










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.77 no.5 Johannesburg 2022
http://dx.doi.org/10.17159/2519-0105/2022/v77no5a6
CASE REPORT
http://dx.doi.org/10.17159/2519-0105/2022/v77no5a6
Diagnosis and treatment of a maxillary lateral incisor with two root canals. A case report
JD Torres-Mantilla
Institution: Department of Endodontics, Carlos Lanfranco La Hoz Hospital. Saenz Peña avenue n/n 6. Puente Piedra. PC: 15118. Lima. Perú. Perú. ORCID: 0000-0003-4733-3489
ABSTRACT
Although endodontic treatment has shown high success rates, the factors involved in the failure cases are still being studied. In this sense, the complexity of interradicular anatomy may lead to inadequate instrumentation and the persistence of etiological factors related to apical periodontitis and endodontic failure. The present case report illustrates the occurrence, diagnosis and nonsurgical endodontic treatment of a maxillary lateral incisor with two canals. A 24-year-old Peruvian woman was referred complaining of darkening of the upper front tooth. After clinical examination, the patient was diagnosed with necrotic pulp and asymptomatic apical periodontitis. Still, radiographic examination revealed a disruption in the canal continuity, leading to a suspicion of unusual root canal morphology in the maxillary lateral incisor. By taking radiographs from different angles, according to the technique described by Clark, the presence of two independent canals was verified. Since most cases of endodontic failure are due to untreated canals, a predictable endodontic therapy must achieve the removal and neutralisation of etiologic factors related to periapical infiltration. The occurrence of additional root canals requires a correct interpretation of radiographic images to detect these variants and take the necessary considerations for proper endodontic treatment.
Keywords: Maxillary lateral incisor, separate apical foramen, two canals, morphological root canal anomalies.
INTRODUCTION
Academic literature reports a 90% success rate of endodontic treatment.1-3 Several studies attribute the high predictability of root canal treatment to removing and neutralising the agents involved in periapical infiltration4. For instance, Hoen and Pink5 found a 42% occurrence of missed canals in teeth selected for nonsurgical retreatment. These results are consistent with the investigations indicating untreated canals and defects in obturation as the most significant causes of failure.6-9 The study of internal root anatomy has allowed setting standard patterns regarding the number and configuration of root canals.10-17 In that sense, among maxillary teeth, the lateral incisors are typically described as single-rooted, with one canal, slightly flattened mesiodistally and with a disto-palatal orientated low curvature. 10,15,18 Although morphological root canal abnormalities of the maxillary lateral incisors are uncommon, 19-21 variations are frequently associated with "dens in dente", palatal grooves, gemination or fusion. 10,22,23 Besides, some reviews have informed a 3% incidence of two canals.10,16
As well as a thorough knowledge of the root anatomy, a detailed examination of the crown and preoperative radiographs are necessary to detect root canal anomalies. 13-17 An accurate treatment plan must include all present canals to achieve endodontic success. 1-9 This article describes a maxillary lateral incisor with two canals managed by nonsurgical endodontic treatment.
CASE REPORT
A 24-year-old Peruvian woman was referred to the Department of Endodontics at Carlos Lanfranco La Hoz hospital, Lima, Peru, for root canal treatment on the right maxillary lateral incisor. The chief complaint of the patient was "darkening of the upper front tooth". Medical history was noncontributory. Clinical examination revealed no extraoral abnormalities and a leaked palatal restoration. Response to both percussion and the cold test was negative. Mobility was within regular patterns (grade 1 according to the Miller index), while palpation and periodontal probing depth (2mm) evidenced neither alteration of adjacent soft tissues nor periodontal pockets. The adjacent teeth were clinically healthy and typically shaped at the crown. Radiographic examination revealed a periradicular radiolucency. Also, unusual root canal morphology suggesting two canals was suspected.
The patient was diagnosed with pulp necrosis and asymptomatic apical periodontitis. After obtaining informed consent, nonsurgical endodontic treatment was planned over two sessions, using Calcium hydroxide as an intracanal medication. The entire procedure was performed under 3.5x magnification.
The restoration was removed under local anaesthesia (2% Lidocaine with 1:80000 epinephrine), and the pulp chamber was accessed. After removing the superficial necrotic tissue and cleaning the chamber with 5% sodium hypochlorite, palatal and buccal canal entrances were identified. Under rubber dam isolation, the canals were accessed using hand files 10 (C-pilot, VDW). Working length was determined using an Apex Locator (ProPex Pixie, Dentsply) and controlled radiographically (Fig 2). Although radiographic control showed both canals converging, a 2mm difference in working length was recorded. A superposition was suspected considering palatal and buccal localisation of the entrances. In order to determine the accurate measurement of canals, another radiograph was taken at a severe distal angulation, and the presence of two independent canals could be confirmed.


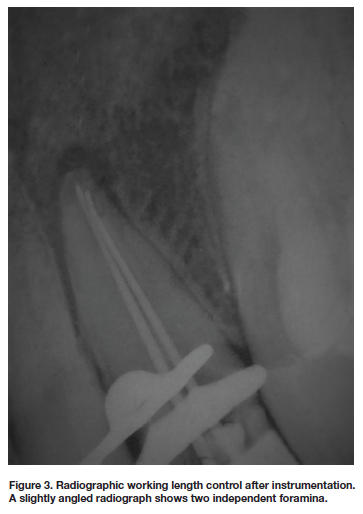
A glide path was created employing hand files until a 15 flexofile instrument was fitted loosely at working length in each canal and then a rotatory nickel-titanium file (Proglider, Dentsply). The canals were cleaned and shaped using constant irrigation of 5% sodium hypochlorite 3 mm before working length and reciprocating movement files (Wave One Gold, Dentsply) up to a 035 .06 file. Both canals had independent foramina (Fig. 3). A paste of Calcium Hydroxide (Calcifar-P, Eufar) was used as intracanal medication, and the access cavity was sealed with Zinc Polycarboxylate cement.
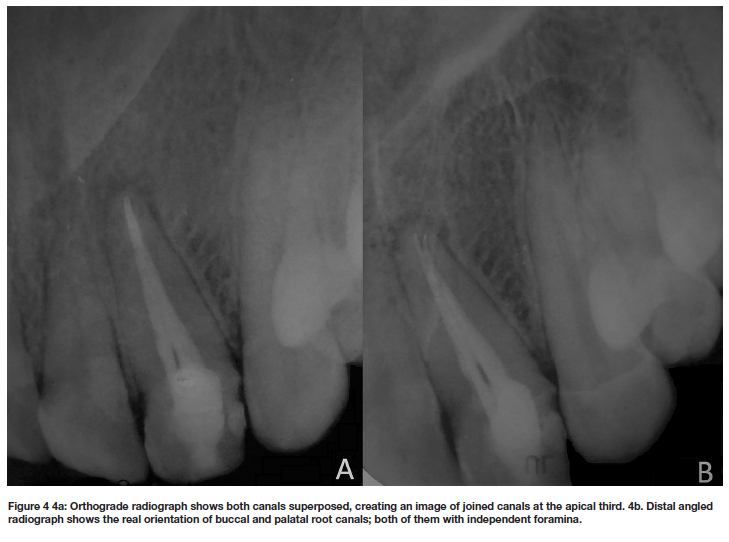
The final session was three weeks later. Calcium Hydroxide was removed from the canals with ultrasonic activation of 17% EDTA and 5% sodium hypochlorite. After controlling the working length radiographically, the canals were dried with paper points and obturated with non-standardised gutta-percha points (Fig. 4). A resin-based cement (AH plus, Dentsply) was used as the root canal sealer. Each of the canals was obturated employing the Tagger's hybrid technique. The tooth was provisionally restored, placing a lining glass ionomer cape at the bottom of the chamber and a composite covering. The patient was advised to get prosthetic rehabilitation.
DISCUSSION
Dental literature describes lateral maxillary incisors as a single-rooted tooth with one root canal in 100% of cases,10-17 despite some morphological studies have found a 3% incidence of two canals.10,16 Although this anatomical variant is infrequent,10,16,17 some case reports provide enough indications to note the presence of more than one root canal, which must be considered during the endodontic therapy to avoid untreated canals. 17,19-21
The root anatomical variations in maxillary lateral incisors are attributed to specific developmental defects: fusion, gemination, "dens in dente", and palatal groove. 10,22,23 Therefore, identifying the aetiology of the abnormality is crucial to developing an appropriate treatment plan. 17,22,23 Dental fusion is a type of anomaly characterised by two independent tooth buds that fuse during crown development, resulting in the formation of a tooth with double crowns and two root canals associated with a single root each. 17,21 Likewise, dental gemination consists of a single tooth divided during formation, resulting in two crowns with one root. Clinically both the fusion and the germination show alteration in the shape of the crown. 19,24 "Dens in dente" is the invagination of the enamel organ within the dental papilla before proper calcification. Although a small fossa may appear on the palatal surface, the diagnosis is usually made by noticing a radiopaque image expanding the affected root to create the appearance of a tooth inside another tooth.17,23,24 For its part, the palatal groove is a developmental disorder in which a deep groove begins in the area of the central fossa and extends apically over the root surface.17,23 Typically, the groove determines the appearance of palatal periodontal pockets, endo-periodontal lesions and surgical complemental treatment is required.22 In the present case, clinical examination showed a regular pattern in the shape of the maxillary lateral incisor, the number of teeth and the absence of invaginations and periodontal pockets. Besides, the radiographic image was compatible with one single root: regular-sized, normal proportioned and one continuous unique periodontal ligament space. This analysis dismissed the aforementioned developmental defects, leading to a diagnosis of two canals in one single root.
Radiographic analysis is decisive for the identification of additional canals. 11,12,14,18 Angled radiographs allow a clear interpretation of the direction and continuity of the canals. 17,20 Usually, additional root canals in the maxillary incisors join at the level of the apical third to end in a single foramen (Vertucci type ii)10,16,17. In the present case, each canal ended in an independent foramen (Vertucci type IV) (Fig. 3 and 4). The apical locator recorded a difference of 2mm between each canal, which indicated the presence of two separate foramina. The CBCT can be an essential help in detecting variations in the number and orientation of root canals.11-14,18,20 Even though it was not possible to access a CBCT for the present case, the usage of the buccal object rule (SLOB rule) described by Clark supplemented the limitation. Taking radiographs from different angles verified the independence of each canal. Even so, in cases where morphological alterations in the root canals are suspected, the use of a CBCT should be part of the protocol for endodontic treatment planning.
Several case reports demonstrate that most root canals in lateral incisors are located in palatine and buccal.19,20 In the present case, the use of 3.5x magnification and the flooding of the pulp chamber facilitated the location of the buccal canal entrance. Magnification has improved various endodontic procedures, leading to improve outcomes.25 It is utterly beneficial for proper exploration in small pulp chambers and narrow canals.
The relationship between anatomical alterations and treatment protocols is not entirely clear.10,22,23 Alterations of form such as fusion, gemination, "dens in dente", or palatal groove require individual therapeutic approaches concerning the singular disposition of the pulp chamber or the specific depth measurement of invagination in every single case.17,19,22,23 However, the variation in the number of canals does not affect the shaping, cleaning and obturation procedures required for periapical healing or prevention of apical periodontitis.17-21 Both canals were managed following the usual protocol for pulp necrosis in the present case. Only the curvature degree of the apical third was a consideration to use a system of reciprocating files along with preflaring.
In the systematic reviews founding variations in the number of root canals, the population under study is non-Caucasian and from a heterogeneous ethnicity.10,11,12,16 The cause of two root canals in the maxillary incisors may be due to an alteration of the normal development of the Hertwig epithelial sheath.24 Furthermore, some studies have related gender and ethnicity to morphological alterations of inter-radicular anatomy.13,14,16 This article reports the incidence of a maxillary lateral incisor with two canals, in a single root and with two independent foramina. The patient was a female native of Peru, whose population is characterised by marked ethnic heterogeneity.
CONCLUSION
In conclusion, deep knowledge of the dental anatomy is necessary to detect possible alterations of the internal root anatomy and treat them during endodontic therapy. In case of finding an alteration of the root anatomy, it would be necessary to determine its aetiology and the use of CBCT or angled radiographs to make an appropriate treatment plan. According to their curvature, permeability and pulp and periapical diagnosis, additional canals should be treated through regular protocols. Also, studies should be conducted on the morphological variability of the internal root anatomy considering ethnicity and gender.
Conflicts of interest
The author has no conflict of interest to declare.
REFERENCES
1. Friedman S, Abitbol S, Lawrence HP. Treatment outcome in endodontics: the Toronto Study-phase 1: initial treatment. J Endod. 2003; 29(12):787-93. [ Links ]
2. Setzer FC, Boyer KR, Jeppson JR, Karabucak B, Kim S. Long-term prognosis of endodontically treated teeth: a retrospective analysis of preoperative factors in molars. J Endod. 2011; 37(1):21-5 [ Links ]
3. Siqueira JF. Reaction of periradicular tissues to root canal treatment: benefits and drawbacks. Endod Topics. 2005; 10(1):123-47. [ Links ]
4. Gomes BPFA, Pinheiro ET, Jacinto RC, Zaia AA, Ferraz CCR, Souza-Filbo FJ. Microbial analysis of canals of root-filled teeth with periapical lesions using polymerase chain reaction. J Endod. 2008; 34(5):537-40. [ Links ]
5. Hoen MM, Pink FE. Contemporary endodontic retreatments: an analysis based on clinical treatment findings. J Endod. 2002(12); 28:834-6. [ Links ]
6. Song M, Kim H, Lee W, Kim E. Analysis of the Cause of Failure in Nonsurgical Endodontic Treatment by Microscopic Inspection during Endodontic Microsurgery. J Endod. 2011;7(11):1516-19. [ Links ]
7. Khan M, Rheman K, Saleem M. Causes of Endodontic Treatment Failure-A Study. Pakistan Oral & Dental Journal 2010; 30(1):232-6. [ Links ]
8. Tabassum S, Khan FR. Failure of endodontic treatment: The usual suspects. Eur J Dent. 2016;10(1):144-147. [ Links ]
9. Olcay K, Ataoglu H, Belli S. Evaluation of Related Factors in the Failure of Endodontically Treated Teeth: A Cross-sectional Study. J Endod. 2018;44(1):38-45. [ Links ]
10. Cohen S, Hargreaves KM, Berman LH. Cohen's Pathways of the Pulp. 10th ed. St. Louis, MO: Mosby; 2010. [ Links ]
11. Martins, J. N. R., Marques, D., Mata, A., & Carames, J. Root and root canal morphology of the permanent dentition in a Caucasian population: a cone-beam computed tomography study. Int Endod J. 2017; 50(11): 1013-1026. [ Links ]
12. Estrela, C, et al. Study of Root Canal Anatomy in Human Permanent Teeth in A Subpopulation of Brazil's Center Region Using Cone-Beam Computed Tomography - Part 1. Braz Dent J. 2015; 26(5): 530536. [ Links ]
13. Pan, J., Parolia, A., Chuah, S. R., Bhatia, S., Mutalik, S., & Pau, A. Root canal morphology of permanent teeth in a Malaysian subpopulation using cone-beam computed tomography. BMC oral health. 2019; 19(1): 14. [ Links ]
14. Martins JN, Marques D, Silva EJNL, Carames J, Versiani MA. Prevalence Studies on Root Canal Anatomy Using Cone-beam Computed Tomographic Imaging: A Systematic Review. J Endod. 2019 Apr;45(4):372-386. [ Links ]
15. Ahlbrecht CA, Ruellas ACO, Paniagua B, Schilling JA, McNamara JA Jr, Cevidanes LHS. Three-dimensional characterization of root morphology for maxillary incisors. PLoS One. 2017 Jun 8;12(6): e0178728. doi: 10.1371/journal.pone.0178728. eCollection 2017. [ Links ]
16. Sert S, Bayirli G. Evaluation of the Root Canal Configurations of the Mandibular and Maxillary Permanent Teeth by Gender in the Turkish Population. J Endod. 2004; 30(6): 391-8. [ Links ]
17. Ahmed HM, Hashem AA. Accessory roots and root canals in human anterior teeth: a review and clinical considerations. Int Endod J. 2016 Aug;49(8):724-36. [ Links ]
18. Park PS et al. Three-dimensional analysis of root canal curvature and direction of maxillary lateral incisors by using cone-beam computed tomography. J Endod. 2013; 39(9):1124-9. [ Links ]
19. Romano N, Souza-Flamini L, Lima I, Gariba R, Miranda A. Geminated Maxillary Lateral Incisor with Two Root Canals. Case Rep Dent. 2016; 3759021. doi: 10.1155/2016/3759021. [ Links ]
20. Elbay M, Kaya E, Elbay Ü&, Saridag S, Sinanoglu A. Management of two-rooted maxillary central and lateral incisors: A case report with a multidisciplinary approach involving CAD/CAM and CBCT technology. J Pediatr Dent. 2016;(4):51-4. [ Links ]
21. Saberi, E., Bijari, S., & Farahi, F. Endodontic Treatment of a Maxillary Lateral Incisor with Two Canals: A Case Report. Iran Endod J. 2018; 13(3), 406-408. [ Links ]
22. Kishan KV, Hegde V, Ponnappa KC, Girish TN, Ponappa MC. Management of palato radicular groove in a maxillary lateral incisor. J Nat Sci Biol Med. 2014; 5(1):178-181. [ Links ]
23. Barzuna M. Dens in dente: anomalía dental difícil de tratar. reporte de un caso clínico. Rev. Cient. Odontol. 2013; 9(2): 35-38. [ Links ]
24. Sapp P, Eversole L, Wysocki G. Contemporary Oral and Maxillofacial Pathology 2nd. ed. Amsterdam, MO: Mosby; 2004. [ Links ]
25. Low JF, Mohd Dom TN, Baharin SA. Magnification in endodontics: A review of its application and acceptance among dental practitioners. Eur J Dent. 2018; 12(4): 610-616. [ Links ]
 Correspondence:
Correspondence:
José Diego Torres Mantilla
Department of Endodontics, Carlos Lanfranco La Hoz Hospital.
Tel: 011-51-992052955; E-mail address: diegotm548@gmail.com


{kind=link}