










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.78 no.1 Johannesburg Fev. 2023
REVIEW
Adverse drug reactions, a guide for dentists
N PadayacheeI; D MatesunI; M MatlalaII; R VagiriIII
IDepartment of Pharmacy and pharmacology, University of Witwatersrand, Johannesburg
IISouth African Health product regulatory authority (SAHPRA), Pretoria
IIIDepartment of Pharmacy, University of Limpopo, Limpopo
ABSTRACT
Adverse drug reactions (ADRs) are unintended or harmful effects due to the use of a medicine. Antibiotics and analgesics, which incidentally, are commonly prescribed by dentists, result in most of the ADRs globally. As with most healthcare professionals, dentists do not report on ADRs regularly. Therefore, the aim of the review was to explore the drugs most used in dental practice in South Africa (SA), their associated ADRs and the ADR reporting channels.
The study undertook a literature review that focused on studies of adverse drug reactions specifically in dental practices. An electronic search was done on EBSCO host to source articles published from 2000 to 2022. There was a plethora of ADRs that were found to occur with the medicines that are prescribed by dentists that ranged from minor to serious. Although all medicines have a risk of ADRs, amoxicillin can result in gastrointestinal disturbances and anaphylactic reactions, while clindamycin has a risk of Clostridium difficile infection.
Patients need to be alerted to the risk of a disulfiram reaction with metronidazole and alcohol. Hepatic failure can occur with paracetamol use especially in patients with underlying liver disease, an alcoholic or in an overdose. Ibuprofen, caution in patients with underlying ulcers as gastrointestinal bleeding is a risk. Local anesthetics pose a high threat of severe reactions such as tissue necrosis and direct neurotoxicity while anterograde amnesia, respiratory depression and thrombosis can occur with benzodiazepines.
Dentists can prevent ADRs by having a good knowledge of their prescribed drugs, monitoring their patients and by being judicious in their prescribing habits.
Keywords: Adverse drug reactions, dentists, adverse drug reaction reporting, SAHPRA
INTRODUCTION
Adverse drug reactions (ADRs) are unintended or harmful effects attributed to the use of a drug. Unrecognized ADRs may have significant financial consequences for the patient. Globally, studies show that antibiotics and analgesics are among the leading causes of ADRs and coincidentally are also commonly prescribed by dentists.1,2
Although, most of these reactions are dose-dependent and predictable, reactions like allergic and idiosyncratic reactions can occur and are unrelated to the normal pharmacological action. ADRs may be compounded (aggravated) by drugdrug interactions, drug- food interactions, drug-physiology interactions and underlying comorbidities of the patient.3
Recognizing, managing, and reporting ADRs or any other complications is critical to medication adherence, improving clinical outcomes, and the patients' overall health. The patient's medical history should be evaluated, and the patient counselled on possible adverse effects, before prescribing medications to reduce the risks of ADRs, and increase compliance.7 As in medical practice, underreporting of ADRs among dental professionals is a common phenomenon.4-6 Therefore, this study explores the drugs most commonly used in dental practice in South Africa (SA), their associated ADRs, the importance of ADR reporting, and the ADR reporting channels.
DRUGS USED IN DENTAL PRACTICE
Dentists most commonly use antimicrobials (antibiotics, antifungals, antiviral agents), analgesics (non-steroidal anti-inflammatory drugs (NSAIDs), paracetamol and opioids), local anaesthetics (lidocaine, articaine, lignocaine, mepivacaine), sedatives and general anaesthetics (nitrous oxide, midazolam). Systemic and topical corticosteroids may also be used to manage post-operative inflammation and treat oral immune-mediated diseases.8
ANTIMICROBIALS
Antibiotics
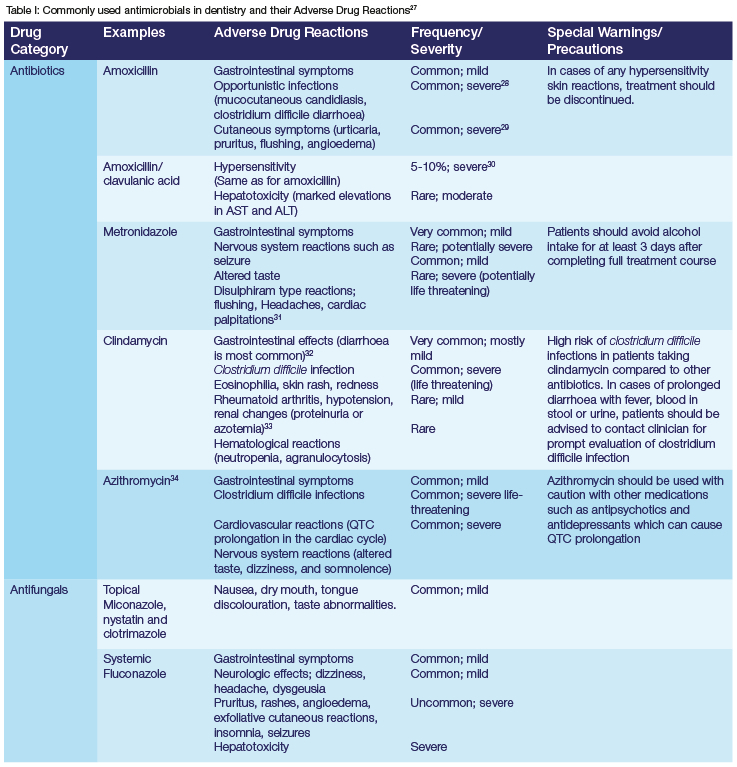
Antibiotics are prescribed for the treatment of bacterial infections, most commonly of pulpal and periodontal origin. However, it may also be used to prevent cardiac and joint complications due to bacteremia in high-risk patients and local complications following surgery.9,10 They are used either empirically based on the anticipated microbiology of odontogenic infections, or based on antimicrobial susceptibility testing.11,12 Short courses of antibiotics (3-7 days) are effective in managing dental infections. In SA, the most prescribed antibiotic in dental practices is amoxicillin.13,14 Azithromycin, a macrolide antibiotic, is not suggested as first-line treatment, but may be considered as an alternative for the patient with suspected or confirmed penicillin allergy.15,16
Amoxicillin, a penicillin-like antibiotic is bactericidal and acts by inhibiting cell wall synthesis in susceptible organisms.17 It is s the first drug of choice in treating odontogenic infections.18,19 A combination of amoxicillin and clavulanic acid, a beta lactamase inhibitor, is also commonly administered due to its lower level of bacterial resistance, extended spectrum of activity and convenient dosing characteristics.20 Amoxicillin is relatively safe in non-allergic patients and has the lowest reported rate of ADRs compared to other antibiotics.19
Metronidazole inhibits nucleic acid synthesis with intracellular macromolecules. It is prescribed as an adjunct to penicillin in severe infections such as severe periodontitis. Additionally, it can be used to treat cases of predominantly anaerobic infections. Metronidazole and alcohol should not be used in combination due to a disulfiram reaction. Metronidazole causes an increase in acetaldehyde because it inhibits the enzyme acetaldehyde dehydrogenase in the ethanol degradation pathway. Patients present with flushing, headache, nausea, and cardiac palpitations and alcohol must be avoided for 3 days after use of metronidazole.17,21
Clindamycin is a lincosamide antibiotic which inhibits protein synthesis by reversibly binding to 50S ribosomal subunits and a good choice for penicillin sensitive patients.22 It is known for its good oral absorption (low incidence of bacterial resistance and high antibiotic concentrations reached in tissues, including bone.23 Nevertheless, there is a greater risk of Clostridium difficile infections reported with clindamycin compared with other antibiotics prescribed in dentistry.24 The anaerobic gram-positive bacteria, Clostridium difficile is transmitted via the fecal-oral route in humans and the usage of ampicillin, amoxicillin, cephalosporins and clindamycin are commonly associated with an increased risk of C. difficile infection. Watery diarrhea, fever, nausea, abdominal pain, nausea, vomiting, weakness, and loss of appetite are common features of C difficile.25,26
ANTIFUNGALS
Oral candidiasis, caused by Candida albicans, is managed topically (using miconazole or nystatin) or systemically with fluconazole and itraconazole. Topical antifungals such as nystatin have few and mild adverse effects because of their limited absorption. However, patient compliance to topical formulations such as nystatin oral suspension may be compromised by unpleasant taste, frequent application, and lengthy use and its prolonged treatment pattern.
In general, the principal risks associated with antibiotics are opportunistic infections, especially oral candidiasis, and gastrointestinal disturbances such as nausea, vomiting and diarrhea, often due to the disruption of the gut flora.27 A summary of the commonly used antimicrobials and their adverse reactions are provided in Table I.
ANALGESICS
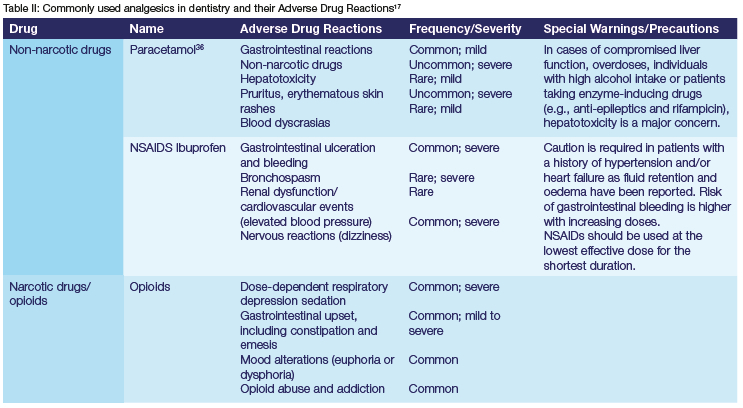
Dentists most commonly prescribe two types of analgesics: non-narcotic analgesics (paracetamol and non-steroidal anti-inflammatory drugs) and narcotic analgesics (opioids). Paracetamol is used for treating mild dental pain when NSAIDs are contraindicated. It is one of the safest analgesics when administered to healthy individuals in usual therapeutic doses.35 However, hepatotoxicity may be a concern due to the buildup of N-acetyl-p-benzoquinone imine, a potentially toxic metabolite, in individuals with compromised liver function (such as alcoholics) or in cases of overdosage.36 The commonly accepted maximum dosage of acetaminophen in a healthy individual is 4 g per day. However, the Food and Drug Administration recommends a maximum dose to 3 g per day to reduce the risk of severe liver injury.37
NSAIDs are the first line of analgesics in treating dental pain, with ibuprofen prescribed most for mild odontogenic pain. It is usually prescribed either alone and in combination with paracetamol.38 Occasionally, maxillofacial surgeons also prescribe etoricoxib and celecoxib, a selective COX-2 inhibitor as short-term treatment for mild to moderate pain associated with dental surgery.39 Due to its selectivity, etoricoxib and celecoxib is usually considered in patients at risk of gastric ulceration or those taking blood thinners such as warfarin.40
Opioids produce analgesia by activation of opioid receptors and are used for managing moderate or severe dental pain. When NSAIDs combined with paracetamol, does not yield sufficient pain relief, a weak opioid analgesic such as tramadol, may be added. However, a short course of a strong opioid, such as oxycodone, may be used in patients suffering from insomnia due to severe pain.41 These patients should be closely monitored due to the high risk of ADR such as constipation. Table II highlights ADR of commonly used analgesics in dentistry.
LOCAL ANAESTHETICS AND THEIR VASOCONSTRICTORS
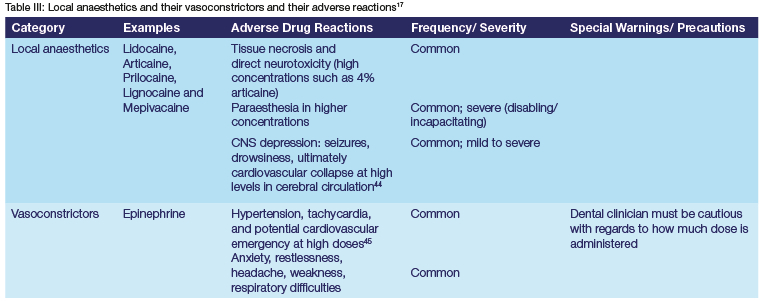
Local anesthesia is commonly used in invasive dental procedures, and include lidocaine, articaine, prilocaine, lignocaine and mepivacaine. These can be applied topically (not all are available as topical preparations) or injected for local infiltration or nerve blocks. Local anaesthetics (LA) are often combined with a vasoconstrictor such as epinephrine, to retain the LA to increase the duration of action, and limit systemic absorption .42
Local anaesthetics are generally considered safe but can cause systemic and local toxicity due to the irritating nature of the solution, pressure from large volumes, or vasoconstriction.43 The dose and concentration should be tailored towards each patient to prevent potential adverse reactions. Table III details the adverse reactions relating to local anaesthetics and their vasoconstrictors.
SEDATIVES AND GENERAL ANAESTHETIC AGENTS
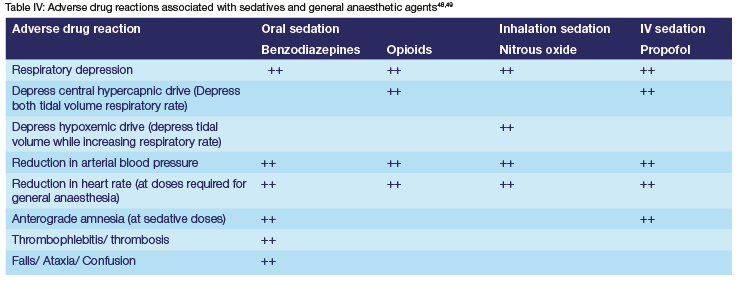
Sedatives and general anaesthetics are classes of drugs which induce sedation, altered consciousness, and reduces anxiety during major dental procedures. They are broadly classified into three categories: oral sedation (diazepam), inhalation sedation (nitrous oxide) and intravenous sedation (propofol, midazolam). Commonly reported ADRs to this class include nausea, vomiting, headache, slurred speech, dry mouth, dizziness, chills, and lockjaw.46 Respiratory depression is a major ADR following the administration of sedatives and general anaesthetic agents47(Table IV). Most adverse reactions to these drugs are dependent on the level of sedation and the number of agents being administered, with more severe effects occurring at high doses and combination therapy.
SYSTEMIC AND ORAL CORTICOSTEROIDS
Both oral and topical corticosteroids have a wide range of uses in dentistry. For example, oral cortisones are used to reduce pulpal inflammation or for post operative inflammation while topical steroids are used for the treatment of lichen planus. However, although useful, corticosteroids pose risks which are dependent on the route of delivery (topical, oral, inhaled, intranasal or intravenous), the length of time that was taken, the type and strength of the cortisone, dosing schedule and systemic other factors. A low dose cortisone is 10mg or less, while a moderate dose is 15-40mg and high dose is over 40mg. Increases in blood sugar and behavioral changes are potential concerns with short-term use of cortisones, while osteoporosis, oral candidiasis, cataracts, glaucoma, arthritis, hypertension, myopathy, Cushing's disease and adrenal suppression can occur after long-term use.50
REPORTING ADRS
As per regulation 40 of the Medicines and Related Substances Act, 1965 (Act 101 of 1965) as amended, a healthcare professional, veterinarian or any other person should inform the South African Health Products Regulatory Authority (SAHPRA), of any suspected ADRs; or any new or existing safety, quality, or effectiveness concerns, occurring because of the use of any medicine or scheduled substance (Medicines Act). Although clinical trials identify ADRs, they are limited due to the number of participants in the trial; the timeframe of the trial as drugs may act differently over a longer period; and also, may exclude high risk individuals such as the elderly or pregnant women. For these reasons, post marketing surveillance is crucial in identifying ADRs and thus informing better prescribing practices which ensures the safety and efficacy of medicines. A spontaneous report, which is a common method of reporting a suspected ADR, is not generated from a controlled study (active surveillance). Spontaneous reports can generate a signal which is 'reported information on a possible causal relationship between an adverse event and a medicine, the relationship being unknown or incompletely documented previously'. More than one ADR report is needed to generate a signal depending on the seriousness.51 For this reason, reporting any ADR is important in identifying signals whereby the necessary course of action can be taken.
The South African adverse drug reaction monitoring system is managed by the regulatory pharmacovigilance unit at SAHPRA. Healthcare professionals including dentists are required to report all suspected adverse reactions to medicines by completing the eReporting link available on the SAHPRA website or completing the Adverse Drug Reaction (ADR)/Product Quality Problem Report form on the SAHPRA website and emailing it to adr@sahpra.org.za.51 Additionally, SAHPRA has launched a MedSafety App, which is a platform whereby both healthcare professionals and the public can report ADRs.
For a report to be considered valid, the following minimum requirements should be included in the report: information about the patient, suspect medicine, suspected reaction, and information about the reporter.
CONCLUSION
Medicines are essential for improving the quality of life of patients, yet they do come with risks. Dentists should consider their patients' comorbidities and current drug use, to select the appropriate drug and dose, which will limit the risk of ADRs. Although dentists have a fair knowledge on ADRs, it is likely that dentists, just like other healthcare professionals, under report these events. To effectively manage the dental patient, dentists need to understand the risks associated with the medicines they prescribe and the importance of reporting ADRs.
REFERENCES
1. Shehab N, Patel PR, Srinivasan A, Budnitz DS. Emergency department visits for antibiotic-associated adverse events. Clin Infect Dis. 2008 Sep 15;47(6):735-43. [ Links ]
2. Howard RL, Avery AJ, Slavenburg S, Royal S, Pipe G, Lucassen P, Pirmohamed M. Which drugs cause preventable admissions to hospital? A systematic review. Br J Clin Pharmacol. 2007 Feb;63(2):136-47. [ Links ]
3. Chavez EM, Jacobsen PL. Pharmacology and aging. Textbook of geriatric dentistry, edited by Poul Holm-Perderson, Angus WG Walls, Jonathan A Ship, 3rd ed, John Wiley and Sons Ltd Publishing. 2015 Jun 19:145. [ Links ]
4. Chari DN, Dave BH, Bargale SS, Deshpande AN, Shah SS, Shah PS. Adverse drug reaction: Knowledge, attitude and practice amongst paediatric dentists in India: An electronic survey. Adv Hum Biol. 2021 May 1;11(2):181. [ Links ]
5. Yip J, Radford DR, Brown D. How do UK dentists deal with adverse drug reaction reporting?. Br Dent J. 2013 Apr;214(8):E22-.E22. [ Links ]
6. Khan SA, Goyal C, Tonpay SD. A study of knowledge, attitudes, and practice of dental doctors about adverse drug reaction reporting in a teaching hospital in India. Perspect Clin Res. 2015 Jul;6(3):144. [ Links ]
7. Schatz S, Weber RJ. Adverse drug reactions. Pharmacy Practice. 2015 Aug 24;1(1). [ Links ]
8. Khammissa RA, Ballyram R, Wood NH, Lemmer J, Feller L. Glucocorticosteroids in the treatment of immune mediated oral diseases: clinical review. S Afr Dent J. 2016 Mar 1;71(2):62-7. [ Links ]
9. Poveda Roda R, Bagán JV, Sanchis Bielsa JM, Carbonell Pastor E. Antibiotic use in dental practice: A review. Med Oral Patol Oral Cir Bucal. 2007 May;12(3):186-92. [ Links ]
10. Almeida VD, Azevedo J, Leal HF, Queiroz AT, da Silva Filho HP, Reis JN. Bacterial diversity and prevalence of antibiotic resistance genes in the oral microbiome. PLOS One. 2020 Sep 29;15(9):e0239664. [ Links ]
11. Siqueira Jr JF, Rôças IN. Microbiology and treatment of acute apical abscesses. Clin Microbiol Rev. 2013 Apr;26(2):255-73. [ Links ]
12. Kuriyama T, Williams DW, Yanagisawa M, Iwahara K, Shimizu C, Nakagawa K, Yamamoto E, Karasawa T. Antimicrobial susceptibility of 800 anaerobic isolates from patients with dentoalveolar infection to 13 oral antibiotics. Oral Microbiol Immunol. 2007 Aug;22(4):285-8. [ Links ]
13. Mthethwa SR, Matjila SA. Antibiotic prescribing practices of dentists at Medunsa Oral Health Centre. South African Dental Journal. 2018 Sep;73(8):520-6. [ Links ]
14. Lalloo R, Solanki G, Ramphoma K, Myburgh NG. Endodontic treatment-related antibiotic prescribing patterns of South African oral health professionals. International endodontic journal. 2017 Nov;50(11):1027-33 [ Links ]
15. Singh VP, Nayak SU, Nettemu SK, Nettem S, Lee YH, Verma MB. Azithromycin in periodontal therapy: beyond the antibiotics. J Periodontol Oral Implant. 2018 Dec 31;2(2):61-6. [ Links ]
16. Buset SL, Zitzmann NU, Weiger R, Walter C. Non-surgical periodontal therapy supplemented with systemically administered azithromycin: a systematic review of RCTs. Clin Oral Investig. 2015 Nov;19(8):1763-75. [ Links ]
17. Rossiter, Dawn. South African Medicines Formulary. Ed. Dawn Rossiter. 13th ed. Rondebosch, South Africa: Health and Medical Pub. Group of the South African Medical Association, 2016. Print. [ Links ]
18. Akhavan BJ, Khanna NR, Vijhani P. Amoxicillin. InStatPearls [Internet] 2021 Aug 17. StatPearls Publishing. [ Links ]
19. Thornhill MH, Dayer MJ, Durkin MJ, Lockhart PB, Baddour LM. Oral antibiotic prescribing by NHS dentists in England 2010-2017. Br Dent J. 2019 Dec;227(12):1044-50. [ Links ]
20. Robertson D, Smith AJ. The microbiology of the acute dental abscess. J Med Microbiol. 2009 Feb 1;58(2):155-62. [ Links ]
21. Dabija-Wolter G, Al-Zubaydi SS, Mohammed MM, Bakken V, Bolstad AI. The effect of metronidazole plus amoxicillin or metronidazole plus penicillin V on periodontal pathogens in an in vitro biofilm model. Clin Exp Dent Res. 2018 Feb;4(1):6-12. [ Links ]
22. Dar-Odeh NS, Abu-Hammad OA, Al-Omiri MK, Khraisat AS, Shehabi AA. Antibiotic prescribing practices by dentists: a review. Ther Clin Risk Manag. 2010;6:301. [ Links ]
23. Leffler DA, Lamont JT. Clostridium difficile infection. New England Journal of Medicine. 2015 Apr 16;372(16):1539-48. [ Links ]
24. Czepiel J, Drózdz M, Pituch H, Kuijper EJ, Perucki W, Mielimonka A, Goldman S, Wultanska D, Garlicki A, Biesiada G. Clostridium difficile infection. European Journal of Clinical Microbiology & Infectious Diseases. 2019 Jul;38(7):1211-21. [ Links ]
25. Kirkwood KL. Update on antibiotics used to treat orofacial infections. The Alpha omegan. 2003 Dec 1;96(4):28-34. [ Links ]
26. Vardakas KZ, Trigkidis KK, Boukouvala E, Falagas ME. Clostridium difficile infection following systemic antibiotic administration in randomised controlled trials: a systematic review and meta-analysis. Int J Antimicrob Agents. 2016 Jul 1;48(1):1-0. [ Links ]
27. Mohsen S, Dickinson JA, Somayaji R. Update on the adverse effects of antimicrobial therapies in community practice. Can Fam Physician. 2020 Sep 1;66(9):651-9. [ Links ]
28. Blondeau JM. What have we learned about antimicrobial use and the risks for Clostridium difficile-associated diarrhoea? J Antimicrob Chemother. 2009 Feb 1;63(2):238-42. [ Links ]
29. Shenoy ES, Macy E, Rowe T, Blumenthal KG. Evaluation and management of penicillin allergy: a review. Jama. 2019 Jan 15;321(2):188-99. [ Links ]
30. Mirakian R, Leech SC, Krishna MT, Richter AG, Huber PA, Farooque S, Khan N, Pirmohamed M, Clark AT, Nasser SM. Management of allergy to penicillins and other beta-lactams. Clin. Exp. Allergy. 2015 Feb;45(2):300-27. [ Links ]
31. Karamanakos PN, Pappas P, Boumba VA, Thomas C, Malamas M, Vougiouklakis T, Marselos M. Pharmaceutical agents known to produce disulfiram-like reaction: effects on hepatic ethanol metabolism and brain monoamines. Int J Toxicol. 2007 Sep;26(5):423-32. [ Links ]
32. Murphy PB, Bistas KG, Le JK. Clindamycin. In StatPearls [Internet] 2018. StatPearls Publishing. [ Links ]
33. Luchian I, Goriuc A, Martu MA, Covasa M. Clindamycin as an alternative option in optimizing periodontal therapy. Antibiotics. 2021 Jul 4;10(7):814. [ Links ]
34. Hansen MP Scott AM, McCullough A, Thorning S, Aronson JK, Beller EM, Glasziou PP, Hoffmann TC, Clark J, Del Mar CB. Adverse events in people taking macrolide antibiotics versus placebo for any indication. Cochrane Database Syst Rev. 2019(1). [ Links ]
35. Roberts E, Nunes VD, Buckner S, Latchem S, Constanti M, Miller P, Doherty M, Zhang W, Birrell F, Porcheret M, Dziedzic K. Paracetamol: not as safe as we thought? A systematic literature review of observational studies. Ann Rheum Dis. 2016 Mar 1;75(3):552-9. [ Links ]
36. Turkoski BB. Acetaminophen: old friend-new rules. Orthop Nurs. 2010 Jan 1;29(1):41-3. [ Links ]
37. Food and Drug Administration. FDA Acetaminophen Dosage Announcement. Available from: chrome extension://efaidnbmnnnibpcajpcglclefindmkaj/ https://www.medicaid.nv.gov/Downloads/provider/web_announcement_468_20120425.pdf. (2012, Accessed 5 August, 2022). [ Links ]
38. Ong CK, Seymour RA, Lirk P, Merry AF. Combining paracetamol (acetaminophen) with nonsteroidal antiinflammatory drugs: a qualitative systematic review of analgesic efficacy for acute postoperative pain. Anesth Analg. 2010 Apr 1;110(4):1170-9. [ Links ]
39. Malmstrom K, Sapre A, Couglin H, Agrawal NG, Mazenko RS, Fricke Jr JR. Etoricoxib in acute pain associated with dental surgery: a randomized, double-blind, placebo-and active comparator-controlled dose-ranging study. Clin Ther. 2004 May 1;26(5):667-79. [ Links ]
40. Hunt RH, Harper S, Callegari P, Yu C, Quan H, Evans J, James C, Bowen B, Rashid F. Complementary studies of the gastrointestinal safety of the cyclo-oxygenase-2-selective inhibitor etoricoxib. Aliment Pharmacol Ther. 2003 Jan;17(2):201-10. [ Links ]
41. Krasniqi S, Daci A. Analgesics use in dentistry. Pharmacology, Toxicology and Pharmaceutical Science-Pain Relief-From Analgesics to Alternative Therapies. 2017 May 24:111-39. [ Links ]
42. Balakrishnan R, Ebenezer V. Contraindications of vasoconstrictors in dentistry. Biomed Pharmacol J. 2013 Dec;6(2):409-14. [ Links ]
43. Becker DE, Reed KL. Essentials of local anesthetic pharmacology. Anesth Prog. 2006;53(3):98-109. [ Links ]
44. Dillane D, Finucane BT. Local anesthetic systemic toxicity. Can J Anesth. 2010 Apr;57(4):368-80. [ Links ]
45. Dalal R, Grujic D. Epinephrine. InStatPearls [Internet] 2022 May 8. StatPearls Publishing. [ Links ]
46. Bounds CG, Nelson VL. Benzodiazepines. In StatPearls [Internet]. 2020. StatPearls Publishing. [ Links ]
47. Laporta ML, Sprung J, Weingarten TN. Respiratory depression in the post-anesthesia care unit: Mayo Clinic experience. Bosn J Basic Med Sci. 2021 Apr;21(2):221. [ Links ]
48. Veselis RA, Reinsel RA, Feshchenko VA. Drug-induced amnesia is a separate phenomenon from sedation: electrophysiologic evidence. Anesthesiology. 2001 Oct 1;95(4):896-907. [ Links ]
49. Stachnik J. Inhaled anesthetic agents. Am J Health Syst Pharm. 2006 Apr 1;63(7):623-34. [ Links ]
50. Glassick A, Hamilton T, Shetty K. Management of Dental Patients on Steroid Therapy and Steroid Therapy for Patients in a Dental Practice. New Year, New Changes. 2010 Jan 1:27. [ Links ]
51. South African Health Products Regulatory Authority. Post-marketing reporting of adverse drug reactions to human medicines in South Africa. Available from: www.sahpra.org.za/wpcontent/uploads/2020/03/2.33_ADR_Reporting_Post_MarketingJan2020v6_31Jan2020.pdf.(2020,Accessed 25 June 2022). [ Links ]
 Correspondence:
Correspondence:
N Padayachee
Neelaveni.padayachee@wits.ac.za
Orcid details
Padayachee https://orcid.org/0000-0002-6146-8702
Deborah Matesun https://orcid.org/0000-0002-9869-9926
Mafora Matala https://orcid.org/0000-0003-2071-3211
Rajesh Vagiri https://orcid.org/0000-0003-0564-7594.
Author contributions
Neelaveni Padayachee conceptualised and drafted the idea for the paper. She contributed to researching and writing part the sections on the policy of the paper. She also edited and reviewed the paper for language and content
Deborah Matesun researched and wrote about the drugs involved in dental practice and assisted with the referencing of the article
Mafora Matlala assisted with the language editing and content review for the paper
Rajesh vagiri assisted with language editing, researching and writing the introduction and conclusion for the paper


{kind=link}
{kind=link}
{kind=link}
{kind=link}