










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.77 n.7 Johannesburg Aug. 2022
http://dx.doi.org/10.17159/2519-0105/2022/v77no7a10
RADIOLOGY CASE
C SmitI; L RobinsonII
IBChD, MSc (Maxillofacial and Oral Radiology). Department of Oral and Maxillofacial Pathology, University of Pretoria. ORCID: 0000-0003-4047-6356
IIBChD, PDD (MaxillofacialRadiology), PDD (Forensic Odontology), MChD (Oral Path), FC Path (SA) Oral Path. Department of Oral and Maxillofacial Pathology, University of Pretoria. ORCID: 0000-0002-0549-7824
CASE
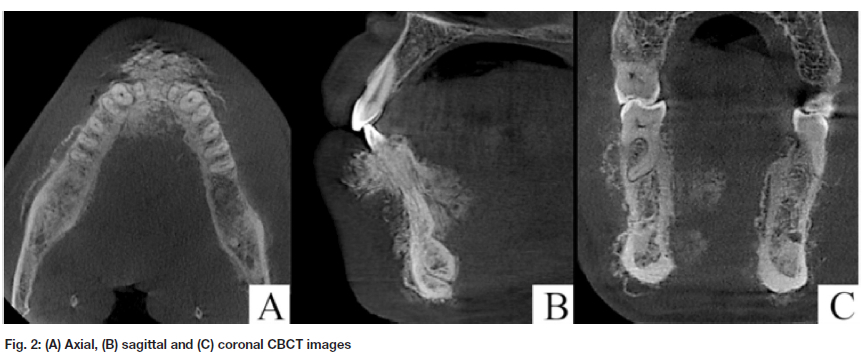
A 30-year-old male patient, RVD-reactive on treatment, presented with a fast-growing, painful swelling involving the mandible of unknown duration. A panoramic radiograph (PR) and cone-beam computed tomography (CBCT) imaging were performed. What are the pertinent radiological features and your diagnostic hypothesis?
INTERPRETATION
The panoramic radiograph showed a poorly-defined, hazy and sclerotic appearance of the anterior mandibular bone. CBCT imaging showed a poorly-defined, hyperdense lesion resulting in a so-called "sunburst" periosteal reaction of the anterior mandible. This periosteal reaction extended to involve the mandible bilaterally. These features supported the histopathological diagnosis of osteosarcoma.
Osteosarcomas are a group of malignant bone neoplasms that constitute approximately 50% of all skeletal malignancies, with 10% of cases occurring within the jawbones.1 Osteosarcomas may arise de novo or following radiotherapy to the head and neck region.2 They present with a near equal gender distribution and at a median age of 38 years, with males often presenting at an earlier age.3 The mandible (56%), maxilla (32%), paranasal sinuses (10%), and the rest of the skull including the skull base (2%) are affected in decreasing frequencies.1
The most common presentation is that of a painful or painless swelling present for a short period.1 Radiologically, they present as poorly-defined osteolytic, mixed or osteogenic lesions.2 Periosteal reactions are common (65%) and may be laminated or spiculated.2 Soft tissue invasion is seen in 48% of cases.1 Treatment consists of primary surgical resection and neoadjunct chemo- or radiotherapy in many cases.1 The 5-year disease-free survival rate has been estimated at 60%3, with a median overall survival of 46 months.1 Factors associated with a worse prognosis include patients over the age of 60 years, location other than the mandible, tumours larger than 6cm, histologic subtype, initial non-surgical therapy, and positive resection margins.3
It is the dentist's responsibility to recognise the early radiological signs, particularly mobile teeth with symmetrical widening of the periodontal ligament space in the absence of periodontal disease. This will ensure early patient referral and diagnosis, and improve overall survival rates.
Authors declaration Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethics approval
This study was approved by the University of Pretoria, Faculty of Health Sciences Research Ethics Committee (Reference no.: 411/2022). All procedures followed the ethical standards of the Helsinki Declaration of 1975, as revised in 2008.
REFERENCES
1. Laskar S, Basu A, Muckaden MA, D'Cruz A, Pai S, Jambhekar N, Tike P, Shrivastava SK. Osteosarcoma of the head and neck region: lessons learned from a single-institution experience of 50 patients. Head & Neck: Journal for the Sciences and Specialties of the Head and Neck. 2008 Aug;30(8):1020-6. [ Links ]
2. Luo Z, Chen W, Shen X, Qin G, Yuan J, Hu B, Lyu J, Wen C, Xu W. Head and neck osteosarcoma: CT and MR imaging features. Dentomaxillofacial Radiology. 2020 Feb;49(2):20190202. [ Links ]
3. Smith RB, Apostolakis LW, Karnell LH, Koch BB, Robinson RA, Zhen W, Menck HR, Hoffman HT. National Cancer Data Base report on osteosarco-ma of the head and neck. Cancer: Interdisciplinary International Journal of the American Cancer Society. 2003 Oct 15;98(8):1670-80. [ Links ]
 Correspondence:
Correspondence:
Chané Smit
Department of Oral and Maxillofacial Pathology
University of Pretoria.
Tel +27 (0)12 319 2311
Email: chane.smit@up.ac.za
Authors contribution:
Chané Smit: 50%
Liam Robinson: 50%


{kind=link}
{kind=link}