










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Dental Journal
versión On-line ISSN 0375-1562
versión impresa ISSN 0011-8516
S. Afr. dent. j. vol.77 no.8 Johannesburg sep. 2022
http://dx.doi.org/10.17159/2519-0105/2022/v77no8a3
RESEARCH
Pharmaceutical cost implications for oral healthcare interventions at a dental clinic in Windhoek, Namibia
BS SinguI; P ShaamenaII
IBSc, BPharm, MPharm, School of Pharmacy, University of Namibia, ORCID: 0000-0002-5663-522X
IIMBChB, School of Medicine, University of Namibia, ORCID: 0000-0003-1414-8076
ABSTRACT
INTRODUCTION: Half of the world's 7.9 billion population suffers from oral health conditions. Most are largely preventable and treatable but costs are often unaffordable especially in developing countries. The World Health Organization (WHO) resolved in 2021 to include oral healthcare interventions in universal healthcare coverage (UHC) programmes. Although the general expenditure on oral healthcare services has been reported by some countries, amounts spent on particularly pharmaceuticals have not been reported
AIMS AND OBJECTIVES: This study aimed to report on the prevalence of different types of oral health diseases in patients attending a dental clinic in Windhoek (Namibia) and quantify the pharmaceutical expenditure incurred.
METHODS: Records for all patients who visited the dental clinic at KIRH during a six-month period (1 January 2021 to 30 June 2021) were reviewed. Costs associated with the respective pharmaceutical management options for the most common oral conditions were calculated based on the approximated cost for a single treatment course per patient
RESULTS: Pharmaceutical expenditure on oral diseases was approximately 0.4% of the hospital's annual budget. From this, 94.6% was due to treatment of dental caries which had a 90.1% prevalence. Prevalence of dental caries among 13-19 years age group (9.5%) was lower than for 1-12 years (18.6%) and 20-64 years (68.2%). Cases for dental caries were fewer for the 65+ years age group (3.8% of total cases) but had the highest prevalence (95.2%) of dental caries then other age groups
CONCLUSIONS: The proportion of the pharmaceutical budget spent on treating oral diseases was 0.4%, of which 94.6% was due to dental caries. Promotion of oral healthcare among children may be instrumental in reducing the pharmaceutical costs associated with treatment of dental carries
Keywords: oral health, dental caries, universal healthcare, pharmaceuticals, costs, Namibia.
INTRODUCTION
Approximately half of the world's 7.9 billion population suffers from oral health conditions.1 Most oral diseases are largely preventable and treatable if presented earlier but treatment is usually not part of universal health coverage (UHC) packages and often unaffordable especially in developing countries; for this reason, the World Health Organization (WHO) resolved in 2021 to include oral healthcare interventions in UHC programmes.2,3 However, financing of medicines, fees for consultations, and procedures are known barriers to implementation of UHC especially in Low- and Middle-income Countries (LMICs).4 Although the general expenditure on oral healthcare services has been reported by some countries to be around 5%, the amounts spent on pharmaceuticals in particular as part of treating oral diseases has not been reported.5,6 The purpose of this study was to report on the prevalence of different types of oral health diseases in patients attending the dental clinic at Katutura Intermediate Referral Hospital (KIRH) in Windhoek (Namibia) and quantify the pharmaceutical expenditure incurred in treatment of patients at this clinic.
Namibia is a LMIC African country with an estimated population of 2.5 million. Its total expenditure on health is roughly 8.9% of its Gross Domestic Product (GDP). 7,8 Windhoek, the capital city of Namibia, has around 400,000 inhabitants of which the vast majority's health needs are served by KIRH, the busiest hospital in the country. The dental clinic located at this hospital is visited by 80 patients per day, and has a staff compliment of 8 dentists, 6 dental assistants, 1 nurse, 1 dental lab technician, and 1 prosthodontic specialist.
METHODS
Data for this retrospective study were retrieved from register books at the Dental Clinic of KIRH, Windhoek, Namibia. Records for all patients who visited the clinic during a six-month period (1 January 2021 to 30 June 2021) were reviewed and included in the data analysis if they had all required Information, which were: age, sex, diagnosis/dental condition, and treatment/intervention. The costs associated with the respective pharmaceutical management options for the most common dental conditions were calculated based on the approximated cost for a single treatment course per patient, the exchange rate at the time of this study was 1.00 United States Dollar = 15.00 Namibian Dollars, (Table 1). Descriptive statistical analysis to summarize the results were performed using Microsoft® Excel, version 16.53 (Microsoft Corp., Redmond, Washington, USA).
Approval to conduct this study was obtained from the Ministry of Health and Social Services (MoHSS) Ethics Committee.
RESULTS
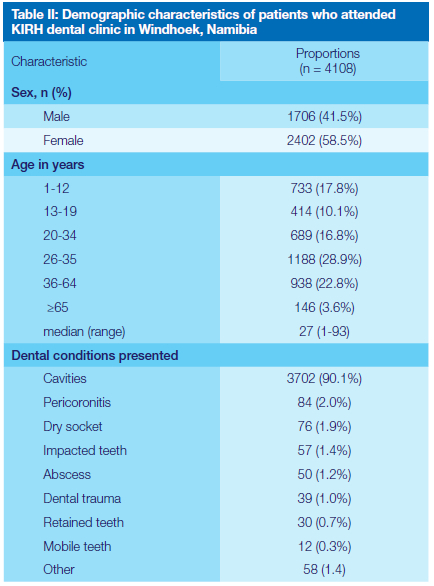
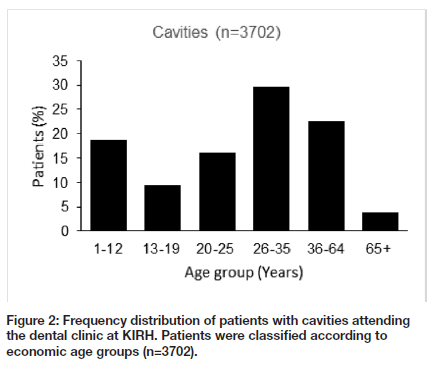
Of the total 6,516 patients seen at the Katutura Hospital dental clinic during the six-month study period (1 January - 30 June 2021), 2,408 were excluded from the data analysis due to missing data such as age, sex, diagnosis, or treatment/intervention. The 4,108 patients included in this study had a median age of 27 years (range:1-93 years) and comprised of 1,706 (41.5%) males and 2,402 (58.5%) females. The 26-35 years age group were the largest patient group (28.9%) while the 65+ years group had the lowest numbers (3.6%). More patients came to the clinic for the first time (59.5%) than for a follow-up visit (40.5%). The most common dental conditions presented at the clinic (Table 2) were cavities (90.1%), pericoronitis (2.0%) and dry socket (1.9%). For cavities alone, the age group of 1-19 years accounted for 28.1%, those between 20-25, 26-35 and 36-64 years together (adults) accounted for 68.2%, while the 65+ years group was 3.8% of the cases (Figure 2). Within age groups, the highest prevalence of dental carries was among the 65+ year-olds (95.2%), followed by the 1-12-year-olds (94.9%) and the lowest being within the 13-19-year-olds (87.2%).
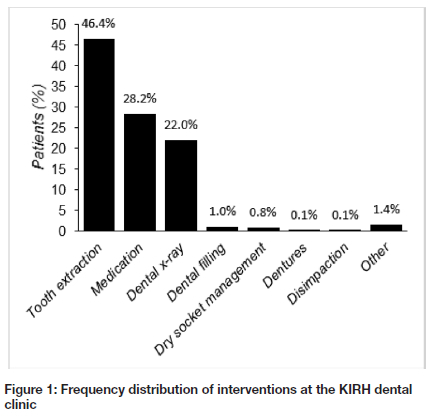
Only a small number of patients (0.2%) received no intervention/treatment on the date of their visit, the vast majority received at least one intervention; 12.1% had 1 intervention, 85.8% had a combination of 2 interventions, and 1.9% had 3 interventions. The most common interventions (Figure 1) were tooth extraction(46.4%), medication (28.2%), and dental x-ray (22.0%).
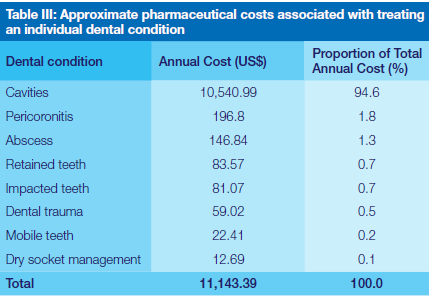
Disease conditions due to infections were treated with combination therapy (taken orally) of amoxicillin (or cefuroxime) + metronidazole + paracetamol for 5 days while pain was managed by common analgesics mostly paracetamol and/or ibuprofen for 3-5 days. The calculated pharmaceutical costs for the 4,050 patients (excluding 58 which were counted as 'Other') was US$ 3,482.31 over the study period. Adjusting this figure to include all the 6,516 patients who presented to the dental clinic during the six-month study period and projecting the costs to 12 months (13,032 patients) brings the total annual pharmaceutical costs at this clinic to approximately US$ 11,143.38 which is 0.4% of the total pharmaceutical budget for the entire hospital. Disease conditions that incurred the highest annual pharmaceutical costs were cavities (dental caries), pericoronitis, and abscess (Table 3).
DISCUSSION
The WHO reports that access to prevention, early diagnosis and treatment of oral diseases is far from universal and remains unattainable for millions of people in poor nations.3 Although it is commendable that WHO intends to implement the primary healthcare strategy of promoting community-based preventative interventions such as water fluoridation and advocating for recognition of fluoride tooth paste as an essential health product,3 it is necessary for the cost of pharmaceuticals to also be considered in order to address the aspect of access to treatment. While access to essential medicines is regarded as vital to achieving UHC, it is known that the majority of people in low- and middle-income countries (LMICs) have no access to essential medicines mostly due to a lack of financing.9 Quantification of pharmaceutical costs associated with treatment of dental conditions will help policy makers and governments of LMICs to make informed decisions in efforts to include oral healthcare interventions in their UHC programmes.
In this study, the interventions made on outpatients who attended a dental clinic at a major state hospital in Windhoek (Namibia) were studied and the pharmaceutical costs associated with treating each of the mostly presented oral health diseases were estimated. At KIRH, 74.6% of the patients who visited the dental clinic received an intervention that involved the use of pharmaceuticals (Figure 1). The total annual cost of pharmaceuticals required to treat patients at this dental clinic was estimated at US$11,143.38 which is 0.4% of the hospital's entire budget allocated to pharmaceuticals in 2021. The hospital at which this study was conducted is one of the two largest state hospitals in Namibia and it is unlikely that the proportion of pharmaceutical costs for dental interventions at this hospital would be the same at all the other state hospitals around the country, therefore generalizing this figure to be true at the national level is a limitation. Nonetheless, using this figure of 0.4% and taking the reported national annual expenditure on pharmaceuticals for Namibia as US$58,300,000.00,6 the corresponding national cost on pharmaceuticals for treating oral health diseases would be inferred to be around US$233,200.00, of which roughly US$220,600.00 goes to treating cavities alone. Since cavities were the most commonly presented condition, as is reported globally,10-12 it is not surprising that such a high proportion (94.6%) of the estimated pharmaceutical costs at this dental clinic were due to treatment of this disease. The majority of patients with dental caries in this study were adults (68.2%), followed by children (18.6%), adolescents (9.5%) (and a small percentage were elderly (Figure 2). These demographics suggest that oral hygiene seems to be better in the high school age group (13-19 years old) in comparison to pre-primary and primary school children (1-12 years old).
However, the elderly are the worst affected by dental caries as an age group. It could be argued that promotion of oral health hygiene in primary school children could lead to a reduction in the high prevalence of dental caries in the older age groups and therefore result in lower pharmaceutical expenditure on treatment. Studies have demonstrated the cost-effectiveness of preventative interventions against dental caries in children such as promotion of the use of fluoridated tooth paste and water fluoridation.13 However, there is a gap in the literature with regard to pharmaceutical costs associated with the treatment of dental carries and other oral health diseases in both high-income countries and LMICs. Namibia's reported expenditure on general dental treatment is around 5% of total health expenditure, which is the same figure reported for high-income countries.5,6 LMICs fail to provide services for prevention and treatment of oral health conditions majorly due to a lack of UHC programmes.14 In essence, the objectives of developing UHC packages are to provide good value for money spent on healthcare, and address a significant disease burden, such as dental carries.15 Countries are encouraged to have financing systems that enable provision of all types of UHC services such as promotion, prevention, treatment and rehabilitation at the lowest cost possible.4 As policy makers in LMICs begin to implement the resolution by WHO to include oral healthcare Interventions In UHC programmes, the associated pharmaceutical expenditure must be taken Into account to enable sincere financial assessments and adoption of better-informed financing strategies.
In conclusion, dental caries was the most commonly presented oral disease at this dental clinic accounting for 90.1% of all disease conditions and 94.6% of pharmaceutical expenditure on treating oral diseases. This study has suggested an estimate of around 0.4% of the local or national pharmaceutical budget for provision of pharmaceutical management of oral health conditions. Promotion of oral healthcare practices among primary school children may be instrumental in reducing the pharmaceutical costs associated with treatment of dental carries. In designing and implementing UHC programmes, LMICs should not only consider preventative strategies, but also the pharmaceutical costs associated with treating oral diseases.
Conflicts Of Interest
The authors have no conflicts of interest to declare that are relevant of the content of this article.
REFERENCES
1. James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 Diseases and Injuries for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789-858. [ Links ]
2. World Health Organization. Proposed Resolution on Oral health 2021 [Internet]. Zurich; 2021. Available from: https://www.who.int/news/item/27-05-2021-world-health-assembly-resolution-paves-the-way-for-better-oral-health-care [ Links ]
3. World Health Organization. Consolidated report by the Director-General 1. Vol. 2030, Seventy-fourth World Health Assembly. 2021. [ Links ]
4. World Health Organization. The world health report 2010. Health systems financing: the path to universal coverage. Zurich; 2010. [ Links ]
5. OCDE. Health at a Glance 2017: Chartset [Internet]. European Observatory on Health Systems and Policies (2017). 2017. Available from: https://www.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-2017_health_glance-2017-en%0Ahttps://www.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-2017_health_ glance-2017-en%0Ahttp://www.oecd-ilibrary.org/educatio [ Links ]
6. World Bank. Namibia Health Sector Public Expenditure Review [Internet]. 2019. Available from: https://documents1.worldbank.org/curated/en/268141563376806867/pdf/Namibia-Health-Sector-Public-Expenditure-Review.pdf [ Links ]
7. World Health Organization. Namibia [Internet]. Available from: https://www.who.int/countries/nam/ [ Links ]
8. World Bank. Namibia At-A-Glance [Internet]. Available from: https://www.worldbank.org/en/country/namibia [ Links ]
9. Ozawa S, Shankar R, Leopold C, Orubu S. Access to medicines through health systems in low-and middle-income countries. Health Policy Plan. 2019;34:III1-3. [ Links ]
10. Political Declaration of the High-level Meeting of the General Assembly on the Prevention and Control of Noncommunicable Diseases. 2011. [ Links ]
11. Subrata S, Subrata S. Prevalence and severity of dental caries and oral hygiene status in rural and urban areas of Calcutta. J Indian Soc Pedod Prev Dent. 1996;14:17-20. [ Links ]
12. Jaiswal D, Kalia P, Hiremath S, Singh AK, Pani P, Kumar N. Evaluation of oral hygiene status among 12-14 year-old school children. J Pharm Bioallied Sci. 2021;13(Suppl 1):S112-5. [ Links ]
13. Tickle M, O'Neill C, Donaldson M, Birch S, Noble S, Killough S, et al. A randomised controlled trial to measure the effects and costs of a dental caries prevention regime for young children attending primary care dental services: The Northern Ireland caries prevention in practice (NIC-PIP) trial. Health Technol Assess (Rockv). 2016;20(71):vii-96. [ Links ]
14. World Health Organization. Oral health [Internet]. 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/oral-health [ Links ]
15. Jamison DT. Disease Control Priorities, 3rd edition: improving health and reducing poverty. Vol. 391, The Lancet. 2018. 11-14 p. [ Links ]
 Correspondence:
Correspondence:
Bonifasius S Singu
School of Pharmacy, University of Namibia
Private Bag 13301, Windhoek, Namibia
Tel: +264 61 206 5052
Email: bsingu@unam.na
Author contributions:
1 . Bonifasius S Singu 70%
2 . Priscila Shaamena 30%


{kind=link}