.1155/2016/2020489 [ Links ]
36. Poggio PM, Incorvati C, Velo S, Carano A. 'Safe zones': A guide for miniscrew positioning in the maxillary and mandibular arch. Angle Orthod. 2006; 76(2): 191-7. DOI: 10.1043/0003-3219(2006)076[0191:SZAGFM]2.0.CO;2 [ Links ]
37. Silvestrini Biavati A, Tecco S, Migiliorati M, et al,. Three-dimensional tomographic mapping related to primary stability and structural miniscrew characteristics. Orthod Craniofacial Res. 2011; 14: 88-99. DOI: 10.111/j.1601-6343.2011.01512.x [ Links ]
38. Liu JF. Characteristics of premaxillary supernumerary teeth: a survey of 112 cases. ASDC J Dent Child. 1995; 62(4): 262-5. [ Links ]
39. Ata-Ali F, Ata-Ali J, Penarrocha-Oltra D, Penarrocha-Diago M. Prevalence, etiology, diagnosis, treatment and complications of supernumerary teeth. J Clin Exp Dent. 2014; 6(4): 414-8. DOI: 10.4317/JCED.51499 [ Links ]
40. Syriac G, Joseph E, Rupesh S, Philip J, Cherian S, Mathew J. Prevalence, characteristics, and complications of supernumerary teeth in nonsyndromic pediatric population of South India: A clinical and radiographic study. J Pharm Bioallied Sci. 2017; 9(5): 231-6. DOI: 10.4103/jpbs.JPBS_154_17 [ Links ]
41. Farman AG. Panoramic radiographic assessment in Orthodontics. In: Panoramic Radiology: Seminars on Maxillofacial Imaging and Interpretation Springer Berlin Heidelberg; 2007; 83-9. DOI: 10.1007/978-3-540-46230-9_8 [ Links ]
 Correspondence:
Correspondence:
Dr E Thomas
Tel: 072 836 5149
Address: Post Net Suite 1007, Private Bag X9, Benmore 2010, Email: lizathomas67@gmail.com
Author contributions
E Thomas: conception and design of the study, acquisition of data and write up - 70%
PJ Becker: design of the study, interpretation of data and writing of the article - 15%
AC Oettlé: interpretation of data, article structure and writing of the article - 15%
Acknowledgements
1. The corresponding author would like to thank Prof MPS Sethusa, Head, Department of Orthodontics, School of Oral Health Sciences, Sefako Makgatho Health Sciences University for his support and encouragement during the entire duration of this study.
2. The authors would like to acknowledge Ms Ciska van der Schoor for her technical assistance, supported by the Bakeng se Afrika project 597924-EPP-1-2018-1-ZA-EPPKA2-CBHE-JP, an Erasmus+ programme of the EU.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}