










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.77 n.10 Johannesburg Nov. 2022
http://dx.doi.org/10.17159/2519-0105/2022/v77no10a4
RESEARCH
Evaluating the oral health knowledge, attitude and practice among undergraduate students and staff at selected federal University in Imo state, Nigeria
SC OnwubuI; KC OgwoII; UP OnyenuIII; GC IwuekeIV; TH MokhothuV
IChemistry, Durban University of Technology (DUT), Durban, South Africa. ORCID: 0000-0002-4499-1534
IIDental Technology, Federal University of Technology (FUTO), Owerri, Imo State, Nigeria
IIIDental Technology, Federal University of Technology (FUTO), Owerri, Imo State, Nigeria
IVDental Technology, Federal University of Technology (FUTO), Owerri, Imo State, Nigeria
VChemistry, Durban University of Technology (DUT), Durban, South Africa
ABSTRACT
BACKGROUND: Oral health is an essential component of an individual's general health and overall well-being. Although past studies have evaluated oral health knowledge, attitude and practices (KAP), little is known about the level of KAP between students and staff of higher education institutions. This study aimed to evaluate oral health knowledge, attitudes, and practices among undergraduate students and staff at a selected University of Technology in Nigeria.
METHODS: A multicentre cross-sectional survey was conducted between May - June 2021 with a sample of 747 consisting of 378 students and 369 staff, recruited from 8 faculties across the University. One-way ANOVA test was applied for the statistical evaluation of numerical measures. The association between knowledge, attitudes and practice scores were assessed using Pearson correlation analyses (α=.0.05).
RESULTS: No significant differences were found in the oral health knowledge, attitude, and practices between the students and staff (P>0.05). Overall, the finding suggests that 84.3% of the respondents had a positive attitude toward oral health, 92.5% had high knowledge and 87.4% practised oral health was adequate. The respondents KAP differed by socio-demographic characteristics. The relationship between knowledge and practice was fair (r = 0.358, p < 0.01) while positive weak correlations were observed between attitude and practice (r = 0.198, p < 0.01), and between knowledge and attitude (r = 0.173, p < 0.01),
CONCLUSION: The salient feature of this study suggests that while there was a high level of knowledge among the respondents, the attitude and actual practice of oral healthcare does not commensurate with the level of knowledge. Nonetheless, it was found that knowledge had positive associations with the practice of oral health care. The findings suggest there is a need to improve the knowledge about oral health practice among both staff and students through a tailored design of community-based awareness to increase oral health practice,
Keywords: Attitude, Knowledge, practice, oral health, university
INTRODUCTION
Oral health is an essential component of an individual's general health and overall well-being, which is related to an individual's oral health knowledge and healthy oral hygiene habits 1. Abstract knowledge of oral health practices alone does not ensure the subsequent change in an individual's attitudes and behaviours -as they are usually acquired after conceptualizing oral health practices 2. Neglect of oral health, on the other hand, can lead to pain and suffering, which can affect an individual's quality of life and hinder productivity in the workplace3,4. According to the World Health Organization (WHO), oral health problems are still not well controlled globally despite the considerable improvements in oral health measures among populations 5. In Africa, for example, it is estimated that more than 480 million people suffer from oral diseases such as dental caries and periodontal, and tooth loss despite most of these diseases being preventable6. This state of oral health might be related to the rapid development of oral diseases following lifestyle changes such as consumption of a sugar-rich diet, lack of water fluoridation, and other socio-environmental factors7, 8.
The high incidence and prevalence of oral diseases globally qualify oral health as a serious public health issue. For instance, the cost of treating oral diseases imposes large economic burdens on families and healthcare systems, with particular concern over their rising prevalence in many low, middle-income countries (LMICs) associated with wider economic, social, and commercial changes4. Moreover, it is noted in the literature that the current westernised model of modern dentistry (high technology and treatment-focused) is unaffordable and inappropriate in many LMICs 49. Hence a radically different approach is essential to address the global challenge of oral diseases.
In 2003, the Fédération Dentaire Internationale World Dental Federation (FDI), WHO, and the International Association for Dental Research issued the document "Global Goals for Oral Health 2020" which contains proposals for new goals, objectives, and targets for the global oral health of increasing detail and complexity. The aforementioned proposal aimed to provide an instrument for local and national health care planners to determine realistic goals and standards for oral health7. Part of this requires a shift in dentistry from a treatment-oriented approach to more preventive oral healthcare10. As such, establishing a baseline of detailed information regarding oral health knowledge and healthy oral hygiene habits will help policymakers set attainable goals and track changes. Moreover, this baseline information will help strengthen oral health programs through the implementation of effective prevention measures.
Studies on oral health knowledge, attitudes, and practices have been conducted among university students in different countries. In 2014, Peltzer and Pengpid investigated oral health behaviour and associated factors among undergraduate university students from various disciplines in 26 low, middle-, and high-income countries. This study confirmed low rates of tooth brushing and dental attendance among university students in different cultures across Africa, Asia, and the Americans11. In Nigeria, a study was conducted to compare oral health knowledge, attitudes, and behaviour of medical, pharmacy, and nursing university students. The investigators found that students' oral health knowledge, attitudes, and behaviour were inadequate and needed to be improved12. In 2017, Kumar and colleagues. studied and compared oral health knowledge, attitudes, and practices among dental and medical students at a university in Eastern India. They reported that oral health knowledge and practices among females were better than that of males13. In Arab countries, several studies have been conducted to assess oral health knowledge, attitudes, and behaviours, especially among school students14. Another study assessed university dental undergraduate students and compared them with undergraduate students of other faculties15. The findings of these studies are expected, as, compared with non-dental students, dental students had already received education on oral health in their undergraduate curriculum.
The above-mentioned studies mainly focused on undergraduate students' oral health knowledge, attitude and practices, but the staff who shoulder the responsibilities of educating and building these students are not considered. The study, to the best of our knowledge, represents the first study of its kind that explored and evaluate oral health knowledge, attitude and practices among both staff and students of higher education institutions.
Moreover, in the Federal University of Technology Owerri, (FUTO), Nigeria, there is not any survey conducted or published that assessed and or compared the knowledge, attitude and practices of oral health care among staff and students. Therefore, the present study aimed to evaluate oral health knowledge, attitudes, and practices among undergraduate students and staff at the Federal University of Technology Owerri (FUTO).
Given these, the present study addresses the following objectives:
1. To assesses the level of oral knowledge, attitude and practice of undergraduate students and staff in a selected Federal University of Technology in Nigeria
2. To determine the association between the socio-demographic characteristics and the oral health knowledge, attitude and practice of undergraduates and staff.
RESEARCH METHODOLOGY
2.1 Research design
A quantitative multicentre cross-sectional design was undertaken to collect data from randomly selected undergraduate students and staff of the University of Technology Owerri, Imo State, Nigeria through the administration of a close-ended questionnaire. The main aim was to assess the level of oral health knowledge, attitude and practices among students and staff.
2.2 Study setting
The study was conducted among undergraduate students and staff of the Federal University of Technology (FUTO). FUTO is a top-ranking University of technology in Nigeria and indeed the nation's pride. Established in 1981, the university has grown tremendously, stretching its academic disciplines and research across eight different schools and over fifty academic departments. FUTO is located 25 kilometres South of Owerri, Imo state. FUTO has over 22000 undergraduate students and a 10000 staff population which are distributed across the eight (8) running faculties namely; School of Engineering and Engineering Technology (SEET), School of Agriculture and Agricultural Technology (SAAT), School of Health Technology (SOHT), School of Physical Sciences (SOPS), School of Environmental Sciences (SOES), School of Biological Sciences (SOBS), School of Management Technology (SMAT), School of Information and Communication Technology (SICT).
2.3 Sampling technique and sample size
The sample size for this study was determined using the Raosoft sample size calculator with a 95% confidence level, 5% margin of error, 50% response distribution and a population size of 22000 for students and 10000 for staff. The sample size of 377 for students and 370 for staff was used in this study. The total number of students and staff from the various faculties included 747 with 378 from SEET, 141 from SAAT, 25 from SOHT, 80 from SOES, 97 from SOPS, 68 from SOBS, and 44 from SMAT.
All undergraduate students were considered for the study from 18 years and above. For the staff, both academic and non-academic staff (administrative and technical staff) which were divided into the status of junior personnel (JP) and senior personnel (SP) were included in the study. Students in 100level (First-year students) were excluded from the study as it is believed that most of them would be below 18 years and would have to seek the consent of their guardian before participating.
Fourth-year students (400 levels) were also excluded as they were not in school at the time this study was conducted and also postgraduate students. Students who are 18 years and above in their second, third, and fifth year of study, and registered at the time of data collection were included in the study. A multicenter study was carried out this stud which entails using stratified sampling techniques in the selection of study participants. Each of the respondents was stratified into three groups, namely students academic staff and non-academic staff. On each day of the data collection, students and staff were randomly selected to fill out the questionnaires from across the eight (8) faculties.
The first 10 students we saw in each classroom entered were approached to fill the questionnaires and for staff, the first 5 seen in each staff room or office across the school were given the questionnaire to fill. This pattern was followed on each data collection day until the sample size was realized. On each data collection day, we did not visit the faculty visited the previous day. This was done so that the data gotten will be evenly distributed. Data collection took us two weeks from May to June 2021 to collect excluding Friday because of the low turnout of students and staff in school.
2.4 Instrument for data collection
A standardized pretested closed-ended questionnaire based on WHO Oral Health Surveys Basic Methods 5th Edition designed in the English language, for children 16 was adapted with few modifications made so as make the questions ideal for the targeted population. It comprises 31 questions which include 11 oral health knowledge questions, 9 Attitude questions and 11 oral hygiene practices questions with the first section containing the socio-demographic questions. The questions were asked to obtain information regarding the socio-demographic background of the participants.
2.5 Data analysis
The Data was presented on Microsoft Excel 2007 spreadsheet and subsequently entered into Statistical Package for Social Sciences spreadsheet (SPSS version 27.0, IBM Statistics, New York, USA) for analysis. For the items included in the knowledge and attitude sections of the questionnaire, each correct answer was scored "one" and wrong and do not know answers were scored "zero." In the practice section, "zero" and "one" scores were given according to the appropriateness of the option selected by the respondent. The individual scores were summed up to yield a total score. Respondents were divided into Good and Poor Knowledge groups in the study results. Participants who scored 0.5 or more on the total questions were categorized as belonging to the good knowledge group and those with a score of 0.4 and below were considered to be in the poor knowledge group.
The same measure was used for attitude and practice scores. Subjects for attitude were categorized into two groups also namely; Negative Attitude and Positive Attitude while for practice, Adequate and Inadequate Practice. Descriptive statistics were obtained, and mean percentage scores, standard deviation, and frequency distribution were calculated for the oral health knowledge, attitude, and practices item. The Student's T-test and ANOVA test was applied for the statistical evaluation of numerical measures. The association between knowledge, attitudes and practice scores were assessed using Pearson correlation analyses.
2.6 Validity and reliability of the instrument
All instruments of the study were critically reviewed by an oral health care expert. In addition, the adapted questionnaire (WHO, 2013), further expresses the validity of the instrument used. Prior to data collection, the study was piloted and pretested with selected students who did not form part of the main study.
2.7 Ethical consideration
Ethical approval for this research work that related to or deals with human subjects was requested and granted by the School of Health Technology Ethical Review Committee before data was collected (FUT/ SOHT/2021/REC-DNT/1).
RESULTS
3.1 Socio-demographic characteristics
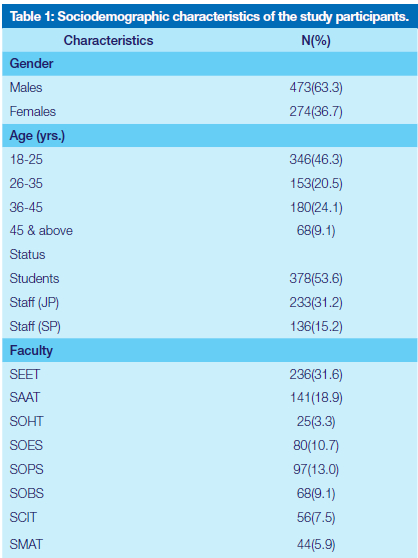
The socio-demographic characteristics of the respondents are given in Table 1. The data show that majority of the respondents were males (63.3%), aged 16 - 25years (46.3%) mainly dominated by students (53.6%), and were from SEET (31.6%).
3.2 Respondents' knowledge of Oral Health
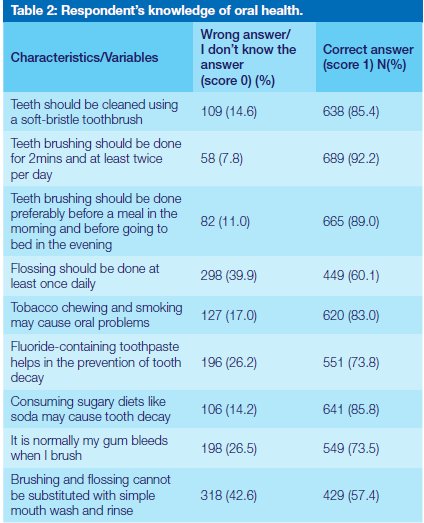
Table 2 depicts the knowledge among the respondents about oral health. The majority (85.4%) knew that teeth should be cleaned using a soft-bristle toothbrush, also 90.2% knew that tooth brushing should be done for 2mins at least twice per day. Teeth brushing should be done preferably before a meal in the evening, 89% knew that and 60.1% knew flossing should be done at least once daily. 83% knows that tobacco chewing and smoking may cause oral problems and 73.8% knew that using fluoride-containing toothpaste helps in the prevention of tooth decay. Consuming sugary diets like soda may cause tooth decay, 85.8% knew this. 73.5% knew it isn't normal for their gum to bleed when brushing. Brushing and flossing cannot be substituted with simple mouthwash and rinse, only 57.4% knew this.
3.2.1 Distribution of Knowledge
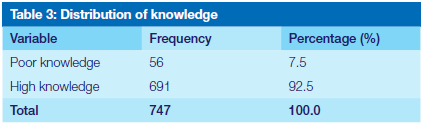
The distribution table for knowledge indicates a high knowledge rate of 92.5% among the respondents (Table 3).
3.3 Respondents' Attitude towards Oral Health
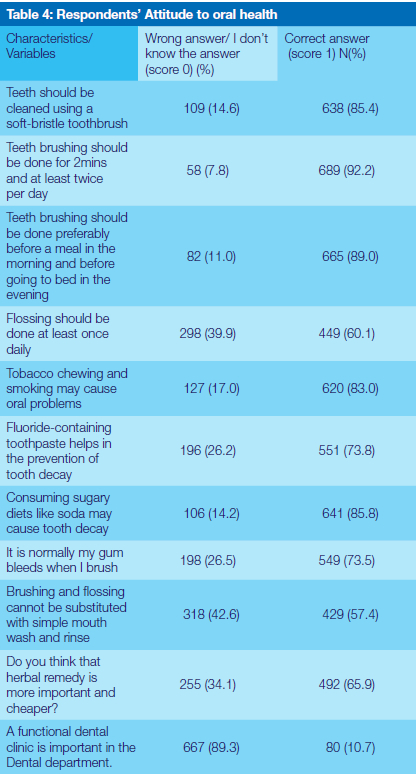
Table 4 shows the oral health attitude of the participants. The majority (88.9%) believe that dental problem can affect general health, participants perceived that regular visit to the dentist is necessary (69.9%), 49.4% thinks it's a big loss to their health to remove a tooth, immediate replacement of missing natural teeth by artificial teeth is necessary (37.2%), 83.9% believes chewing tobacco/ smoking is a bad habit and that dentist care only about treatment and not prevention (73.4%). Do you think that the treatment of toothache is important as any other part of the body? (90.4%) supports that assertion and 73% are afraid of going to the dentist because they think is expensive (81.5%). The herbal remedy is more important and cheaper (34.1%). Having a functional dental clinic is important in the dental department (89.3%).
3.3.1 Distribution of Attitude
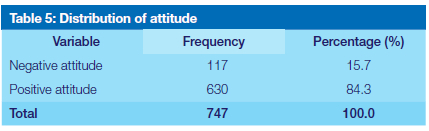
Table 5 shows the distribution of attitude and it indicates that a good number of the respondents have a positive attitude towards their oral health (84.3%).
3.4 Respondents' Practice of Oral Health
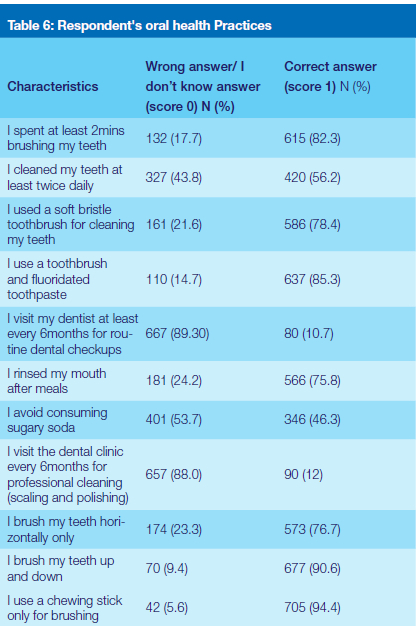
Table 6 depicts the respondents' oral health practices. The table shows that the majority (82.3%) spend at least 2 minutes brushing their teeth, 56.2% brush twice daily and 78.4% used soft bristle toothbrushes for cleaning their teeth. Also, the table shows that the majority of the participants (85.3%) use toothbrushes and fluoridated toothpaste and only 10.7% visit the dentist for at least 6 months for routine dental checkups. Most (75.8%) rinse their mouth after meals and only 46.3% avoid consuming sugary soda. Only 12% go for scaling and polishing every 6 months and the majority brush their teeth horizontally only, 90.6% brush their teeth up and down and a great number (94.4%) of the participants do not use only chewing sticks for brushing.
3.4.1 Distribution of Oral Health Practice
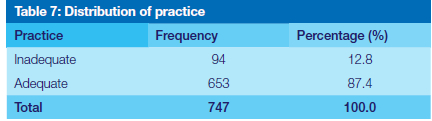
The data in Table 7 shows the distribution of the respondents' oral health practices. The oral health practice was found to be adequate (87.4%).
3.5 Association between socio-demographic characteristics and mean kap scores
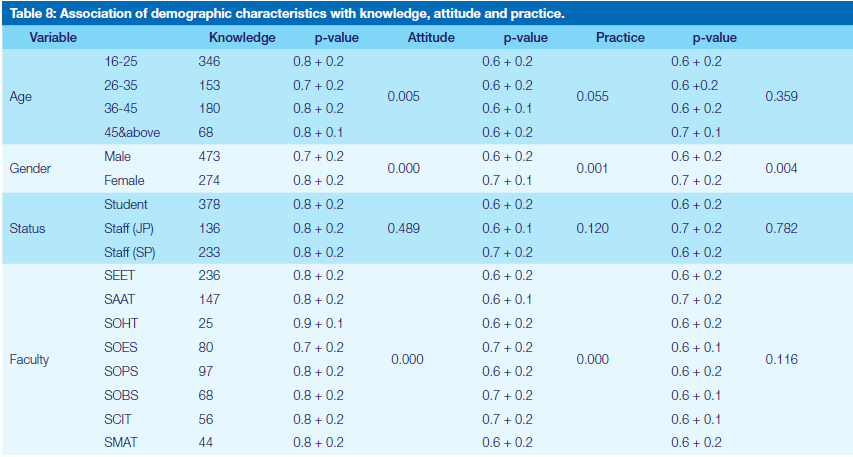
The association between the respondents' socio-demographic characteristics and the mean KAP score is presented in Table 8. The ANOVA value measured for the age indicates that there is a statistically significant difference among the respondents in terms of their knowledge of oral health (P=0.005). No difference was however found between the respondents' gender and their attitude and practice of oral health (P>0.05).
The ANOVA value measured for the gender indicates that there is a statistically significant difference among the respondents in terms of their knowledge of oral health (p<0.005), attitude (p=0.001), and practice (P=0.004). The mean value measured suggests that the female respondents have higher knowledge (M=0.8±0.2), attitude (M=0.7±0.1), and practice (M=0.7±0.2) of oral health when compared to the males.
In terms of status, the ANOVA value measured indicates that there was no significant difference in the respondents' knowledge, attitude, and practice of oral health (P>0.05). In terms of the faculty of the respondents, the ANOVA value indicates that there is a statistically significant in the respondents' knowledge (p<0.001) and attitude (p<0.001), but no difference was found for their practice (P>0.05). The mean value measured suggests that the SOHT respondents have higher knowledge (M=0.9±0.1) while those from SOES (0.7±0.1), SOBS (0.7±0.1), and SCIT (0.7±0.1) have a more positive attitude towards oral health.
3.6 Correlation between knowledge, attitude and practices
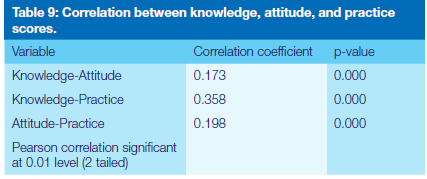
Correlation were interpreted using the following criteria 0 - 0.25 = weak correlation, 0.25 - 0.5 = fair correlation, 0.5 - 0.75 = good correlation, and greater than 0.75 = excellent correlation (Cohen, 1988). The data in Table 9 revealed a weak association between knowledge -attitude (r = 0.173, p < 0.0001), and attitude - practice (r = 0.198, p < 0.0001). For knowledge - practice (r = 0.358, P < 0.0001) there was a fair positive linear correlation. This suggests that a good knowledge of oral health positively associates with the appropriate practice of oral health care.
DISCUSSION
Many KAP surveys concerning oral health have earlier been conducted in the University of Port Harcourt, River State Nigeria but concentrated on medical, pharmacy and Nursing students 12 and overseas 17-19. In developing countries, there is a high prevalence of oral disease in their communities 20. This can be due to neglect, scarcity of resources, poor knowledge and negative attitudes. This multicenter cross-sectional study assesses the knowledge, attitude and practices of (747) students and staff who were randomly selected from the right (8) faculties in FUTO.
The finding of this study suggests that the majority of the respondents knew the use, frequency and time of using a toothbrush, as a tooth-cleaning aid. This was higher than most studies reported in India and globally17, 21. More than half of the respondents were aware of the role of fluoride in preventing dental decay in contrast to only 29.6%, in a study on Saudi students in 201514. The knowledge of the surveyed candidates in regards to the use of dental floss in preventing dental decay was 55.2%, which was somewhat lower than compared of Iranian students, which was 78.8%, in a study in 2015 22. The finding suggests that the majority (83%) of the respondents knew that tobacco chewing and smoking may cause oral problems. This is important given that a good knowledge of oral health is necessary to pursue healthy oral practices 23, 24. Moreover, the respondents' knowledge of oral health measured in this study (92.5%) was higher when compared to the 55.7% reported at Qassim University, Saudi Arabia25. Possible reasons that can be attributed to this difference in response are a demographic variation of the study population, study location and as well as the study tool used for data collection. The results notwithstanding, it is important that the population should be educated on all aspects of oral health rather than on a single or few issues.
The attitude among the participants regarding oral health was diverse. In a study done by Jaber, Khan25 among male students at Qassim University Saudi Arabia, the results showed that students perceived that regular visits to the dentist were necessary (81.5%). This was per a similar study by 26. However, in our study, our data is slightly lower (69.9%). This may be attributed to poor favourable conditions like no university dental clinic, no dental clinic at the primary health centre, negative impression about dentists, their supposed belief that dental care is expensive or that the only government-owned hospital with a dental clinic is far from the campus.
Equally concerning, although 69.9% of the surveyed participants stated that regular dental visit was necessary, only 12% of them, however, practice it. This shows that the awareness of oral health doesn't necessarily influence good dental practice. It was also uncovered that the majority of the respondents (73%) are afraid of visiting the dentist. This perhaps could be because of their phobia of needles or pain felt during extraction of tooth/teeth or they are supposed to believe in the cost of Dental care. This is concerning as fear of the dentist can have serious repercussions on an individual's oral health and therefore constitute a barrier to dental visits 27.
In literature, it is evident that the easiest oral care is to practice daily brushing and flossing - as this help reduce the incidence of dental diseases 24. In this study, it was found only 56.2% at least clean their teeth twice daily. Nonetheless, our findings are slightly higher than the 52.6% reported by Jaber, Khan 25 but still lower than the 65% reported by Kassak, Dagher 28. This is concerning and suggests that not everyone adheres to the golden rule of cleaning the teeth at least twice daily. The majority brushed with a toothbrush and fluoridated toothpaste (85.3%) which is similar to those reported by Jaber, Khan 25. The high use of fluoridated toothpaste may be related to the fact that it is a common and important ingredient found in toothpaste 29. Besides, fluoride used helps in decreasing caries risk and is effective in aiding enamel remineralisation 30, and thus could be beneficial in maintaining good oral health.
Part of the study objective was to determine the association between the respondents' socio-demographic characteristics and the oral health knowledge, attitude and practice of oral healthcare. There was no statistical significance in their status, meaning no difference was noticed in the KAP scores of both students and staff. It was, however, found that the gender and faculty of the respondents differ significantly in their mean KAP scores (Table 8). The female respondents, for example, had better knowledge, attitude toward oral health and better oral care practice than males. This is similar to most studies that have shown females consistently achieving better scores in the KAP survey regarding oral health 28, 31, and could be attributed to the fact that the females are more concerned about body and facial image. Consequently, they would seek regular dental care and take more care of their oral health to maintain a good appearance 31.
With reference to the respondents' faculty, SOHT scored highest in the knowledge and attitude section with a statistically significant difference (Table 8). This is the same with the study in Saudi Arabia done among university students by Al Subait, Alousaimi 14. This indicates a high level of awareness among the school of health respondents. It could be expected that respondents in the health discipline are conscious of general health including dental health which could have informed their knowledge.
Moreover, the study found that better knowledge can lead to positive oral health practices. This will help in the prevention and management of oral diseases. There are certain advantages to the study. Targeting youths seem to be most appropriate for procuring information about the oral health status of a place as they disclose information about what is being taught/learnt from the school, parents and surroundings regarding oral health and what kind of attitude and habits have been groomed or are grooming which will eventually be carried in the next generation in the particular area 18.
4.1 Limitations and directions for future studies
We acknowledge that the data collection method may have certain limitations. Bias could be introduced as the participants tend to give socially desirable responses like overestimating the frequency of tooth brushing and underestimating negative behaviour such as consumption of sugar and tobacco. This was minimized by piloting and pretesting the questionnaire to help establish the practicality and its applicability. The survey was focused mainly on obtaining the level of knowledge, attitude and practice in relation to the oral health of students and staff in FUTO. Further studies should be done to examine the perception of university students regarding the link between oral health hygiene and susceptibility to diseases such as oral cancer, periodontal disease, and caries. To more accurately measure participants' knowledge of good oral health practices, questions identifying the consumption of alcohol, energy drinks and soft drinks should be included in the survey.
4.2 Recommendations
As a result of the findings and conclusion reached the researchers proposed the following recommendations:
1. Health practitioners need to change the public perception of oral health. Many people do not consider oral health important to their overall health and fail to understand the role it plays in preventing future diseases. If health practitioners effectively communicate the importance of oral health and its impact on the body, it will encourage people to visit the dentist and thus prevent future diseases. It behoves health care professionals to encourage people to maintain good oral health practices by brushing and flossing their teeth daily, as well as visiting a dentist for an annual check-up. It is vital to establish a line of communication between dentists and medical doctors to ensure an individual's oral and physical health is concomitantly examined to minimize the onset of future health problems.
2. Introducing good oral health practices to young adults early in their educational career can promote overall health, particularly as they age. To accomplish this, it is necessary to integrate good oral health education into the health curriculum developed for secondary school and university students. Optimally it is best to begin teaching oral health practices to children as early as preschool age. At this young age, parents need to be actively involved in teaching their young children about the necessity to brush and floss their teeth regularly. For this study, given the diverse population of the university, it is essential to direct educational efforts toward members of underrepresented and economically insecure populations to ensure they understand the importance of visiting a dentist on an annual basis.
CONCLUSIONS
From the study conducted an overwhelming majority of the survey respondents had good knowledge, positive attitude and adequate practice with respect to oral health. Nevertheless, it was observed from the attitude section that not all of the respondents believe that regular visit to the dentist is important. These moderate statistics show that there is an underlying problem. Moreover, many respondents believe that dental treatment is expensive thereby making them depend on other remedies like the use of herbal treatment. Overall, the study demonstrates that good knowledge of oral health positively stimulates appropriate practices of oral health. As such, there is a need to improve the knowledge about oral health practice among both staff and students through a tailored design of community-based awareness to increase oral health practice.
Acknowledgement
The authors acknowledge the financial support from the National Research Foundation of South Africa (Grant Numbers: 129492)
Declaration
No conflict of interest declared
REFERENCES
1. Sabbah W, Tsakos G, Chandola T, et al. Social gradients in oral and general health. J Dent Res 2007; 86: 992-996. [ Links ]
2. Farsi NJ, Merdad Y, Mirdad M, et al. Oral health knowledge, attitudes, and behaviors among university students in Jeddah, Saudi Arabia. Clin. Cosmet. Investig. Dent 2020; 12: 515. [ Links ]
3. Petersen PE, Bourgeois D, Ogawa H, et al. The global burden of oral diseases and risks to oral health. Bull. World Health Organ. 2005; 83: 661669. [ Links ]
4. Peres MA, Macpherson LM, Weyant RJ, et al. Oral diseases: a global public health challenge. Lancet 2019; 394: 249-260. [ Links ]
5. 5. Regional Committee for Africa. Regional oral health strategy 2016-2025: addressing oral diseases as part of NCDs (Document AFR/ RC66/5). World Health Organization. Regional Office for Africa. 2016. [ Links ]
6. WHO. World Oral Health Day 2022. 2022. WHO Regional Office for Africa. [ Links ]
7. Hobdell M, Clarkson J, Petersen P, et al. Global goals for oral health 2020. Int Dent J 2003; 53: 285-288. [ Links ]
8. Onwubu SC, Mdluli PS and Singh S. Evaluating the buffering and acid-resistant properties of eggshell-titanium dioxide composite against erosive acids. J. Appl. Biomater. Funct. Mater 2019; 17: 2280800018809914. [ Links ]
9. Kathmandu RY. The burden of restorative dental treatment for children in Third World countries. Int Dent J 2002; 52: 1-9. [ Links ]
10. Glick M, Williams DM, Kleinman DV, et al. A new definition for oral health developed by the FDI World Dental Federation opens the door to a universal definition of oral health. Br Dent J 2016; 221: 792-793. [ Links ]
11. Peltzer K and Pengpid S. Oral health behaviour and social and health factors in university students from 26 low, middle and high income countries. Int. J. Environ. Res. Public Health 2014; 11: 12247 12260. [ Links ]
12. Bashiru BO and Omotola OE. Oral health knowledge, attitude and behavior of medical, pharmacy and nursing students at the University of Port Harcourt, Nigeria. J. Oral Res. Rev 2016; 8: 66. [ Links ]
13. Kumar H, Behura SS, Ramachandra S, et al. Oral health knowledge, attitude, and practices among dental and medical students in Eastern India-A comparative study. J. Int. Soc. Prev. Community Dent 2017; 7: 58. [ Links ]
14. Al Subait AA, Alousaimi M, Geeverghese A, et al. Oral health knowledge, attitude and behavior among students of age 10-18 years old attending Jenadriyah festival Riyadh; a cross-sectional study. Saudi J Dent Res 2016; 7: 45-50. [ Links ]
15. Peker I and Alkurt MT. Oral health attitudes and behavior among a group of Turkish dental students. Eur. J. Dent 2009; 3: 24-31. [ Links ]
16. Petersen PE, Baez RJ and World Health Organization. Oral health surveys: basic methods. 5th ed.: World Health Organization., 2013. [ Links ]
17. Zhu L, Petersen P, Wang H, et al. Oral health knowledge, attitudes and behavior of children and adolescents in China. Int Dent J 2003; 5: 289-298. [ Links ]
18. Vadiakas G, Oulis C, Tsinidou K, et al. Socio-behavioural factors influencing oral health of 12 and 15 year old Greek adolescents. A national pathfinder survey. Eur Arch Paediatr Dent 2011; 12: 139-145. [ Links ]
19. Broadbent J, Thomson W and Poulton R. Progression of dental caries and tooth loss between the third and fourth decades of life: a birth cohort study. Caries Res 2006; 40: 459-465. [ Links ]
20. Abid A, Maatouk F, Berrezouga L, et al. Prevalence and severity of oral diseases in the Africa and Middle East Region. Adv. Dent. Res 2015; 27: 10-17. [ Links ]
21. Suprabha BS, Rao A, Shenoy R, et al. Utility of knowledge, attitude, and practice survey, and prevalence of dental caries among 11-to 13-year-old children in an urban community in India. Glob. Health Action 2013; 6: 20750. [ Links ]
22. Rad M, Shahravan A and Haghdoost AA. Oral health knowledge, attitude, and practice in 12-year-old schoolchildren in Iran. J Int Soc Prev Community Dent 2015; 5: 419. [ Links ]
23. Mitrakul K, Laovoravit V, Vanichanuwat V, et al. Factors associated with parent capability on child's oral health care. Southeast Asian J Trop Med Public Health 2012; 43: 249. [ Links ]
24. Sambunjak D, Nickerson JW, Poklepovic T, et al. Flossing for the management of periodontal diseases and dental caries in adults. Cochrane Database Syst Rev 2019. [ Links ]
25. Jaber MF, Khan A, Elmosaad Y, et al. Oral health knowledge, attitude and practices among male Qassim university students. Int J Community Med Public Health 2017; 4: 2729-2735. [ Links ]
26. Wahengbam PP, Kshetrimayum N, Wahengbam BS, et al. Assessment of oral health knowledge, attitude and self-care practice among adolescents-a state wide cross-sectional study in Manipur, North Eastern India. J. Clin. Diagnostic Res 2016; 10: ZC65. [ Links ]
27. Beaton L, Freeman R and Humphris G. Why are people afraid of the dentist? Observations and explanations. Med Princ Pract 2014; 23: 295-301. [ Links ]
28. Kassak KM, Dagher R and Doughan B. Oral hygiene and lifestyle correlates among new undergraduate university students in Lebanon. J Am Coll Health 2001; 50: 15-20. [ Links ]
29. Harris NO and Garcia-Godoy F. Primary preventive dentistry. 8th ed.: Upper Saddle River, NJ: Pearson Education, 2014. [ Links ]
30. Clark-Perry D and Levin L. Comparison of new formulas of stannous fluoride toothpastes with other commercially available fluoridated toothpastes: A systematic review and meta-analysis of randomised controlled trials. Int Dent J 2020; 70: 418-426. [ Links ]
31. Tada A and Hanada N. Sexual differences in oral health behaviour and factors associated with oral health behaviour in Japanese young adults. Public Health 2004; 118: 104-109. [ Links ]
 Correspondence:
Correspondence:
Onwubu Stanley Chibuzor
Chemistry Department, Durban University of Technology (DUT)
Durban, South Africa
Email: 21445599@dut4life.ac.za
Author contributions:
1 . Stanley Chibuzor Onwubu 25%
2 . Kingsley Chukwuka Ogwo 25%
3 . Uchenna Promise Onyeny 25%
4 . Getrude Chika Iwueke, Advisor 15%
5 . Thabang Hendrica Mokhothu 10%


{kind=link}