










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.78 no.2 Johannesburg Mar. 2023
RESEARCH
Perceptions of oral health practitioners regarding the long-term effects of service learning; a qualitative study
MG PhalwaneI; B MthelebofuII; P SodoIII
IDepartment of Community Dentistry, School of Oral Health Sciences, Sefako Makgatho Health Sciences University, Pretoria, South Africa. ORCID: 0000-0002-2977-9092
IIDepartment of Surgery, Clinical Trial Laboratory, School of Medicine, Sefako Makgatho Health Sciences University, Pretoria, South Africa. ORCID: 0000-0003-4224-142X
IIISchool of Clinical Medicine, Faculty of Health Sciences, University of Witwatersrand, Johannesburg, South Africa. ORCID: 0000-0002-2542-6038
ABSTRACT
INTRODUCTION: The long-term effects of service learning (SL) have not been explored in the oral health field. Such information has the potential to provide useful feedback to dental educators regarding the effectiveness and impact of SL. This would be relevant in the South African context of inequality and poor access to care
Aim and objective: To explore the perceptions of oral health professionals from an academic institution regarding the long-term effects of SL.
METHODS: A case study design was used. Semi-structured interviews were conducted. A total of 22 participants from the Bachelor of Dental Therapy, Bachelor of Dental Surgery, and Bachelor of Oral Hygiene participated in the study
RESULTS: The participants indicated that SL is a worthy activity that exposed them to the real world of dentistry and provided them with the exposure that prepared them for work actualities. Four major themes emerged; namely, personal qualities, relationship building, challenges related to SL and strategies to improve the outcomes
CONCLUSION: Participants found SL to be beneficial in their professional development and practice although they highlighted some challenges in practice. They recommended the improvement and upgrading of the SL program, as well as further research on SL approaches in other environments
Keywords: Service Learning, Community Engagements, Perceptions, Academic Enhancement, Civic Responsibility, Interpersonal Skills, and Learning.
INTRODUCTION
The benefits of Service Learning (SL) in Dental Education are well-known. Evaluations of SL are generally based on the experiences and opinions of undergraduate students. Unfortunately, the views of dental graduates and working dentists regarding their SL experience in dental school remain relatively unexplored. Such information has the potential to provide useful feedback to dental educators regarding the effectiveness and impact of SL. This would be especially relevant in the South African context of inequality and a lack of access to care for large parts of the population.
SL, according to several authors1,2 may be unpacked as an educational approach that combines learning objectives with community service in order to enable students at an early stage of their academic development to provide/improve services to communities in areas where governments fail to serve, and provide a pragmatic, progressive learning experience while meeting societal needs.
Community-based education (CBE) on the other hand is "field-based experiential learning" with community partners as an instructional strategy. CBE is part of the work-integrated learning (WIL) approaches such as SL. The idea is to give students direct experience with issues they are studying in the curriculum and with ongoing efforts to analyse and solve problems in the community. A key element in these programs is the opportunity for students to apply what they are learning in real-world settings and reflect in a classroom setting on their service experiences. These programs model the idea that giving something back to the community is an important University outcome, and that working with community partners is good preparation for citizenship, work, and life.3 Similar benefits were reported in a four-year study conducted at the dental Academy of the University of Portsmouth, London where students* responses to the CBE were evaluated. The findings included quality, more understanding, self-confidence, and personal growth. Furthermore, students felt empowered due to the autonomy granted during training.4 The learning is usually guided by using various models for structured reflections like the Gibb's (1988) model.5 Self-reflection is a cognitive process as part of self-regulation whereby a learner reviews current world views and or performance in order to adapt to a more progressive standpoint or execution.6
It is generally assumed that oral health students who undergo SL as a teaching approach during their undergraduate training will develop many other skills like social responsibility, teamwork, communication, problem-solving, emotional intelligence, maturity, and personal growth as well as civic responsibility by connecting academic content and clinical experiences.7,8 These connections bring about academic enhancement among the students, as well as further strengthening SL skills.9 These skills may also be viewed as matching the 'market' demands and increasing opportunities for employment in the country.10
Skills acquired include interdisciplinary thinking and collaborations with colleagues, improved interactions, and positive attitudes towards serving the underserved communities.11 Students have been found to value outreach educational experiences, particularly when they are afforded certain responsibilities. Confidence levels get uplifted, and a sense of professional development ensues.4,12 As it occurs In other parts of the globe, Higher Education Institution (HEI) in Australia send their students to a SL excursion where they stay in the community for two weeks to get the true feel of a rural environment.13 Students reported that their lives changed. They developed empathetic skills, endurance and resilience, patient communication as well as the heart to help the poor. According to Postma et al,. social responsibility and a desire to serve under-privileged communities are prominent outcomes of SL as reported by final year oral healthcare students.14 SL in the rural settings proved to bring about pleasant outcomes to communities.
Studies conducted in South Africa, confirm the above elements as contributing to the benefits that SL offers to student learning. In agreement with several countries, Bhayat, Vergotine, Yengopal, and Rudolph (2011) allude to the fact that both medical and dental training benefit from SL.15 The University of Witwatersrand has been sending oral health students to the Phelophepa Health Train as well as other Public Oral Health Facilities (POHF) on SL trips. The Phelophepa Health Train is a mobile Primary Health Care (PHC) facility offering Oral Health, Pharmacy, Nursing, Diet, Speech Language and Audiology, and Medical services to rural communities next to designated train stations. HEIs send students from the above disciplines to do SL.
The findings of a South African study conducted among final-year oral health students to determine their SL experiences between 2008 and 2009 revealed that there was improved efficiency in clinical skills, self-awareness and awareness of the community needs and social responsibility. Challenges that these students experienced included strenuous and long working hours as well as non-functional equipment. Gaines-Hanks and Grayman (2009) also conducted a study where they found that SL increased awareness, relational and professional growth as well as increased gratitude among students.16 Postma et al,. in 2016 piloted a Community Service Attitudes Scale on the final year oral health students at Sefako Makgatho Health Science University (SMU), where students displayed a positive attitude towards serving destitute communities after exposure to SL.14 The participants also suggested a need for relevant stakeholders to get involved in the procurement of SL resources and in meeting community needs. The impeding challenge was a quota-driven dental training.
Although the local studies provide valuable information in the local context, evaluations were focused on undergraduate students' perceptions only. Almost all studies conducted both locally and internationally evaluate perceptions of students towards SL, but we have not found any studies that have followed-up on these students after graduation as professionals in practice, that evaluate the perceptions of oral health professionals regarding how they applied the knowledge and skills acquired during oral health academic training. These South African studies have therefore highlighted the need to further investigate the usefulness of SL in oral health practice. Therefore, in this study we aim to further explore the long-term influence of SL on oral healthcare professionals, to gain a better understanding of how SL experienced during undergraduate training may develop social responsiveness of practitioners beyond graduation.
METHODS
This was an exploratory study that was conducted within a phenomenological qualitative approach. Twenty-two participants were included in the study, which comprised BDS (Dentistry), BDent Ther (Dental Therapy) and BOH (Oral Hygiene) degree program graduates of a South African University in Gauteng Province.
Semi-structured two-part interviews were administered using either face-to-face or telephonic conversations, depending on feasibility. Questions elicited participants" lived experiences during SL. An interview schedule was developed from questions that were adopted from Shiarella, McCarthy & Tucker, (2000) and Boysen, Salsbury, Derby, & Lawrence, (2016).17,18 The first part consisted of socio-demographic characteristics. The second part captured their experiences regarding the influence of SL during their undergraduate practice as students, before, during and after the placement at the SL projects sites, as well as the impact in post-graduate practice. The information on the interview guide covered theoretical aspects, reflections, detailed information on the SL domains of social responsibility, academic development (which included problem-solving skills) and personal growth (which included interpersonal and leadership skills). English language as the lingua-franca was used. The completed records of participants were filed away before the interviews. The audio recorded data are kept safe on university premises, and the data will be kept for five years.
Thematic Content Analysis was used.19 Data were analysed by creating codes. To ensure a robust process of data interpretation, numerical codes were allocated. Interrelated themes were combined to form categories and themes as detailed in the next section. Permission to conduct the study was granted by the research ethics committee of SU, HREC Reference # S18/05/102.
RESULTS
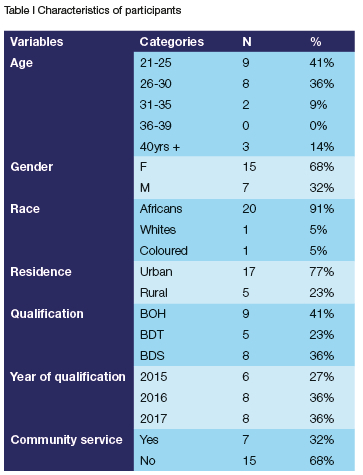
Demographic characteristics of the participants.
Most participants were between 21 and 25 years old (41%), with the fewest being between 31 and 35 years old (9.1%). There were more females than males (68.2%) and vast majority were from the African race (91%). Just above two-thirds (77%) were residing in urban areas. Most participants were oral hygienists (BOH - 41%) and 68% had completed their community service Table 1.
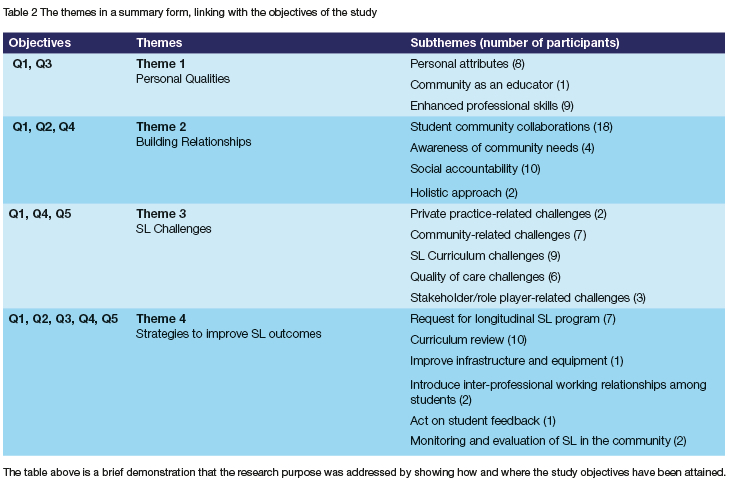
Four major themes emerged in the analysis of data in the study. These are personal qualities, relationship building, challenges related to SL and strategies to improve the outcomes. Themes were further divided into sub-themes. A summary of each theme is presented below. Sub-themes that emerged under personal qualities are personal attributes, self-reflection, character-building, psychological reward, and cultural conscientization.
Theme 1: Personal Qualities
Participants reported experiencing collegial dialogue, which precipitated into professional self-realization, and further ramifications such as maturity, empathy, compassion, humility, emotional intelligence, cultural sensitivity, and on-the-job reward and motivation. Six minor sub-themes emerged under this sub-theme. From a refreshing experience participants enjoyed a sense of professionalism and open-mindedness with which they could improve communication by confidently building rapport with each other, and with community members and faculty. Social constructivism of learning succeeded. They refined clinical skills and were also able to execute independence in decision-making related to the exigencies of their duties and this facilitated efficiency in service delivery. Other profits included: academic and intellectual achievement, positive self-esteem, improved communication, patience, and time management skills.
Theme 2: Building Relationships
Over and above personal attributes that participants reported to have gained during SL, they also expressed that SL is important in building workable relationships that bring about solutions to students, faculty, and communities.
Participants therefore said that SL exposed them to human service in that they became more aware of community needs, became socially accountable to create public awareness regarding oral health problems in communities, which would bring the most needed access to services. They felt morally obliged to plough back and SL became their roadmap to their current practice.
Theme 3: Challenges
Despite all the good that participants reported about SL however, there were also challenges such as poor planning at SMU School of Oral Health Sciences that rendered the program to appear insufficient in some areas. These inadequacies manifested in the following ten sub-themes: less challenging theory, communities' lack of knowledge, limited resources impeding quality of oral health services, unfair assessment of reflective essays, dissatisfaction with political rhetoric coupled with lack of political will to prioritize oral health, lack of professionalism by supervisors, restrictive exposure to patient category and care, lack of follow-up in the curriculum and bloated final year syllabus.
Theme 4: Strategies to Improve Outcomes
Due to the above departmental and community frustrations around SL, participants therefore recommended some upgrading such as SL theory to be reduced and replaced by community work. Many recommended that SL needs to be expanded to local communities, to other departments and disciplines, as well as to introduce it earlier in the academic programme. All 22 participants supported SL approach, but expressed implementation of the following strategies: Expansion of SL to other communities (inside and outside campus) and programs, inclusion of current socio-political issues in the SL curriculum, increase of SL opportunities and introduction of the credit system, maximising the student outreach opportunities, evaluation of treatments in the communities, increase of the number of mobile clinics, inclusion of patient follow-up in the SL curriculum, gradual and simultaneous introduction of theory and practical, increased treatment packages, inclusivity of learning styles during reflections, introduction of video clips during community engagements, prompt student feedback, making SL fun and fashionable, introducing student reflections earlier in the dental program and introduction of inter-professional working relationships among students.
DISCUSSION
This study sought to obtain the views of qualified professionals regarding their SL experience at SMU and is the first of its kind in Dentistry in South Africa. Generally, participants agreed to the benefits of SL in their personal capacities, professional life, and in building relationships with one another, with faculty as well as with communities. However, there were some drawbacks in the sense that some practitioners perceived SL as an unknown and unsupported approach. They complained that a good approach such as SL cannot be applied in one University Department such as Community Dentistry, but needs to be expanded to other departments, faculties, and facilities in the community. Some mentioned that political corruption affects oral healthcare in a bad way. Although our study identified some gaps in SL, it is in line with other studies that reported the positive contributions of SL such as developing social responsibility, teamwork, communication, problem-solving, emotional intelligence, maturity, and personal growth as well as civic responsibility by connecting academic content and clinical experiences.7-10 Participants therefore came up with recommendations to deal with problems that they perceived as stumbling blocks to SL benefits. In addition, time pressures of the curriculum factored a lot in their dissatisfaction and recommendations.
Like other studies, the participants asserted that SL had a positive influence on their personal development as well as In their career practice as oral health professionals.7-10 They view SL as a mechanism for self-reflection, through which a humble character is built. Their new character empowered them to view communities with compassion and sensitivity to different cultures. From these communities they acquired a holistic perspective in their career, integrating the technical/ academic skills with the essential skills for clinical practice that are needed when actual practice takes place. They also indicated to have experienced SL as a pleasurable learning occasion. The exposure to communities and learning to handle them according to their needs and problems beyond the oral health related ones (dental box), seem to have enabled and assisted the professionals to approach the treatment in a more caring way.
The study participants also attested to more added values of SL confidence regarding the management of anxious patients (those who fear the treatment), as well as the children who come for treatment. Further to the above the graduates' general perception about exposure yielded a view that this apprenticeship-cum-induction contributed immensely to their self-concept as practitioners. This is in agreement with other studies that reported SL beneficial in improving patient management skills.7, 8,14,15 The SL exposure enabled the oral health professionals to invest in people's trust by giving best services and encouraged return services and word-of-mouth referrals. The SL-trained oral health practitioners, together with their clients/patients, were also led to an enjoyable service provision because of SL guidance. These professionals' goal was to satisfy the clients under treatment, and moreover, to provide services that could be appreciated, and this was confirmed by the reported excitement of their clients. This approach was also experienced as a connection, linking theory with practice as those trained were able to manage actual work in the field of practice; to understand people more, and to have a desire to assist patients, especially where and when they are needed.
While the main training of the health professionals was in oral health, SL extends to enabling relationships between professionals and communities. It also creates a platform for the experts to empower community members as stated by one of the participants: "Yes, you can't beat yourself to it but at least you have tried, and you are aware of certain situations in the community". It is through the connection, trust, and confidence of the professionals that they can enlighten the community members about oral health treatment and clear some myths among communities. Similar to other studies that reported positive clinical and social outcomes in the community,11,14 the trust was also viewed in our study as enhancing the relationships with people where good rapport would exist between oral practitioners and their patients, hence participants felt morally obliged to assist the community. However, some studies cited the fact that SL being quota-driven, poses a challenge because students tend to focus on completing quota rather than acquiring quality skills.14
Other challenges related to SL were indicated though, as limited training time, limited coverage of communities, inadequate supervision, price limitations (in some instances), poor timing of SL and unfulfilled promises. The participants complained that the duration of SL is very short and denied them adequate exposure because it ends when they start realising the actualities of oral health practice; it blocks actual treatment of patients and prevents perfection as it ends before leading to mastery. The communities visited during SL training are the same every year and are few. This means that exposure does not expand the various groups engaged in SL to varieties of conditions. There was also a complaint about lack of supervision as the trainees are placed alone in the actual work environment and required to make decisions independently, without any experienced professional showing different options and scenarios. Some SL trained oral health practitioners confessed to providing service only to the level that suited the price paid (though only a few occasions). This was a weakness, since even one failure was considered lack of success. The fact that SL takes place only in the final year was viewed as a loss of opportunity for more learning as earlier student years are starved of the reality that could be used to expose the trainees much earlier to actualities of their professions. This could also perfect their skills towards mastery as they would have gone for many years on the SL. The issue of empty promises in which previous SL trainees had indicated to return to treat community members in need, haunted the subsequent SL groups, as they were being blamed for current state. However, the same groups who felt unfairly blamed, seem to have continued the same mistakes of promising without fulfilment.
The weaknesses identified and the desire to provide best practice of SL to the oral health practitioners led to proposals to improve the SL training. There was also a suggestion that while the public sector was receiving support from government, this sector should also be supported equally to ensure that even the communities without government health facilities can benefit from the support.
The findings of this research are quite crucial in improving the SL delivery model. Oral health practitioners can reflect on the SL intentions and adapt their attitudes and practice, especially those who were focused mostly on making profit and lowering service where payments were not adequate. On the other hand, curriculum experts in the relevant departments can also incorporate the suggested proposals in order to improve the SL model in SMU.
In addition, the study was a form of action research, which, according to McNiff (2013), may be defined as research either initiated to solve an immediate problem or a reflective process of progressive-problem-solving managed by individuals working with others in teams.20 This could also work as a component of a community practice aimed at improving the way issues and problems are being addressed. This study was practical in the sense that it managed to confront problems existing in the SL training. It also identified problems that could be resolved and on the verge of producing guidelines for effective practices in the form of recommendations. The problems adjusted can be addressed in different timeframes such as short-term and long-term. Short-term solutions could be implemented by sending oral health students to the SL sites for observation, while ensuring that arrangements are made for future curriculum to integrate SL from earlier years.
CONCLUSION
Participants found SL to be beneficial in their professional development and practices. They pointed out that they appreciated the members of communities and assisted where the communities were unable to pay for their services. They also indicated that they went beyond oral health treatment in some cases, especially after familiarising themselves with the problems and challenges that the communities and the families were experiencing and had to endure. There were still few practitioners who did not fully embrace or appreciate providing full service when money from clients was limited, and thus provided a service that suited the amount of money paid; this is the implied prescription by the current capitalistic system in healthcare. The participants indicated that the academic side of their training was only theory, and that SL was handy in bringing the practical perspective which made them understand the oral practice requirements of their qualifications even better. The challenges in the communities and the real work situation were not reflected anywhere in the academic learning of oral health, but SL was said to have provided that component to an inclusive extent. Furthermore, the SL as offered, beneficial as it was indicated, had limitations of timing and duration, as well as limited coverage to communities. These findings may be useful to adjust and standardize the curriculum at SMU and at all other Oral Health Faculties.
RECOMMENDATIONS
The participants indicated that the academic side of their training was reinforced by SL practice in the community. They emphasized that SL content would be efficient in all respects if it was properly delivered. They also said that SL was convenient in bringing a practical perspective, which made them understand the oral practice requirements of their qualifications. The strengths of SL offered at SMU should be researched qualitatively in a separate study. There should be benchmarking research undertaken by leading higher education institutions. Comparative in-depth studies should be undertaken to determine the areas, which are not adding value to the current SL in SMU in order to ensure that they are removed before any incorporation into the revised curriculum, and SMU should involve community partners in the continual evaluation of the pedagogy as a mission to improve the SL program and the educational experience for the students.
ACKNOWLEDGMENTS
We acknowledge Dr Lakshini Sandhya McNamee and my co-supervisor Prof. Thomas Corne Postma, for their supervision, continued support, dedication, and tireless commitment, to this work.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
AUTHOR CONTRIBUTIONS
MGP was involved in conceptualization, data collection, data analysis, and manuscript preparation. PS and BM were involved in the manuscript preparation.
FUNDING SOURCES
This research was funded by MGP through the Research Development Grant (RGD) by DHET from 2016-2019.
REFERENCES
1. Anand BS, Pratap K, Padma TM, Kalyan VS, Vineela P, Varma SC. Assessment of attitude toward community service among dental students of Tertiary Care Teaching Hospital in South India. Indian Journal of Dental Sciences. 2017;9(3):181. [ Links ]
2. Sykes BE, Pendley J, Deacon Z. Transformative learning, tribal membership, and cultural restoration: A case study of an embedded Native American service-learning project at a research university. Gateways: International Journal of Community Research and Engagement. 2017; 10:204-28. [ Links ]
3. Kuh GD. Excerpt from high-impact educational practices:Whattheyare, who has access to them, and why they matter. Association of American Colleges and Universities. 2008;14(3):28-9. [ Links ]
4. Radford D, Holmes,Dunne S, Woolford M. Outreach clinical dental education: the Portsmouth eEperience-a 4-year follow-up study. European Journal of Dental Education. 2016;20(3):148-55. [ Links ]
5. Gibbs B, Wood GC.Reflection for Learning and Practice in Developing Enginners. Excellence in Engineering Education for the 21st Century: The Role of Enginnering Education Research. 2019:118. [ Links ]
6. Zimmerman BJ. Becoming self-regulated learner: An overview. Theory into practice. 2004-41(2):64-70. [ Links ]
7. Victoroff KZ, Hogan S. Students' perceptions of effective learning experiences in dental school: a qualitative study using critical incident technique. Journal of Dental Education. 2006; 70(2): 124-32. [ Links ]
8. Hood JG. Service-learning in dental education: meeting needs and challenges. Journal of Dental Education. 2009;73(4):454-63. [ Links ]
9. Simonet D. Service-learning and academic sucess: The links to retention research. Minnesota Campus Compact. 2008;1(1):1-13. [ Links ]
10. Tumuti DW,Mule LW, Gecaga M, Manguriu DG. Enhancing graduate employability through community engagement: A case study of students' community service at Kenyatta University. Journal of Administrative Sciences and Policy Studies. 2013;1(1):1-14. [ Links ]
11. Volvovsky M, Vodopyanov D, Inglehart MR. Dental students and faculty members' attitudes towards care for underserved patients and community service: do community-based dental education and voluntary service-learning matter? Journal of dental education. 2014;78(8):1127-38. [ Links ]
12. Voogelgesang LJ, Astin AW. Comparing the effects of community service and service-learning. Michigan Journal of Community Service Learning. 2000;7(1). [ Links ]
13. Lalloo R, Evans JL, Johnson NW. Dental students' reflections on clinical placement in a rural and indigenous community in Australia. Journal of dental education. 2013;77(9):1193-201. [ Links ]
14. Postma T, Ayo-Yusuf O, Phalwane M. Piloting the Community Service Attitudes Scale in a South African context with matching qualitative data. South African Dental Journal. 2016;71(10):460-6. [ Links ]
15. Bhayat A, Vergotine G, Yengopal V, Rudolph MJ. The impact of service-learning on two groups of South African dental students. Journal of dental education. 2011;75(11):1482-8. [ Links ]
16. Gaines-Hanks N, Grayman N. International service-learning in South Africa and pens/nal change: An exploratory content analysis. NASPA Journal. 2009;46(1):72-93. [ Links ]
17. Boysen JC, Salsbury SA, Derby D, Lawrence DJ. A focus group study of chiropractic students following international service-learning experiences. Journal of Chiropractic Education. 2016;30(2):124-30. [ Links ]
18. Shiarella AH, McCarthy AM, Tucker ML. Development, and construct validity of scores on the community service attitudes scale. Educational and Psychological Measurement. 2000;60(2):286-300. [ Links ]
19. Braun V Clarke V. Using thematic analysis in psychology. Qualitative research in psTcPology. 2006;3(2):77-101. [ Links ]
20. McNiff J. Action research: Principles and practice: Routledge; 2013. [ Links ]
 Correspondence:
Correspondence:
MG Phalwane
Email: grace.phalwane@smu.ac.za
Author contribution:
MG Phalwane 60%;
B Mthelebofu 20%
P Sodo 20%


{kind=link}