










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.77 n.6 Johannesburg Jul. 2022
http://dx.doi.org/10.17159/2519-0105/2022/v77no6a5
RESEARCH
The Practice of Oral Medicine in South Africa
J FourieI; A MasengeII
IBChD, DipOdont(Perio), DipOdont(Rest), MSc(Odont), MChD, Department of Periodontics and Oral Medicine, School of Dentistry, Faculty of Health Sciences, University of Pretoria. ORCID: 0000-0002-8674-8145
IIMSc (Statistics) Senior Research Consultant. Department of Statistics, University of Pretoria, Hatfield campus, ORCID : 0000-0001-8372-2356
ABSTRACT
INTRODUCTION: Oral medicine is a clinical discipline, practiced by periodontists, which concerns itself mostly with the nonsurgical management of oral mucosal diseases. Many of these diseases are rare and the discipline less well known - making it essential to identify the obstacles this discipline faces
AIMS AND OBJECTIVES: The purpose of this study was to describe the private and academic practice of Oral Medicine
DESIGN AND METHODS: A self-administered, internet-based, questionnaire was distributed to South African periodontists which questioned the clinician's competency, diseases managed, special investigations performed, referral sources, proportional time and monetary distribution of the discipline, and perceived barriers to the practice
RESULTS: Twenty-six periodontists completed the questionnaire. In comparison to periodontology and implantology, periodontists generally feel less competent, spend less time on, and receive less money from Oral Medicine. Lack of awareness of the speciality (55.6% - 59.3%) was identified as the biggest constraint, with only 11.2% of referrals received from medical doctors. Immune-mediated diseases (29.3%) and benign neoplasms (26.5%) are managed the most, and surgical biopsies (80.2%) are used most regularly to diagnose oral mucosal disease
CONCLUSION: Oral Medicine is still a lesser-known clinical speciality. Despite the heavy burden of HIV-related oral disease and oral mucosal malignancies, this speciality remains underutilised
Keywords: oral medicine, oral mucosal disease, special investigations, scope of practice
INTRODUCTION
There Is currently no available data that describes the clinical practice of Oral Medicine (OM) In South Africa. Because OM is a less well-known dental speciality, among both dental and medical practitioners as well as the public, the service remains incompletely utilised,1,2 even though many healthcare practitioners feel that the diagnosis and management of oral diseases fall outside their scope of practice.3 The speciality shares its clinical domain with other medical and dental disciplines, but appropriate referrals are necessary to reduce treatment cost and time while improving patient care.3 In addition, while the clinical competencies of the OM clinician have been delineated by the HPCSA, it is necessary to mirror these competencies with the clinical practice of OM in real life.
It is important to establish the current state of affairs of OM in private practice and academia so that recommendations can be made regarding the future of OM, in terms of training, treatment, collaboration, continuous skill development, research, and service provision. This should ultimately culminate in an improved service that is rendered to patients with oral mucosal disease.
Oral medicine is a relatively young, and somewhat unknown,1 speciality with varying definitions and recognition across the globe. In the United Kingdom, it is defined as 'the speciality of dentistry concerned with the oral health of patients with chronic, recurrent and medically-related disorders of the oral and maxillofacial region, and with their diagnosis and nonsurgical management'4 while in the USA it is considered as 'the speciality of dentistry concerned with the oral healthcare of medically complex patients and with the diagnosis and non-surgical management of medically-related disorders or conditions affecting the oral mucosa'.5 The common denominator seems to be the 'diagnosis and non-surgical management of medically related disorders' but differs in terms of the treatment of medically complex patients. The HPCSA stipulates that: "The scope of expertise of the specialist in Oral Medicine and Periodontics includes the diagnosis and management of diseases, disorders and anomalies that affect the oral and periodontal tissues, as well as the oral and peri-oral manifestations of systemic diseases according to evidence-based practices".
The VIth World Workshop in Oral Medicine has recently validated core clinical competencies in OM through the contributions of 31 different countries.7 South Africa has largely adapted these competencies but has excluded those involving temporomandibular disorders and behavioural and mental health.
The major competencies subsequently include the examination and diagnosis of oral mucosal disease through careful history taking, clinical examination, and special investigations; as well as the effective pharmacological and surgical management of localised benign disease in which surgical biopsies are employed to establish a diagnosis of disease. Diseases of an immune-mediated, developmental, genetic, or infective basis, as well as salivary gland disorders, orofacial pain, and the oral presentation of systemic diseases, are included in the scope of practice of the OM specialist.
Despite the American Association of Oral Medicine being established 75 years ago, it was only in 2020 that it received recognition as a speciality.5 While in Europe, although OM can be considered as a distinct field of study in several countries, it is only registered as a speciality in the UK, Croatia and Israel, while elsewhere it is combined with other disciplines'6 A similar sentiment is shared in South Africa where the speciality is combined with periodontics to culminate in the "Periodontics and Oral Medicine" degree.
Currently, it is unknown what the demand for OM services is, and whether the professional services of OM clinicians are fully utilised by health care workers8 and the general public. If the service is not well known, general clinicians may resort to either inappropriate diagnostic and therapeutic strategies of conditions that they are unfamiliar with,3 or inappropriate referrals.1,2 It is therefore important to assess referral and treatment patterns of OM-related complaints to most effectively structure the delivery of these services, workforce planning, and hospital, academic, and government funding policy.
This study will therefore attempt to shed some light on OM practice in South Africa. It will seek to identify what proportion of their time periodontists spend on OM, who their referral base is, which diseases are most commonly managed and whether it is financially rewarding given the fact that OM is mostly considered as a part-time practice by specialists in academic institutions.8 Hopefully, the results can be used to inform future decision-making regarding the dental training curriculum, expected clinical competencies of trainee periodontists, and support future collaboration with other clinical disciplines.
MATERIALS AND METHODS
This was a cross-sectional, descriptive study that describes the practice of OM in SA through a self-administered, internet-based, questionnaire.
The study was conducted among a population of HPCSA registered periodontists in South Africa. An email, with the invitation to participate in the study and an informed consent form, was distributed by the South African Society for Periodontology, Implantology and Oral Medicine. A personal follow-up email was sent to each member with another invitation to participate.
The survey was distributed as an electronic link powered by the Qualtrics XM survey platform. It consisted of 16 questions. Questions ranged from multiple response questions, yes/no answers, using a sliding scale to give proportionate agreement/disagreement answers, as well as a single open-ended question. Respondents were asked how long they had been in practice, where they qualified, type of clinical practice (academia, private, public), whether they render OM services and which factors they perceive as barriers to OM practice. In addition, they had to use a rating scale to proportionally portray their OM practice in terms of time spent, money earned, referral sources, variety and frequency of diseases treated, special investigations ordered; and self-perceived clinical competency.
Participation was completely voluntary and the survey response was anonymous. Respondents gave consent by agreeing to participate in the study and the results could by no means be traced back to a respondent. Ethics approval was obtained from the University of Pretoria, Faculty of Health Sciences, Research Ethics Committee (366/2021).
Data were analysed with IBM SPSS Statistics version 27 (1989,2020). Descriptive statistics using frequencies (counts and percentages) was performed for categorical variables and means, medians, standard deviations, and 95% confidence intervals were performed for continuous variables. A total sampling method was applied whereby all registered periodontists were invited to participate in the study.
RESULTS
Demographics of study participants
Twenty-seven periodontists agreed to participate in the study, but only 26 completed the questionnaire, resulting in a 47.2% response rate, given that the invitation was emailed to 55 periodontists. Yet, not all questions were answered by all respondents, and neither were all the questions relevant to all clinicians. Two periodontists were in their first year of clinical practice, while one had been in practice for 46 years. The greatest number of respondents (n = 7) had been in practice for 3 years (26.9%), and 18 (69.2%) had been in practice for 13 years or less. The greatest proportion of respondents had qualified from the University of Pretoria (n = 10, 38.5%), eight (30.8%) from the University of the Western Cape, and five (19.2%) from Sefako Makgatho Health Sciences University (SMU), also previously known as Medunsa or the University of Limpopo.
Description of clinical practice
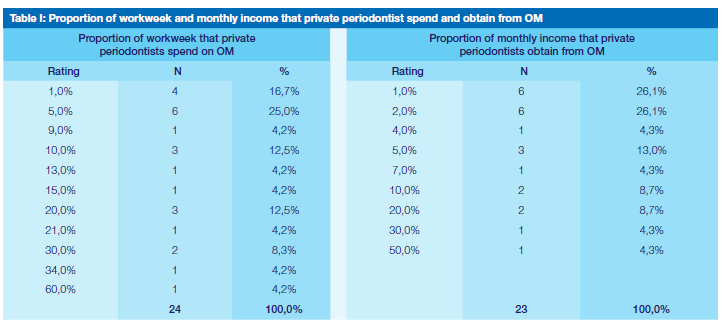
There was an equal distribution between periodontists that are in full-time private practice and those that have some academic involvement (n = 11, 40.7%). All of the periodontists practice oral medicine, either as part of their private or academic practice. In private practice, four (16.7%) periodontists spend 1% of their workweek on OM, 6 (25%) spend 5% of their workweek on OM and only 1 (4.2%) spend 60% of the workweek on OM. In total, 95.8% spend 34% or less time per week on OM. Six periodontists said that OM contributes only 1% to their practice turnover, while 82.6% said it contributes less than 10% to their practice turnover. Only one (4.3%) periodontist generates 50% of his/her income from OM (Table I). On average, periodontists spend 14% of their time on OM and 8% of their monthly income comes from OM. Twenty-nine percent of periodontists collaborate in multidisciplinary clinics to manage complex oral mucosal diseases.
Self-perceived competency and constraints that periodontists experience in their OM practice:
Periodontist could present their self-perceived competency in the different clinical disciplines of the speciality on a sliding percentage scale:
• Periodontology: 10 (38.5%) of periodontists scored their self-perceived competency in periodontology as 80% (also the greatest number of periodontists on a single score), and 5 (19.2%) scored themselves at a 100%. The lowest score was 70% which only one periodontist scored him/herself. Only 2 (7.7%) scored themselves less than 80% competent in periodontology.
• Oral Medicine: 5 (19.2%) of periodontists scored their self-perceived competency in OM as 50%, which was also the lowest mark given and the greatest total number of periodontists on a single score. Four periodontists (15.4%) scored themselves as 100% competent, while 11 (61.5%) periodontists scored themselves less than 80% competent in OM.
• Implantology: 2 (7.7%) scored themselves at 60% (lowest mark), 5 (19.2%) scored themselves at 100% and 7 (26.9%) felt they were less than 80% competent. The greatest number of periodontists on a single score was 6 (23.1%) who scored themselves 80% (Table II).
• On average, periodontists scored themselves as 85.3%, 83.8%, and 74.2% competent in periodontology, implantology, and oral medicine respectively.
The greatest constraint to a successful OM practice, as perceived by the respondents, is the lack of awareness of the speciality by both the general public (55.6%), general dental practitioners (51.9%), and medical practitioners (59.3%). Although lack of patient finances (7.4%) was not considered a significant constraint, the fee structure of OM-related procedures (40.7%) was. The lack of continuous professional development opportunities in OM (48.1%) was identified as another significant constraint to a successful OM practice (Table III).
Sources of OM referrals in private and academic practice:
For private OM clinics, 85% of referrals come from general clinicians and only 15% from other specialities. Dental clinicians are the most frequent sources of referrals; 73.8% and 9.8% among general and specialist clinicians respectively (Table IV). In the academic environment, most referrals (64.3%) come from other academic departments in both the dental and associated medical school.
Twenty-one percent of referrals come from private clinicians, and other public clinics contribute 14.5% of the referrals. Yet, referrals from medical healthcare workers only contribute a small fraction: 8.6% from academic medical departments, 1.5% from private, and 3.9% from public clinics (Table V).
Frequency of oral mucosal lesions and conditions seen in OM practice:
Respondents estimated that immune-mediated diseases such as oral lichen planus, mucous membrane pemphigoid, pemphigus vulgaris, recurrent aphthae, and erythema multiforme are seen the most frequently (29.3%), followed by benign reactive neoplasms (26.5%). These would include lesions such as traumatic fibroma, fibrous epulis, pyogenic granuloma, etc. Chemosensory disorders, such as altered taste perception, account for only 1.5%, and oral mucosal disease as the presentation of systemic disease, only 2.5% of lesions and conditions (VI).
Frequency of special investigations performed in OM practice:
Surgical biopsies were the most commonly performed special investigation (80.2%), and as part of this investigation, direct-immunofluorescence was regularly performed (23%). The next most commonly performed special investigation was serology (20.2%), followed by radiographic assessments. Allergy testing was performed the least (5.2%) followed by the use of adjunctive diagnostic aids, such as the VELscope and Toluidine Blue (5.7%) (VII).
The proportion of time spent on different aspects of Oral Medicine in academia:
When the respondents only considered the amount of time they spent on different aspects of OM in academic practice. They spent the most time training postgraduate students in OM (41.4%), and the least amount of time on research (2.3%) and undergraduate training (6.1%) (Table VIII).
DISCUSSION
A 47.2% response rate was achieved in this study, which falls slightly short of the target of 60%. The 52.8% of periodontists who did not complete the questionnaire, introduce a degree of nonresponse bias which reduces the validity and reliability of this study.9 Multimode approaches, such as another SMS or Whatsapp communication, may have improved this response rate.9 It is possible that clinicians who are not interested in OM, naturally, opt-out of research on this topic. From the response rate to questions that only focused on the academic aspect of OM, and by deducing the number of periodontists that are known to be in academia, it seems that the larger proportion of non-respondents is in full-time private practice. The respondents of this study were equally weighed between full-time private practice and those that have some academic involvement. But a survey among OM specialists in 40 different countries, found that most clinicians practice in hospitals and dental schools and that private practice was less commonly utilised.8 However, in South Africa, because of the combined clinical practice of periodontology and implantology, private practice is a feasible option for many periodontists.
It seems that OM is the neglected stepchild of many periodontists, which only occupies 14% of the average workweek, and only contributes 8% to the monthly income. It can be argued that the lower self-perceived competency that periodontists have in OM, as opposed to their other clinical disciplines, is either the result or the cause of the above figures. However, periodontists largely attribute it to a lack of awareness of this sub-speciality among the general public and other healthcare workers. In addition, the low fee structure of OM-related treatment codes reflects the mismatch between time spent and money earned in this discipline. Lastly, there are extensive, local, and international, continuous development opportunities in periodontology and implantology, but hardly any in OM. Conferences and training opportunities in these disciplines are sponsored by manufacturers, but because OM is not a revenue-generating source to large companies, this type of sponsorship, and hence, continuous professional development in OM, is sorely lacking in South Africa.
Private periodontists receive most of their referrals from general dentists. This may sound like a paradox because the lack of awareness of this speciality among general dentists was also considered one of the largest constraints. Yet this phenomenon is mirrored in the literature: while dentists may be the largest referral source to an OM practice,3,10-13 very few dentists make use of an OM service.10 Implying that it is a small group of general dentists that notice and refer the bulk of oral mucosal disease.
Other studies which have assessed OM referral practices were predominantly hospital-based.3,10-14 From these studies, it was only Villa et al., 2015, who conducted their study in a medical hospital, that found most referrals come from medical practitioners.14 Given the high prevalence of common oral mucosal diseases and lesions,15-18 it is possible that dentists either manage these patients themselves, refer to other disciplines, or not notice these lesions. Yet, when general clinicians do refer patients, it is seldom accompanied with a diagnosis,12,14 and when a diagnosis is offered, it is mostly incorrect.13 In addition, most healthcare workers feel that the management of oral diseases falls outside their scope of practice and that OM is a clinical competency that is hard to maintain in clinical practice because many of the diseases present too infrequently.3 Given the fact that only 6.1% of OM dedicated academic time is spent on the training of undergraduate students, we need to reconsider our dental curricula so that the clinician responsible for the management of oral diseases, and to whom a referral should be directed, stands front and center in the training of dentists.
Patients with oral mucosal disease are just as likely to consult with a medical doctor, than with a dentist.17 Yet, only 16.5% and 14% of referrals in this study came from medical doctors in private and academic clinics respectively. The lack of referrals from medical practitioners implies that they are more likely to refer to a medical colleague, such as an otolaryngologist,18 or a more well-known dental specialty, such as maxillofacial and oral surgery, or a dental colleague. Only a few medical practitioners are aware of OM specialist services.19 This can be improved by greater involvement in multidisciplinary clinics, in which only 29.2% of South African periodontists are involved, as opposed to our international counterparts (50%).8
The fact that OM is so poorly known, and perhaps hidden to a degree within other specialties, can result in patients seeing multiple clinicians,1,2 where inappropriate tests are ordered and ineffective therapy is provided, before the eventual referral to an OM specialist.20 This results in an unnecessary escalation of health care costs and patient morbidity. Because OM is such a poorly known speciality among the general public,1 patients are unlikely to self-refer and may be obstructed by the archaic principle which requires a general clinician referral to a specialist clinician. Given the fact that OM often involves chronic, painful, and even life-threatening oral mucosal conditions21 with a significant impact on the quality of life of the affected individual, the need to provide effective and expedited care cannot be overemphasised. The demand for OM services in other countries has been well established1,17 and should reasonably be transferrable to South Africa. Yet, the ability to match service provision to demand should be elucidated.
An international survey of oral medicine practice conducted by the Vth World Workshop in Oral Medicine in 2011 described the status of OM practice amongst 40 different countries (not including South Africa). The definition of OM varied between different countries, mostly concerning general dental care provided to medically complex patients, chemosensory disorders, and orofacial problems in patients with physical and mental disabilities.8 Although the South African periodontist may need to manage periodontal and oral mucosal complaints of medically complex patients or patients with mental and physical disabilities, the provision of general dental care to this population is not part of the HPCSA defined scope of practice. Chemosensory disorders, though not explicitly specified in the scope of practice, are hardly ever managed by our study population (1.5%).
The spectrum of oral diseases treated by South African OM specialists matches the common scope of practice in other countries, and those stipulated by the HPCSA, which includes the management of oral mucosal diseases, salivary dysfunction, oral manifestations of skin disorders, HIV, gastrointestinal, rheumatic disease and facial pain. In the study by Stoopler et al., respondents indicated that their patient populations mostly consisted of patients with oral mucosal lesions but facial pain and the oral presentation of skin disorders were also well represented.8
In South Africa, OM specialists treat immune-mediated diseases, which can also be described as the oral presentation of skin disorders, most frequently, followed by benign, reactive, neoplasms. Although infections are managed the third most commonly, the low frequency at which it is managed (10.2%) contradicts the common misperception that infections of the oral mucosa are exceedingly common. Although the frequency with which periodontists manage diseases certainly cannot be extrapolated to the overall prevalence of a disease, it merely demonstrates the focus of a clinician's practice. Yet, it is surprising to see that HIV-associated oral disease is managed the 5th most frequently, and only 7% of the time. This is even though STATS SA estimates that 13.7% of the South African population is infected with HIV in 202122 and that more than a third of these patients are expected to present with oral manifestations.23 Managed only slightly more frequently were potentially malignant disorders and malignancies of the oral mucosa. A recent meta-analysis calculated the worldwide prevalence of oral potentially malignant disorders as 4.47%,24 which of course differs among populations according to the varied exposure to risk factors. While the WHO reported 1933 new lip- and oral cancer cases, and a resultant 814 deaths in 2020 in Southern Africa, it does seem that periodontists are an underutilised resource in the management of these conditions.25
In this study, periodontists used surgical biopsies and subsequent direct immunofluorescence (DIF) staining, most frequently in the assessment and management of oral mucosal disease. The frequent use of DIF corresponds to the regular management of immunemediated diseases as well as the close relationship these participants have with academic pathology laboratories where these facilities are more readily available. Surgical biopsy of oral mucosal lesions, and the subsequent histopathological examination, remains the gold standard in the assessment of oral mucosal disease.26 And while conventional exfoliative cytology is often employed in the diagnosis of oral candidiasis, the clinical appearance, combined with an accurate history, is often sufficient to reach a diagnosis.27 When it does become necessary to distinguish between different Candida strains, as in the immunocompromised host who shows resistance to therapy, conventional histopathological assessment of a smear will be insufficient.28 More reliable techniques, such as microbiological culture with sensitivity testing may then become necessary.29 The low frequency at which oral mucosal infections are managed by periodontists (10.2%), matches the equally low frequency at which exfoliative cytology (9.2%) and microbiological culture (12.1%) are used.
Brush biopsies and adjunctive diagnostic aids, such as the VELscope and Toluidine Blue, are frequently used in the assessment of potentially malignant disorders. While the sensitivity and specificity of a brush biopsy have been improved by the use of a cytobrush and liquid-based cytology, further advances such as computer-assisted-, DNA-, molecular- and immunocytochemical analysis that can further improve the reliability of this investigation,30 are still not used routinely in South Africa. It is therefore unlikely that a brush biopsy will replace a surgical biopsy to reach a definitive diagnosis of OPMD or OSCC, it is helpful in the assessment of doubtful lesions and the monitoring of OPMD.30 It is encouraging to see that the adjunctive diagnostic aids are being used by the specialists who are best suited to interpret their results.31
OM specialists working in academia are primarily tasked with the training of post-graduate students (41.1%), followed by administration (28.8%) and patient treatment (21.7%), only 2.3% of their time is spent on research. While internationally, the most time is spent on patient care, followed by administration, teaching, and also, lastly, on research.8
This study attempted to address some of the shortcomings that Stoopler et al. 2011, identified in their study. Namely, to establish referral sources and the financial viability of an OM practice. They also recommended that future research should assess the potential of OM as "a full-time clinical practice, rather than chiefly a part-time practice by specialists in academic institutions".8 But, through the words of one study respondent, unfortunately, "Oral Medicine is not a viable component to sustain private practice".
CONCLUSION
Therefore, we should develop strategies to expand the awareness of OM among patients, dentists, and our medical colleagues. We can only hope to achieve this through focused collaboration in the training of healthcare workers, and the management of our shared patients. OM-related research and local publications should further improve the visibility of this speciality among clinicians.
Ethics approval
Ethics approval was obtained from the University of Pretoria, Faculty of Health Sciences, Research Ethics Committee (366/2021).
Conflict of interest
None.
REFERENCES
1. Miller CS, Hall EH, Falace DA, Jacobson JJ, Lederman DA, Segelman AE. Need and demand for oral medicine services in 1996. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontology. 1997 Dec;84(6):630-4. [ Links ]
2. Haberland CM, Allen CM, Beck FM. Referral patterns, lesion prevalence, and patient care parameters in a clinical oral pathology practice. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999 May;87(5):583-8. [ Links ]
3. Farah CS, Simanovic B, Savage NW. Scope of practice, referral patterns and lesion occurrence of an oral medicine service in Australia. Oral Dis. 2008;14(4):367-75. [ Links ]
4. British Society for Oral Medicine Constitution (2018) [Internet]. British & Irish Society for Oral Medicine. 2018 [cited 2020 Oct 27]. Available from: https://bisom.org.uk/british-society-for-oral-medicine-constitution-2018/ [ Links ]
5. Press Release: Oral Medicine Is Now an ADA-recognized Dental Specialty [Internet]. [cited 2020 Oct 22]. Available from: https://maaom.memberclicks.net/index.php?option=com_content&view=article&id=588:press-release--oral-medicine-is-now-an-ada-recognized-dental-specialty&catid=21:news&Itemid=285?utm_source=website&utm_medium=homepage&utm_campaign=member-engagement [ Links ]
6. Steele JC, Clark HJ, Hong CHL, Jurge S, Muthukrishnan A, Kerr AR, et al. World Workshop on Oral Medicine VI: an international validation study of clinical competencies for advanced training in oral medicine. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015 Aug;120(2):143-151.e7. [ Links ]
7. Bez C, Sklavounou A, Carrozzo M. Oral medicine in Europe: past, present and future. Br Dent J. 2017 Nov;223(9):726-8. [ Links ]
8. Stoopler ET, Shirlaw P, Arvind M, Russo LL, Bez C, Rossi SD, et al. An international survey of oral medicine practice: Proceedings from the 5th World Workshop in Oral Medicine. Oral Dis. 2011;17(s1):99-104. [ Links ]
9. Fincham JE. Response rates and responsiveness for surveys, standards, and the Journal. Am J Pharm Educ. 2008 Apr 15;72(2):43. [ Links ]
10. Friesen R, McGaw T, Peters E, Lai H. A retrospective analysis of referral patterns to a university oral medicine clinic. Oral Surg Oral Med Oral Pathol Oral Radiol. 2019 Oct;128(4):381-5. [ Links ]
11. Guan G, Lau J, Yew V, U J, Qu W, Lam J, et al. Referrals by general dental practitioners and medical practitioners to oral medicine specialists in New Zealand: a study to develop protocol guidelines. Oral Surg Oral Med Oral Pathol Oral Radiol. 2020 Jul;130(1):43-51.e5. [ Links ]
12. Navarro CM, Onofre MA, Sposto MR. Referral letters in oral medicine: an approach for the general dental practitioner. Int J Oral Maxillofac Surg. 2001 Oct;30(5):448-51. [ Links ]
13. Sardella A, Demarosi F, Lodi G, Canegallo L, Rimondini L, Carrassi A. Accuracy of Referrals to a Specialist Oral Medicine Unit by General Medical and Dental Practitioners and the Educational Implications. J Dent Educ. 2007;71(4):487-91. [ Links ]
14. Villa A, Stock S, Aboalela A, Lerman MA, Woo S-B, Sonis ST, et al. Oral Medicine referrals at a hospital-based practice in the United States. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015 Apr;119(4):423-9. [ Links ]
15. Laronde DM, Williams PM, Hislop TG, Poh C, Ng S, Bajdik C, et al. Influence of fluorescence on screening decisions for oral mucosal lesions in community dental practices. J Oral Pathol Med Off Publ Int Assoc Oral Pathol Am Acad Oral Pathol. 2014 Jan;43(1):7-13. [ Links ]
16. Bhatnagar P, Rai S, Bhatnagar G, Kaur M, Goel S, Prabhat M. Prevalence study of oral mucosal lesions, mucosal variants, and treatment required for patients reporting to a dental school in North India: In accordance with WHO guidelines. J Fam Community Med. 2013;20(1):41-8. [ Links ]
17. Miller CS, Epstein JB, Hall EH, Sirois D. Changing oral care needs in the United States: the continuing need for oral medicine. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001 Jan;91(1):34-44. [ Links ]
18. Shulman JD, Beach MM, Rivera-Hidalgo F. The prevalence of oral mucosal lesions in U.S. adults: data from the Third National Health and Nutrition Examination Survey, 1988-1994. J Am Dent Assoc 1939. 2004 Sep;135(9):1279-86. [ Links ]
19. Jovanovic A, Schulten EAJM, van der Waal I. Referral pattern of patients with oral mucosal lesions in The Netherlands. Community Dent Oral Epidemiol. 1992 Apr;20(2):94-6. [ Links ]
20. Bokkasam V, Raviraj J, Gundlapalle P, Kolugundla V, Vardhan H, Thombarapu L. Awareness of oral medicine specialty among medical practitioners in and around Tirupati: A survey. J Indian Acad Oral Med Radiol. 2015;27(1):59. [ Links ]
21. Scully C, Miller CS, Aguirre Urizar J-M, Alajbeg I, Almeida OPD, Bagan JV, et al. Oral medicine (stomatology) across the globe: birth, growth, and future. Oral Surg Oral Med Oral Pathol Oral Radiol. 2016 Feb;121(2):149-157.e5. 22. http://www.statssa.gov.za/publications/P0302/P03022021.pdf [ Links ]
23. Tappuni AR. The global changing pattern of the oral manifestations of HIV. Oral Dis. 2020 Sep;26 Suppl 1:22-7. [ Links ]
24. Mello FW, Miguel AFP, Dutra KL, Porporatti AL, Warnakulasuriya S, Guerra ENS, et al. Prevalence of oral potentially malignant disorders: A systematic review and meta-analysis. J Oral Pathol Med Off Publ Int Assoc Oral Pathol Am Acad Oral Pathol. 2018 Aug;47(7):633-40. [ Links ]
25. https://gco.iarc.fr/today/data/factsheets/populations/710-south-africa-fact-sheets.pdf [ Links ]
26. Poh CF, Ng S, Berean KW, Williams PM, Rosin MP, Zhang L. Biopsy and histopathologic diagnosis of oral premalignant and malignant lesions. J Can Dent Assoc. 2008 Apr;74(3):283-8. [ Links ]
27. Farah CS, Lynch N, McCullough MJ. Oral fungal infections: an update for the general practitioner. Aust Dent J. 2010 Jun;55 Suppl 1:48-54. [ Links ]
28. Williams DW, Lewis MA. Isolation and identification of Candida from the oral cavity. Oral Dis. 2000 Jan;6(1):3-11. [ Links ]
29. Manfredi M, Polonelli L, Aguirre-Urizar JM, Carrozzo M, McCullough MJ. Urban legends series: oral candidosis. Oral Dis. 2013 Apr;19(3):245-61. [ Links ]
30. Mehrotra R, Hullmann M, Smeets R, Reichert TE, Driemel O. Oral cytology revisited. J Oral Pathol Med. 2009;38(2):161-6. [ Links ]
31. Farah CS, McIntosh L, Georgiou A, McCullough MJ. Efficacy of tissue autofluorescence imaging (VELScope) in the visualization of oral mucosal lesions. Head Neck. 2012 Jun;34(6):856-62. [ Links ]
 Correspondence:
Correspondence:
Jeanine Fourie
Department of Periodontics and Oral Medicine, School of Dentistry, Faculty of Health Sciences, University of Pretoria
Tel: 012 319 2312; Cell: 082 460 8368; Email: jeanine.schaap@up.ac.za
Author contributions:
1. Jeanine Fourie: 80%
2. Andries Masenge: 20%


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}