










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.77 no.6 Johannesburg Jul. 2022
http://dx.doi.org/10.17159/2519-0105/2022/v77no6a3
RESEARCH
Students' knowledge, attitudes and practices related to infection control in undergraduate dental clinical training during COVID-19 A report from one South African university
S SinghI; R MoodleyII; I MoodleyIII
IPhD, PhD, School of Health Sciences, Discipline of Dentistry, School of Health Sciences, College of Health Sciences, University of KwaZulu-Natal, South Africa. ORCID: 0000-0003-4842-602X
IIPhD, School of Health Sciences, Discipline of Dentistry, School of Health Sciences, College of Health Sciences, University of KwaZulu-Natal, South Africa. ORCID: 0000-0003-2703-9370
IIIPhD, School of Health Sciences, Discipline of Dentistry, School of Health Sciences, College of Health Sciences, University of KwaZulu-Natal, South Africa. ORCID: 0000-0001-5834-9887
ABSTRACT
The COVID-19 pandemic has highlighted the need for renewed conversations in infection control in the context of dental undergraduate learning.
OBJECTIVES: This study set out to examine dental therapy and oral hygiene students' knowledge, attitudes and practices related to infection control
METHODS: This quantitative survey was conducted at one dental training site in South Africa. The study population comprised 156 full time enrolled students that was stratified into Year 1 (n=55), Year 2 (n=54) and Year 3 (n=47). An online, self-administered questionnaire with closed and open-ended questions was used to collect information. Data were analyzed using SPSS version 25.0 (IBM Corp., USA) and thematic analysis
RESULTS: The response rate for the study was 70.5% (n=111). Almost all participants (n=104) strongly agreed/agreed that COVID-19 is transmitted mainly through infected droplets. Most participants (Year 1: n=24, 22.5%; Year 2: n=28, 26.2%; Year 3: 22, 31.2%) strongly disagreed / disagreed that younger people were less susceptible to contracting COVID-19 disease. While 23 first (21.5%) and 16 second-year students (14.9%) strongly agreed/agreed that personal protective gear was sufficient protection against COVID-19, about 16 third-year students (14%) were unsure or disagreed. Almost all participants (n=105, 98.1%) strongly agreed/agreed to washing or sanitizing their hands regularly. The emergent themes from qualitative data analysis included: better access to resources and more coordinated planning for clinical and classroom-based learning
CONCLUSION: There were inconsistencies in participants' knowledge and attitudes towards infection control. There is a need for ongoing awareness of infection control in both clinical and class-room based learning
Keywords: incontrol, COVID-19, dental students, learning
INTRODUCTION
Cross-contamination in the dental clinical environment remains a significant public health concern given the high risk of exposure to blood and airborne infections.1-2 In addition, the use of high-speed hand pieces and ultrasonic scalers during dental clinical procedures can create aerosols that could potentially transfer air-borne infections beyond the dental working environment. Apart from these possible sources of cross contamination, the environmental work surfaces and water lines of dental units could also pose a potential risk.3 Standard (universal) precautions in infection control include hand washing/ disinfection; use of personnel protective equipment (e.g. gowns, protective eye wear, and gloves); use of disinfectants for clinic surface cleaning; and appropriate handling and disposal of contaminated sharp instruments and other clinical waste.4-6 While infection control is described as the prevention of disease transmission in health care and clinical settings,7 this definition and scope requires a re-examination in light of the COVID-19 pandemic.
The need for public health measures to include infection control practices such as regular handwashing, sanitization with at least 70% alcohol-based solutions and wearing of facial masks in public spaces, in addition to social distancing, isolation and quarantine,8 somewhat provides an expanded understanding of infection control practice. The need to break the chain of infection now extends beyond the clinical settings and is seen as the 'new normal'.9
Although the COVID-19 pandemic has been in existence for more than a year, not much is known about undergraduate dental students' preparedness to deal with this pandemic.10-12 The risks associated with dental clinical service delivery such as cross infection, and close contact with patients, clinical supervisors and fellow students are well documented yet the extent to which COVID-19 complicates this already high-risk environment,13-14 especially from a clinical training perspective, remains largely unknown. Nevertheless, patients, students, dental operators, staff and the public at large have a right to access or provide oral health care within a safe and healthy clinical environment.15
This study arose out of a need to understand the contextual influences on theory based and clinical teaching during COVID-19, and undergraduate students' understanding and preparedness for learning during this pandemic. Using a student-centred approach,16 students' perspectives and input should be taken into consideration when reviewing and adapting the undergraduate curriculum to meet the demands of a changing teaching and learning environment during COVID-19. The study thus aimed to contribute to curriculum review by determining undergraduate dental students' knowledge, attitudes and practices related to infection control in response to clinical and classroom-based learning during the COVID-19 pandemic.
This study formed part of a larger study that examined undergraduate students' perspectives on learning during the COVID-19 pandemic.
Study population and methodology
This quantitative survey was conducted at one dental training site to determine undergraduate Dental Therapy and Oral Hygiene students' knowledge, attitudes and practices related to infection control during COVID-19. There are currently two undergraduate training programmes offered by the Discipline of Dentistry, namely, B. Dental Therapy and B. Oral Hygiene at the identified training institution. A whole population approach was used thus the study population comprised 156 full time enrolled students. The study population was stratified into Year 1 (n=55), Year 2 (n=54) and Year 3 (n=47). The B. Oral Hygiene only commenced in 2020 thus only first year students were included in the study. This study was conducted at the end of the second semester in 2020 and students had already been exposed to almost nine months of teaching and learning during the COVID-19 pandemic. Ethics approval (Ref. No. HSSREC/00001601/2020) and gatekeeper permission were obtained prior to commencement of this study.
An online, self-administered questionnaire was developed to determine students' knowledge, attitudes, and infection control practices related to clinical learning during the COVID-19 pandemic. The data collection tool comprised of four sections; Section A focused on student demographics, Sections B, C, and D focused on knowledge of COVID-19 disease transmission, attitudes towards susceptibility to infection, use of personal protective equipment, and infection control practices (such as handwashing, care of personal belongings). The questionnaire comprised closed questions using a Likert scale format with responses ranging from 1 (strongly agree), 2 (agree), 3 (not sure), 4 (disagree) to 5 (strongly disagree). one open-ended question was used to elicit participants' recommendations to improve infection control in undergraduate dental learning. All returned questionnaires were coded (e.g P1) to ensure anonymity of study participants.
Participants were recruited through the social media platform WhatsApp, using a snowball sampling technique. An invitational message was sent to the first student to consider participating in the study. This message included a link to the informed consent documents and survey questionnaire. Once the student clicked on the link, he/she had to give consent by clicking on the necessary icon. The participant was then given a choice to complete the survey. The participant was also given a choice to forward the survey link to the next student with each participant remaining anonymous. The link remained active for approximately six weeks to allow study participation.17 Participants had the right to withdraw and any stage of the study without any negative consequences.
For data analysis, the collected information from the closed ended questions was analyzed using SPSS version 25.0 (IBM Corp., USA) after the data were cleaned and coded. Data analysis included univariate descriptive statistics such as frequency and mean distribution. An inferential statistical technique, the Pearson chi-squared test was used to determine a relationship between the independent variable (year of study) and the dependent variables (knowledge, attitudes and practices). A p-value of <0.05 was established as being statistically significant. The open-ended question was analyzed using thematic analysis. The response from each student was first transcribed verbatim. The data was coded and then organized into code groups. Each code group was further examined for patterns and emergent themes. Confirmability was established by quoting actual responses of students
RESULTS
The response rate for the study was 70.5% (n=111). The majority of study participants were female (n=72, 68%) and were registered for the Dental Therapy programme (97%). There were almost equal numbers of respondents over the three years of study: Year 1 (n=33, 30.8%), Year 2 (n=33, 30.8%), Year 3 (n=41, 38.3%).
Knowledge of infection control
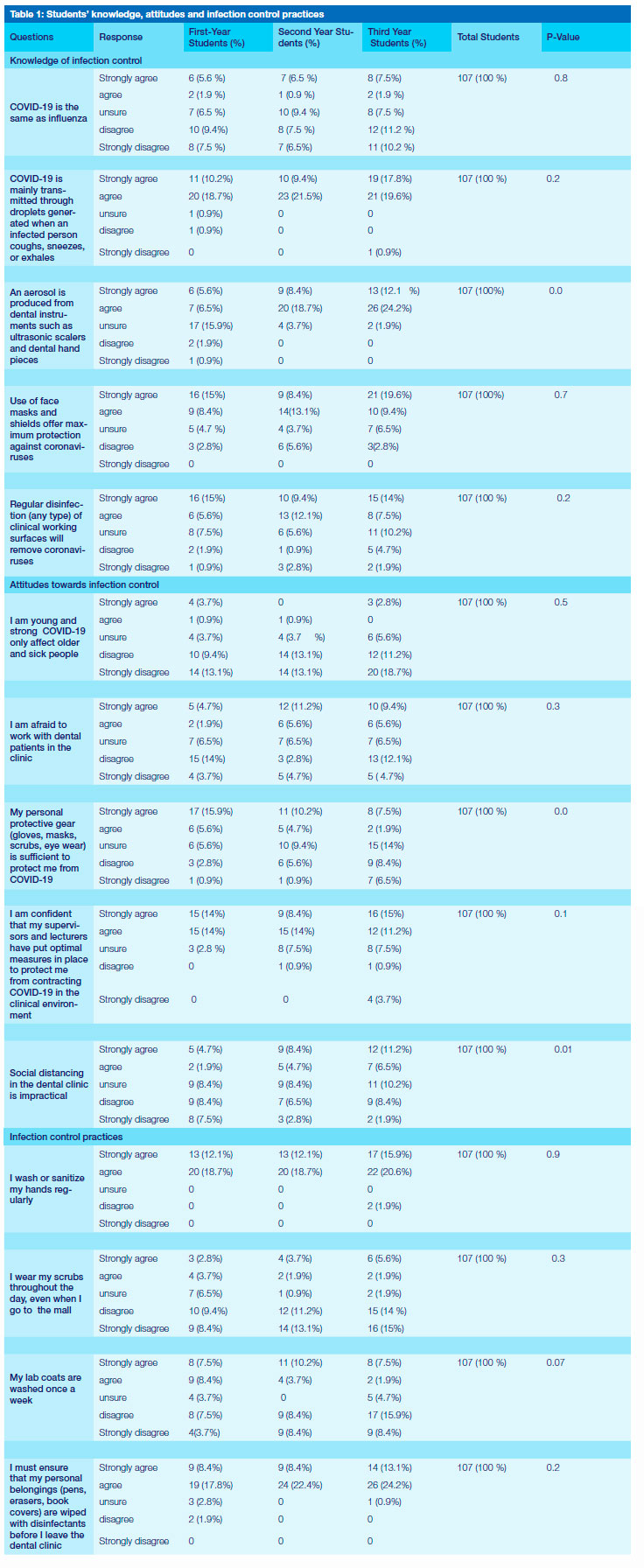
More students in first (n=18, 16.9%) and third years (n=23, 21.4%) strongly disagreed/disagreed that COVID-19 is the same as influenza. Interestingly, 10 participants (9.4 %) in the second year and 8 (7.5 %) in the third year were unsure (Table 1). Most participants (Year 1: n=31, 28.9%; Year 2: n=33, 40.9%; Year 3:
n=40, 37.4%) strongly agreed/agreed that COVID-19 is mainly transmitted through droplets generated when an infected person coughs, sneezes, or exhales. Almost 36.3% of third years (n=39) strongly agreed/agreed that an aerosol is produced from dental instruments such as ultrasonic scalers and dental hand pieces. About 17 first year students (15.9%) were unsure. This finding was seen as statistically significant (0.000). While the majority of participants (n=79, 73.9%) strongly agreed/ agreed that the use of face masks and shields offer maximum protection against coronaviruses, about 16 participants (14.9%) were unsure.
Attitudes towards infection control
The majority of participants (Year 1: n=24, 22.5%; Year 2: n=28, 26.2%; Year 3: 22, 31.2%) strongly disagreed /disagreed that younger people were less susceptible to contracting COVID-19 disease. About 18 second (17.2%) and 16 third year students (15%) expressed fear of working with dental patients in the clinic. Interestingly, 19 first year students (17.7%) strongly disagreed /disagreed with this statement. While 23 first (21.5%) and 16 second year students (14.9) strongly agreed/agreed that personal protective gear (gloves, masks, scrubs, eye wear) is sufficient to protect them from COVID-19, about 15 third year students (14%) were unsure or disagreed with the statement (n=16, 14,9%).
The majority of participants (n=82, 76.6%) were confident that optimal measures were in place to protect students from contracting COVID-19 in the clinical environment.
Only 7 first (6.6%) and 19 third year students (18.7%) strongly agreed/agreed that social distancing in the dental clinic is impractical. At the same time 11 third year students (10.2%) were unsure (=0.01).
Infection control practices
Almost all participants (n=105, 98.1%) strongly agreed/agreed that they washed or sanitized their hands regularly. The majority of participants (Year 1: 19,17.8%; Year 2: n=26, 24.3%; Year 3: n=31, 29%) strongly disagreed/disagreed that the scrubs were worn throughout the entire day. About 17 first (15.9%) strongly agreed/agreed that the laboratory coats were washed once a week while 18 second (16.8%) and 26 third year students (24.3%) strongly disagreed/ disagreed with this statement. Almost all participants (n=101, 94.3%) strongly agreed/agreed that one should ensure that personal belongings (pens, erasers, book covers) are wiped with disinfectants before leaving the dental clinic.
Several emergent themes were obtained in response to the question: How can we improve infection control during clinical and class room based- learning? These included the availability of resources for better infection control practices; the need for coordinated planning in clinical training and re-organization of class-based learning. These themes inadvertently highlighted the current gaps in creating a safe and heathy environment for student learning at the identified research site.
Availability of resources for better infection control practices
Respondents indicated the need for increased availability in personal protective equipment (PPE). While gowns, face shields, and N95 masks were made available for student learning in the clinical environment, some respondents expressed concern over the quality of N95 masks, while others were dissatisfied on having to use the same PPE for a week or more. Likewise, respondents pointed out there were limited availability of hand sanitizers.
The following quotes illustrate these expressed views: It's not logical to use one N95 mask for an entire week. The quality of our N95 masks are poor as well. The elastics tear easily (4).
Provide students with new N95 masks and gowns everyday or every session. At clinics we are expected to use two masks and 2 gowns for 2 weeks straight. We are expected to use the same hairnet throughout the day. Shoe covers are not provided. Students have to wait in a classroom in order to fill in their COVID [screening] form and [have] their temperature [checked], No social distancing can be carried out (14).
Provide more sanitizer bottles in the clinic as were always fighting over the 3 bottles that are currently available. The spray bottle makes it easier to clean (3).
The need for coordinated planning for clinical training
Respondents outlined the need for better coordination in clinical training so as to optimize students' health and safety in clinical training. A major sub-theme arising was the need for students to practice proper social distancing in the clinical environment. Respondents highlighted the need for regular temperature checks, and for reminders to be put up for handwashing or hand sanitization. Other reported recommendations for improving clinical training included better ventilation in the clinic, and repair of non-functioning dental clinical units. Respondents also iterated the need for small groups of students during clinical rotation.
We need proper ventilation in our working area (55) Fix malfuctioning cubicles to have more space for everyone to work, Please!!!!! (32)
Re-organization of class-based learning
Concurrently, the need for optimal infection control practices was also seen to be pertinent for class-room based learning as well.
All desks and chairs must be cleaned before students use it and again for the next set of students Social distancing must be followed and desks must be spaced apart. There is no reason to sit so close to each other (64).
Respondents highlighted the need for greater student awareness in infection control. There was also a need for the development of protocols for the use of PPE and for hand sanitization processes. These protocols should be supported by regular monitoring to ensure student compliance.
Correct use of PPE and the correct handwashing procedures and also disinfecting the working surfaces (69).
Surprisingly, respondents also highlighted the need for students to reflect on the traditional peer learning support practices.Ensure that everyone sanitize regularly and do not borrow [items] such as pens, books (15)
DISCUSSION
The study findings suggested inconsistencies in study participants' knowledge and attitudes towards infection control in the undergraduate training programmes. About 18 second and 16 third year students expressed fear of working with dental patients in the clinic while 19 first year students did not see this as a challenge. Study participants in the first (21.5%) and second year (14.9) believed that personal protective gear (gloves, masks, scrubs, eye wear) was sufficient to protect them from COVID-19, yet 15 third year students (14%) were unsure or disagreed with the statement (n=16, 14,9%). These inconsistencies in responses are not unusual. Students' perspectives on infection control and susceptibility to infection would be dependent on their year of study and exposure to clinical training. The undergraduate training programme is structured as such that clinical training only occurs in the second and final years hence students in the first year would not have had much exposure to the clinical environment. However, this study findings were in contrast to those reported by Ebrahimpour et al. The authors contended that students' level of infection control knowledge and practice across the different years of study was the same.18 While the findings reported by Halboub et al. support this study findings in terms of inconsistency in students' perspectives on infection control in relation to their academic year of study, it was interesting to note that the authors reported that a 'higher percentage of 5th-year students (58.9%) showed positive attitudes toward the treatment of patients with infectious diseases, as compared to only 31.0% of 4th year students'.19:15 It is however, equally important to note that these studies were conducted pre-COVID-19 and that the findings of this study should be contextualized within the current COVID-19 pandemic. COVID-19 has shown that individual susceptibility to infection increases with close physical contact.20 Thus, final year students perceived a greater level of vulnerability to COVID-19 infections in this study, than students in the lower academic years, given their exposure in the clinical environment.
The majority of participants (Year 1: n=24, 22.5%; Year 2: n=28, 26.2%; Year 3: 22, 31.2%) disagreed that younger people were less susceptible to contracting COVID-19 disease. This implied that study participants believed that they were indeed susceptible to the disease. This finding is supported by other studies that outlined the demographic shifts in the COVID-19 pandemic and suggested that younger people are not only susceptible to contracting the disease but that their health-related behaviors could be driving the pandemic.21-22
While almost all participants (n=105, 98.1%) reiterated the importance of handwashing and sanitization, about 17 first year students (15.9%) indicated that the laboratory coats were washed once a week. Again, this response could be attributed to first year students not being in a clinical setting, therefore washing of lab coats was not seen as a priority in infection control measures. However, these findings are supported by other studies where students reported changing their lab coats only where there were visible signs of contamination such as blood splatter.19,23
The availability of appropriate resources for optimal infection control was also seen as a critical component for learning. Study participants highlighted the need for increased availability as well as better quality of personal protective equipment (PPE) and more hand sanitization stations. Study participants expressed dissatisfaction in having to use the same PPE for a week or more. The availability of appropriate PPE, including face masks remains a global challenge that is further exacerbated in resource constrained clinical teaching and learning environments. Blignaut, Nemutandani and Samaranayake advocate for innovative practice when confronted with shortages in PPE for dental clinical practice. These could include local fabrication of face shields and use of plastic disposal aprons worn over the gowns.24 Additionally, this study findings imply that the impact of limited access to PPE, could contribute to students' fear and anxiety of working in the clinical environment. This finding is consistent with other reports that highlight a correlation between limitations in access to PPE and fear and anxiety among dental health workers,24-25 and dental students are no exception.
The study findings iterate the need for better coordination in clinical training so as to optimize students' health and safety in clinical training. These included the need for social distancing measures, regular temperature checks, and reminders for handwashing or hand sanitization. Other reported recommendations included better ventilation in the clinic, and repair of non-functioning dental clinical units coupled with small groups of students for clinical rotation. These findings are supported by a number of studies that highlight the need to review current dental clinical practice in the context of the COVID-19 pandemic.26-28
Study participants also highlighted the need for optimal infection control practices for class-room based learning. While universal entry screening for university students and staff is critical, other mitigation measures such availability of COVID-19 vaccines, increased physical spacing/social distancing in classrooms, mandatory wearing of face masks, cough etiquette and avoidance of crowding, are equally important to curb the spread of COVID-19 infections.29 This reiterates that universal precautions for infection control needs to extend beyond the clinical settings and that all other aspects of the learning environment must take these measures into consideration. Study participants also highlighted the need for ongoing training in infection control and the availability of standard protocols for wearing of personal protective equipment. This finding is supported by another study that highlights the need for comprehensive strategies for regular infection control monitoring to ensure student compliance.30
Although this study was conducted on a single site, some interesting insights have emerged. The study findings overall highlight the need to engage actively with students, specifically in relation to their perceived needs and demands in undergraduate training. Hence the student becomes a stakeholder in curriculum review and development, and not merely a passive recipient of knowledge and skills acquisition. Such inclusive decision-making processes could address issues such as limited access to PPE in resource-constrained learning settings and students can be given the opportunity to engage in innovative measures to ensure sustained learning where possible during the pandemic.
Limitations of the study
Despite these valuable insights, several limitations were noted. Given that the study was conducted on a single training site, its generalizability was limited to the research site. There could have been over-reporting of data and the responses might not be a true reflection of students' attitudes and compliance in infection control.31 Despite these limitations, the study does provide pertinent data to understand students' perspectives in infection control and the measures needed to mitigate transmission of COVID-19 infections in dental undergraduate training.
CONCLUSION
There was general agreement among study participants that infection control practices such as handwashing and sanitization occurred regularly. However, there were inconsistencies in participants' knowledge and attitudes towards infection control that could have been influenced by the year of academic study. There is a need for ongoing awareness in infection control and general health and safety practices in both clinical and class-room based learning that should extend beyond the COVID-19 pandemic.
Clinical Relevance
Standard precautions (regular hand hygiene, use of face masks and respiratory hygiene) in infection control and other public health measures (such as social distancing and regular temperature checks) should be important considerations for both clinical and classroom-based learning.
REFERENCES
1. Cleveland JL, Bonito AJ, Corley TJ, Foster M, Barker L, Gordon Brown G, Lenfestey N, Lux L. Advancing infection control in dental care settings: factors associated with dentists' implementation of guidelines from the Centers for Disease Control and Prevention. J Am Dent Assoc. 2012 Oct;143(10):1127-38. doi: 10.14219/jada.archive.2012.0044. Erratum in: J Am Dent Assoc. 2012 Dec;143(12):1289. [ Links ]
2. Ghai S. Are dental schools adequately preparing dental students to face outbreaks of infectious diseases such as COVID-19? J Dent Educ. 2020 Jun;84(6):631-633. doi: 10.1002/jdd.12174. [ Links ]
3. Coleman DC, O'Donnell MJ, Shore AC, Russell RJ. Biofilm problems in dental unit water systems and its practical control. J Appl Microbiol. 2009 May;106(5):1424-37 [ Links ]
4. Weinstein RA, Bridges CB, Kuehnert MJ, Hall CB. Transmission of Influenza: Implications for Control in Health Care Settings. Clin Infect Dis [Internet]. 2003;37(8):1094-101. Available from: https://academic.oup.com/cid/article-lookup/doi/10.1086/378292 [ Links ]
5. Garner JS. Guideline for isolation precautions in hospitals. The Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol [Internet]. 1996 Jan;17(1):53-80. Available from: http://www.ncbi.nlm.nih.gov/pubmed/8789689 [ Links ]
6. Kohn WG, Amy S. Collins AS,, Cleveland JL., Harte JA., Eklund KL, Malvitz DM. Guidelines for Infection Control in Dental Health-Care Settings. 2003. December 19/ 52(RR17);1-61. https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5217a1.htm PMID: 14685139 [ Links ]
7. Centers for Disease Control and Prevention. Summary of Infection Prevention Practices in Dental Settings: Basic Expectations for Safe Care. Atlanta, GA: Centers for Disease Control and Prevention, US Dept of Health and Human Services; October 2016. [ Links ]
8. Bastani, P., Mohammadpour, M., Ghanbarzadegan, A. et al. Global concerns of dental and oral health workers during COVID-19 outbreak: a scope study on the concerns and the coping strategies. Syst Rev, 2021, 10, 45. https://doi.org/10.1186/s13643-020-01574-5 [ Links ]
9. Yusoff MSB, Hadie SNH, Mohamad I, et al. Sustainable Medical Teaching and Learning During the COVID-19 Pandemic: Surviving the New Normal. Malays J Med Sci. 2020;27(3):137-142. doi:10.21315/mjms2020.27.3.14 [ Links ]
10. Chang T., Hong G., Paganelli C., Phantumvanit P., Chang W,, Shieh Y., Hsu M. Innovation of dental education during COVID-19 pandemic, Journal of Dental Sciences, 2021,16(1): 15-20. https://doi.org/10.1016/j.jds.2020.07.011. [ Links ]
11. Amir, L.R., Tanti, I., Maharani, D.A. et al. Student perspective of classroom and distance learning during COVID-19 pandemic in the undergraduate dental study program Universitas Indonesia. BMC Med Educ 2020,20, 392. https://doi.org/10.1186/s12909-020-02312-0 [ Links ]
12. Generali L., Iani C., Macaluso GM., Montebugnoli L., Siciliani G., Consolo U. The perceived impact of the COVID-19 pandemic on dental undergraduate students in the Italian region of Emilia-Romagna. European Journal of Dental Education. Dec. 2020. Available at: https://doi.org/10.1111/eje.12640 [ Links ]
13. Grossman S, Sandhu P., Sproat C., PateL V. Provision of dental services at a single institution in the UK's epicentre during the COVID-19 pandemic. British Dental Journal, 2020, 228 (12): 964-70. [ Links ]
14. Banakar, M., Bagheri Lankarani, K., Jafarpour, D. et al. COVID-19 transmission risk and protective protocols in dentistry: a systematic review. BMC Oral Health 2020, 20, 275 https://doi.org/10.1186/s12903-020-01270-9 [ Links ]
15. 15. Petersen PE. Continuous improvement of oral health in the 21st century-the approach of the WHO Global Oral Health Programme. 2003. [ Links ]
16. Singh S. Can undergraduate student learning in prevention influence oral health self-care practices? - a report from a South African University. International Journal of Dental Hygiene, 2016;15(4) DOI: 10.1111/idh.12235 [ Links ]
17. Moodley R, Singh S, Moodley I. Dental undergraduate students' perspectives on teaching and learning during the Covid-19 pandemic -a report from a South African university. 2021. Submitted to African Journal for Health Professions Education. In review. [ Links ]
18. Ebrahimpour A., Pakravan A.H., Nezhad M.Y., Alipour N., Saravi M.E., Rahbar F., Khatam Z.S. Knowledge and performance of dental students with regard to infection control guidelines in Dental School of Mazandaran University of Medical Sciences in 2015. International Journal of Medical Research & Health Sciences, 2016, 5, 8:298-304. Available at: https://www.ijmrhs.com/medical-research/knowledge-and-performance-of-dental-students-with-regard-to-infection-control-guidelines-in-dental-school-of-mazandaran-.pdf [ Links ]
19. Halboub ES, Al-Maweri SA, Al-Jamaei AA, Tarakji B, Al-Soneidar WA. Knowledge, attitudes, and practice of infection control among Dental Students at Sana'a University, Yemen. J Int Oral Health 2015;7(5):15-19. [ Links ]
20. World Health Organization 2020. Transmission of SARS-CoV-2: implications for infection prevention precautions. Scientific Brief. 9 July 2020. Available at https://www.who.int/news-room/commentaries/detail/transmission-of-sars-cov-2-implications-for-infection-prevention-precautions [ Links ]
21. Monod M., Blenkinsop A., Xi X, Hebert D., Bershan S., Tietze S. et. al. Age groups that sustain resurging COVID-19 epidemics in the United States. Science., 02 Feb 2021:eabe8372. DOI: 10.1126/science. abe8372. Available at: https://science.sciencemag.org/content/early/2021/02/01/science.abe8372 [ Links ]
22. Abbasi J. Younger Adults Caught in COVID-19 Crosshairs as Demographics Shift. JAMA. 2020;324(21):2141-2143. doi:10.1001/jama.2020.21913 [ Links ]
23. Rahman B, Abraham SB, Alsalami AM, Alkhaja FE, Najem SI. Attitudes and practices of infection control among senior dental students at college of dentistry, university of Sharjah in the United Arab Emirates. Eur J Dent 2013;7 Suppl 1:S15-9. [ Links ]
24. Blignaut E, Nemutandani S., Samaranayake L. Strategic implementation of dental infection control in resource-poor jurisdictions during COVID-19 pandemic: a perspective from South Africa, Acta Odontologica Scandinavica, 2020, 78:8, 614-617, DOI: 10.1080/00016357.2020.1804073 [ Links ]
25. Chersich MF, Gray G, Fairlie L, et al. COVID-19 in Africa: care and protection for frontline healthcare workers. Global Health. 2020; 16(1):46. [ Links ]
26. Bizzoca ME. Campisi G., Muzio LL. Covid-19 Pandemic: What Changes for Dentists and Oral Medicine Experts? A narrative review and novel approaches to infection containment. Int. J. Environ. Res. Public Health 2020, 17, 3793; doi:10.3390/ijerph17113793 [ Links ]
27. Amato A., Caggiano M., Amato M., Moccia G., Capunzo M., De Caro F. Infection Control in Dental Practice During the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 4769. http://dx.doi.org/10.3390/ijerph17134769 [ Links ]
28. Meng L., Hua F., Bian Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. Journal of Dental Research 00(0), 2020: 1-7. Available at: https://doi.org/10.1177/0022034520914246 [ Links ]
29. Walke HT, Honein MA, Redfield RR. Preventing and Responding to COVID-19 on College Campuses. JAMA, 2020;324(17):1727-1728. Doi:10.1001/jama.2020.20027 [ Links ]
30. AL-Essa N.A., AlMutairi M.A. To what extent do dental students comply with infection control practices? The Saudi Journal for Dental Research, 2017, 8 (1-2): 67-72. Available: https://doi.org/10.1016/j.sjdr.2016.10.003 [ Links ]
31. Alharbi, G., Shono, N., Alballaa, L. et al. Knowledge, attitude and compliance of infection control guidelines among dental faculty members and students in KSU. BMC Oral Health, 2019,19(1).1-18 https://doi.org/10.1186/s12903-018-0706-0 [ Links ]
 Correspondence:
Correspondence:
Shenuka Singh
School of Health Sciences, Discipline of Dentistry, University of KwaZulu-Natal
Private Bag X54001, Durban, 4001, South Africa
Email: singhshen@ukzn.ac.za
Author contributions:
1 . Shenuka Singh: 60%
2 . Rajeshree Moodley: 25%
3 . Ilana Moodley: 15%


{kind=link}