










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.77 no.5 Johannesburg 2022
http://dx.doi.org/10.17159/2519-0105/2022/v77no5a10
RADIOLOGY CASE
http://dx.doi.org/10.17159/2519-0105/2022/v77no5a10
S NelI; C SmitII
IBChD, MSc (Odontology). Department of Oral Pathology and Oral Biology, University of Pretoria. ORCID: 0000-0002-0802-079X
IIBChD, MSc (Maxillofacial and Oral Radiology). Department of Oral Pathology and Oral Biology, University of Pretoria. ORCID: 0000-0003-4047-6356
CASE
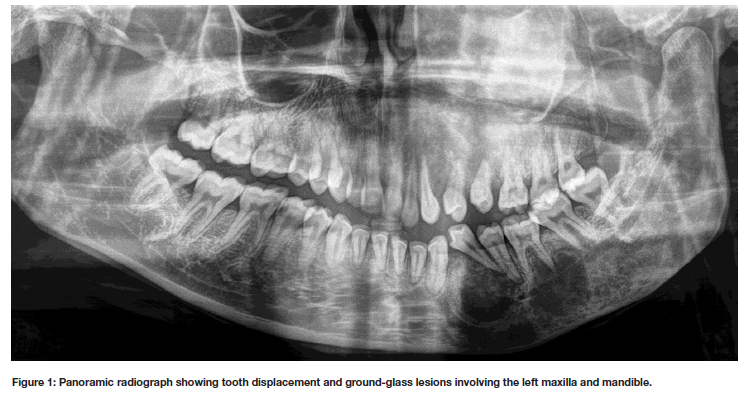
A 23-year-old female patient presented with diffuse swelling causing intermittent pain involving the left side of the face that had been present for over 10 years. Extra-oral examination revealed expansile lesions in the maxilla and mandible, that appeared mixed radiolucent-radiopaque on panoramic radiography. The maxillary lesion resulted in opacification of the maxillary sinus. The left side of the mandible presented with trabecular bony changes and larger radiolucent areas (Figure 1). Cone-beam computed tomography (CBCT) imaging revealed ground-glass opacification and significant expansion involving the majority of the skull bones on the left with selected bones also affected on the right-hand side. The frontal, temporal, parietal, sphenoid, ethmoid, maxillary, zygomatic bones and mandible were all affected (Figure 2).
INTERPRETATION
Fibrous dysplasia (FD) is a rare disorder that results in normal bone being replaced by fibro-osseous tissue.1,2 Post-zygotic substitution mutations of the guanine nucle-otide-binding protein (GNAS) gene is responsible for the development of this disorder.3 Mosaic mutations result in the dysregulated overproduction of cyclic adenosine monophosphate (cAMP) in bone marrow stromal cells, leading to increased proliferation and differentiation of functionally impaired osteoprogenitor cells.4 This leads to weak, deformed bone; prone to fracture. Varying degrees of mosaicism give rise to a wide clinical spectrum that varies between asymptomatic to severe disabling cases.1
FD can present as single lesions (monostotic) where the GNAS mutation occurred in postnatal life. However, if the mutation occurs during embryonic development it can affect multiple bones (polyostotic).4 When the maxilla is affected, it is referred to as craniofacial FD, due to the involvement of numerous close approximated bones. FD commonly affects the maxilla and presents radiologically with expansion and a ground-glass opacification of the affected bone.2
Polyostotic FD occurs in conjunction with extra-skeletal diseases and may be associated with Jaffe-Lichtenstein syndrome, McCune-Albright syndrome, or Mazabraud syndrome. Patients with Jaffe-Lichtenstein syndrome present with additional associated hyperpigmented (café-au-lait) skin lesions.5 McCune-Albright syndrome presents with café-au-lait skin lesions and endocrine disorders (gonadotropin-independent sexual precocity).4 Mazabraud syndrome is characterized by the involvement of intramuscular myxomas.6
In this case, the patient presented with swelling that led to facial asymmetry and tooth displacement as a result of significant expansion of the affected bones. Radiologically, early FD presents as a radiolucent lesion, but over time it develops a homogeneous ground-glass appearance that blends into the surrounding bone.2 These features are highly characteristic of FD and a strong presumptive diagnosis can be made, but ultimately histologic confirmation is required. In polyostotic FD it is important to rule out additional endocrine disorders to optimise patient treatment. Contouring of the affected bone is required in some cases and surgery can be done for cosmetic improvement. This should however be delayed for as long as possible or until the patient has reached adulthood, as FD usually stabalises with skeletal maturation.6
Authors contribution:
Sulette Nel: 50% Chané Smit: 50%
REFERENCES
1. Hartley I, Zhadina M, Collins MT, Boyce AM. Fibrous Dysplasia of Bone and McCune-Albright Syndrome: A Bench to Bedside Review. Calcif Tissue Int. 2019;104(5):517-29. [ Links ]
2. El-Mofty SK. Fibro-osseous lesions of the cranio-facial skeleton: an update. Head Neck Pathol. 2014;8(4):432-44. [ Links ]
3. Hopkins C, de Castro LF, Corsi A, Boyce A, Collins MT, Riminucci M, et al. Fibrous dysplasia animal models: A systematic review. Bone. 2022;155:116270. [ Links ]
4. Weinstein LS. G(s)alpha mutations in fibrous dysplasia and McCune-Albright syndrome. J Bone Miner Res. 2006;21 Suppl 2:P120-4. [ Links ]
5. Miranda PG, Henriques JCG, Paulo LFB, Guedes C, Mitri FF, Silva CJ. Jaffe-Lichtenstein Syndrome Associated with a Simple Bone Cyst: Unprecedented Rare Case Report. Braz Dent J. 2020;31(5):557-61. [ Links ]
6. Baumhoer D. Bone-Related Lesions of the Jaws. Surg Pathol Clin. 2017;10(3):693-704. [ Links ]
 Correspondence:
Correspondence:
Chané Smit
Department of Oral Pathology and Oral Biology, University of Pretoria.
Tel +27 (0)12 319 2311; Email: chane.smit@up.ac.za


{kind=link}
{kind=link}