










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Dental Journal
versión On-line ISSN 0375-1562
versión impresa ISSN 0011-8516
S. Afr. dent. j. vol.77 no.3 Johannesburg abr. 2022
http://dx.doi.org/10.17159/2519-0105/2022/v77no3a4
RESEARCH
Exploring the feasibility of a framework to align a competency framework in a dental curriculum: a Delphi study
RD MaartI; RZ AdamII; JM FrantzIII
IBChD, MPhil, PhD, HOD Prosthetics, Faculty of Dentistry, University of the Western Cape, https://orcid.org/0000-0002-1560-040X
IIBChD, MSc, PhD), Senior lecturer, Restoratve Dentistry, Faculty of Dentistry, University of the Western Cape https://orcid.org/0000-0002-2645-9878
IIIPhD), DVC: Research and Innovation, Department of Physiotherapy, University of the Western Cape. https://orcid.org/0000-0002-8296-5601
ABSTRACT
AIM: The aim of this study was to test the feasibility of an implementation framework for an undergraduate competency framework by means of a Delphi study.
METHODS: A modified Delphi research design consisting of two rounds was conducted and aimed to seek consensus defined as agreement of 70% or more from a group of experts. Twenty-two (22) dental experts were purposefully selected from the four dental schools in South Africa. An online survey consisting mainly of closed-ended questions was used and analysed quantitatively. In addition, the second part of each question included a comment section to allow participants to elaborate on their answer. Comments were considered as adapted statements for the second round of the Delphi.
RESULTS: Thirteen (13) participants completed the first round, and 10 participants completed the second round of the Delphi study. Following the first round of the Delphi, consensus (70%) was reached for five of the seven statements. These statements focus on the impact of internal and external stakeholders on the dental schools, leadership support for faculty development, teaching and learning changes, and curriculum mapping. Statements that needed further consideration in round 1 included impact of institutional framework and diversity of academics. Consensus was reached for both the diversity of academics statements in round 2.
CONCLUSION: The results suggest that the proposed framework to align and implement the AfriMEDS core competency framework was feasible. However, from the comments of the dental experts there seems to be no common understanding of implementation and alignment of the institutional frameworks and the AfriMEDS core competency framework.
Keywords: Competency framework, Delphi study, dental curriculum, competencies
INTRODUCTION
Competency frameworks are documents produced by regulating and accrediting bodies to create a shared model of performance standards of particular milestones along the professional career continuum.1 The African Medical Education Directions for Specialists (AfriMEDS) core competency framework was adapted from the Canadian Medical Educational Directives for Specialists (CanMEDS) by the Health Professions Council of South Africa (HPCSA) to inform undergraduate medical and dental curricula in South Africa.2 Evidence of the incorporation and alignment of the core competencies in the undergraduate dental curricula outlined in AfriMEDS is required during the HPCSA accreditation processes. No explicit guidelines for the implementation of AfriMEDS were prescribed, allowing dental schools' autonomy to incorporate and implement this core competency framework. Competency-based education (CBE) provides a framework for developing educational programmes, but it is with implementation that various challenges emerge.3
Differences of CBE from the more traditional approaches are: (i) a focus on outcomes, (ii) an emphasis on abilities, (iii) a reduced emphasis on time-based training, and (iv) the promotion of learner-centredness. These differences cause challenges and implications for designing and implementing CBE.3 Essential key differences between CBE and traditional educational frameworks lie in the structure and process of education . Traditional education tends to focus on what and how learners are taught and less on whether or not they can use their learning to solve problems, perform procedures, communicate effectively, or make good clinical decisions.3 The focus is more teacher-centred with attention mostly on the content or curriculum. Contrarily, CBE places the curriculum as an end-product of a needs assessment rather than as the structure that constrains educational objectives and assessments.3
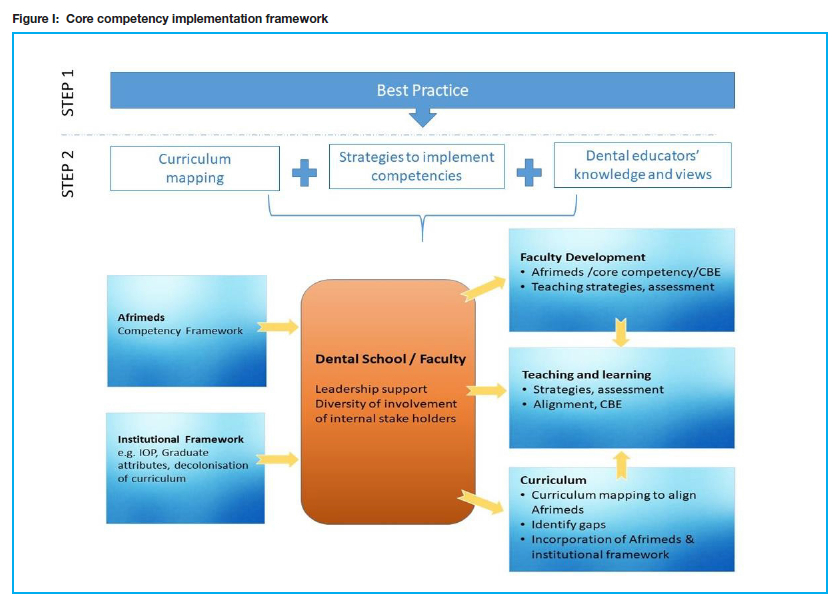
Considering the differences between the traditional model of education and CBE, a shift from a teacher-centred to a learner-centred approach that focusses on addressing the health needs of the society is required to transform traditional curriculum to CBE. Implementing the CanMEDS competency framework requires a systematic multifaceted approach that includes: standards for curriculum, teaching and assessment, faculty development, research and development, and outreach.4 This multifaceted implementation approach aligns with the CBE model (Figure I) that involves competency outcomes, curriculum, and assessment. Factors that foster the implementation of a competency-based curriculum include accrediting bodies' support of this change; support and buy-in from stakeholders, i.e., institutional leaders; available resources; and effective change management.5
Another facet for the implementation is the involvement of a diversity of stakeholders, both within and outside academia, and a careful 'orchestration' of the change process.6 A combination of strong external pressure, internal dissatisfaction with the existing educational quality (often latent among teachers, students, and alumni), and courage of the institutional leadership to make a fundamental change, will make transformation from a 'traditional' curriculum to a competency-based curriculum possible.6 The alignment to face accrediting and certifying bodies in support of the competencies and outcomes assessment provided a major implementation of curriculum reform or changes thrust.7 As a consequence of the HPCSA's adoption of the AfriMEDS core competency framework, it provided external pressure for transformation to a CBE model for all undergraduate dental curricula in South Africa. When both accreditors and certifiers require evidence of competency attainment, residency programmes will be doubly motivated to increase their emphasis on these areas.7
Concerns have identified challenges in the implementation of competency-based medical education (CBME), and consequently have advised caution. Addressing the challenges in the implementation of CBME requires consideration of the implications for the complex systems in which our education programmes exist.8 This study is the final phase of a larger study of the first author that aimed to develop a framework to implement the AfriMEDS core competency framework (Figure I). The aim of this study was to test the feasibility of this implementation framework by means of a Delphi study.
METHODS
Research Design
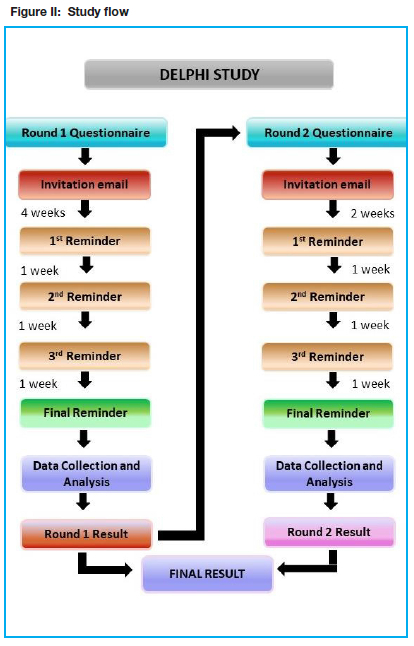
A Delphi approach works best with higher-level concepts as opposed to an in-depth exploration of the topic.9 In addition, this technique is a creative and efficient method of facilitating health sciences education research.10 The technique brings advantages of clarity, privacy, voice, and collegiality. In doing so it engages the issues of anonymity and disclosure of relevant information whilst protecting participants' rights to privacy.11 Therefore, the Delphi research design was considered appropriate to test the feasibility of the proposed implementation framework for the AfriMEDS core competency framework. The Delphi study was used to assess the feasibility and seek consensus from a group of experts to validate the designed intervention.12 A modified version of the traditional Delphi was used as depicted in Figure II. In the first round, the designed implementation framework was presented to the panel of experts to elicit consensus compared to the traditional first round that includes questions or expert opinions in order to gain insight into a specific issue.
Participants are usually required to rate their level of agreement with each statement using a Likert scale. Offering a finite number of ranking options is a way of encouraging the panel to commit to a particular item.10 In this study, experts were asked to respond to a 4-point Likert scale offering the options: "strongly disagree", "disagree", "agree", and "strongly agree". A neutral middle point was excluded to compel respondents to choose a particular option. This strategy assisted in making clear calculations on agreement and disagreement.13,14 It is critical that the researcher carefully determines what particular definition of 'consensus' is to be used in his/her study in advance. The first and second round of consensus was defined as when 70% or more of the respondents agreed with a statement.
Panel of experts
There are no criteria upon which to determine the nature of the "expert", the optimal panel size, or even selection criteria of the panellists in a Delphi study.12 For this study, the experts - dental academics with experience in curriculum development, design, or as programme accreditors -were purposefully selected. These experts were invited from all four dental schools in South Africa. Invitations to participate in this online Delphi study were emailed to a total of 22 dental experts from the dental schools/faculties. Information sheets explaining the purpose of this study and the relevant information regarding the study were included in the invitations.
Survey
The Google Forms platform was used to send a Google survey link to all participants via their email. Regular emails (4 in total) with reminders to complete the online survey were sent to all the participants. The consent form was included in the first part of the online survey. The surveys consisted mainly of closed-ended statements that were analysed quantitatively. In addition, the second part of each question included a comment section to allow participants to elaborate on their answer in the first part of the statement. Comments were adapted to statements for the second round of the Delphi.
Ethics
Ethics clearance was obtained from the University of the Western Cape's Biomedical Research Ethics Committee (BM 19/1/23). True anonymity is ensured when no one (including the researcher) can link a response to a participant. Because of the iterative process inherent in the Delphi technique, true anonymity cannot be guaranteed as the individual panel member's responses are unknown to the other participants but known to the researcher.15 At all phases of the study an information sheet was provided with enough detail to clarify the purpose of the project and what it entails. All of the participants signed a consent form and had the right to withdraw from the study at any stage without repercussions. The information gathered was kept anonymous by assigning numbers to the dental experts instead of using their names.
RESULTS
Round 1 of the Delphi study
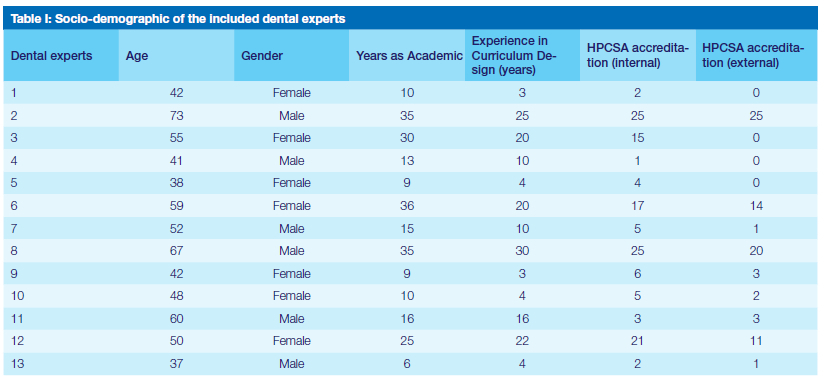
Thirteen (13) participants (59%) completed the first round of the Delphi study. The socio-demographic information collected included age, gender, and number of years as an academic, years of experience in curriculum design, and HPCSA accreditation (Table I). Of the participants, six (6) were male and seven (7) were female. The average age was 51 years, and the average number of years as an academic was 19. In addition, as a collective, the years of experience in curriculum design ranged from 3 to 30 years, with an average of 13 years. The participants also had 10 years of experience with HPCSA accreditation processes.
Results of round 1 of the Delphi study
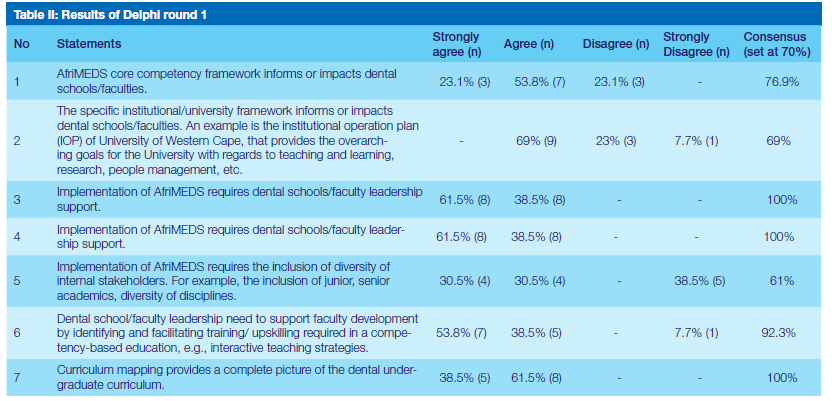
The first round of the Delphi aimed to reach consensus on seven statements (Table II), which was defined as being achieved when 70% or more of the dental experts agreed with each of the statements of the questionnaire. From the results, the dental experts reached consensus for five of the statements (numbers 1, 3, 5, 6 and 7) in the questionnaire. Verbatim quotes are provided below to offer some understanding of the dental experts' opinions. No consensus was reached for statements 2 and 4, and comments relating to these statements were analysed to inform the second round of the Delphi study. Statement 1: AfriMEDS core competency framework informs or impacts dental schools/faculties.
The excerpts below capture some of the comments of the dental experts that disagreed with this statement:
"My experience with accreditation is that very few dental academics either know of these or can translate them into meaningful attributes for their students". DE 1
"At the moment very, few people understand it - it's a lot of hype and talk, but not many wet nosed clinicians or junior academics have any idea about its actual contents and impact". DE 5
"Each dental school has autonomy and tends to follow university framework. ¡The] AfriMEDS framework is only relevant as ¡a] paper pushing exercise when accreditation is on the horizon". DE 6
Statement 3: Implementation of AfriMEDS requires dental schools/faculty leadership support.
All of the dental experts agreed with this statement, as noted in the following excerpts:
"Any change needs strong leadership". DE 1
"Without buy-in from the key decision-makers, such drastic approach changes will usually not succeed". DE 3
Statement 5: Dental school/faculty leadership needs to support faculty development by identifying and facilitating training/upskilling required in a competency-based education, e.g., interactive teaching strategies.
Most of the dental experts supported this statement, as reflected in the following excerpts:
"Most dental educators have no formal T&L [teaching & learning] training, and are merely just clinicians with experience in treating patients and some minor understanding of education strategies". DE 10
"Faculty development can help in furthering scholarship, collaboration, leadership, and professionalism, which are central in AfriMEDS". DE 3
"Of course, leadership must support development. What is more important, is how they identify the needs, and what criteria will they use". DE 1
Statement 6: Changes in teaching and learning needs to be encouraged to promote a competency driven framework.
The comments of dental experts that supported this statement are captured below:
Statement 7: Curriculum mapping provides a complete picture of the dental undergraduate curriculum.
All of the dental experts agreed with this statement. Some of their comments are included below:
"Any map or picture is useful to illustrate a complex arrangement in a nutshell". DE 7
"Curriculum mapping will allow us to view operational curriculum and actually see if it speaks to the competencies needed for the modern South African dentist". DE 12
Comments about the AfriMEDS core competency framework highlighted the lack of knowledge and level of importance given to this framework at the dental schools. Dental experts agreed that this framework impacted and informed the dental schools. However, it is suggested that the superficial manner that dental academics engage with AfriMEDS contributes to their level of understanding. Accreditation of dental schools is undertaken every four years, and if AfriMEDS is only engaged with superficially as part of the accreditation process, it limits the level of understanding and impact on the dental curriculum. The practice of most of the dental schools is that the accreditation process is managed and conducted by senior academics. Therefore, the more junior dental academics have limited exposure, which contributes to their lack of understanding and knowledge of AfriMEDS. Similarly, the impact of the institutional framework and how it translates to the dental curriculum is influenced by the lack of knowledge and understanding by all levels of staff, particularly junior dental academics. The dental experts agreed that the implementation of the AfriMEDS core competency framework requires support from the leadership, referred to as 'buy-in'. Absence of the latter could underpin the lack of understanding and knowledge of dental academics regarding the AfriMEDS core competency framework. The dental experts underscored the importance of informing all levels of dental academics that changes in teaching and learning practices are required for the successful implementation of a competency framework. The latter's perceived resistance to changes could possibly be attributed to their lack of consultation or involvement in curriculum related matters.
Comments of dental experts related to the survey statements
Statement 2: The specific institutional/university framework informs or impacts dental schools/ faculties. An example is the institutional operation plan (IOP) of one university in South Africa that provides the overarching goals for the university with regards to teaching and learning, research, people management, etc.
From the results, nine (9) (69%) of the dental experts agreed that the specific institutional framework impacts or informs dental schools/faculties. As the consensus was defined at 70%, this statement was reframed and included in the second round of the Delphi.
Some comments related to this statement in the first round of the Delphi are indicated below:
"Though the curricula responds to professional accreditation requirements in principle, local institutional plans are central too". DE 3
"Sometimes the use of such models are merely lip service to impress accreditors. Models are often not fully implemented or understood". DE 5
"A school/faculty is part of a university and as such its framework contributes and informs the university framework and therefore should be aligned". DE 6
"The IOP is a generic framework which does not adequately address all the competencies required to be taught/ transferred to the oral health professional". DE 8
"I became aware that in general academic lecturers are not familiar with the contents of the IOP. Lecturers' involvement and contributions to the IOP are limited. Although there is an effort from lecturers to align their learning outcomes with the UWC graduate attributes, the enactment in teaching, learning and assessment is limited". DE 9
"Faculty plans need to be aligned with [the] institutional plan so that the system functions in alignment and not out of sync with each other. Staff need to understand how they fit into the whole institutional plan as a department, as well as a faculty/ school". DE 10
It appears that the dental experts agreed that the institutional framework impacts the dental schools/faculties. Concerns were raised about the alignment of the dental specific competencies guided by the HPCSA and the institutional frameworks. Similar to the AfriMEDS core competency framework, it was suggested that the understanding and knowledge of the institutional plans were superficial and there was limited engagement related to accreditation processes. Another concern is that lecturers in the dental schools were not familiar with the institutional framework and its translation to their teaching and learning practices. Therefore, this statement was restructured in round two of this Delphi study to include the dental experts' views.
Statement 4: Implementation of AfriMEDS requires the inclusion of diversity of internal stakeholders. For example the inclusion of junior, senior academics, diversity of disciplines.
From the results, the dental experts agreed that implementation of AfriMEDS requires the inclusion of a diversity of internal stakeholders: four (4) dental experts (30.5%) "strongly agreed", four (4) (30.5%) "agreed", and Ave (5) (38.5) "strongly disagreed" with statement 4. As the consensus was determined at 70%, this statement was reframed and included in round 2 of this Delphi study.
The following extracts reflect some of the dental experts responses to this statement:
"All role players and stakeholders that are involved in teaching and training should be part of the process". DE 1
"There needs to be a lot more information provided to all staff and not just at the higher levels". DE 3
"It seems the lower-level staff never get all the information] and don't have much [of a] voice. Once a decision is made, they are told to comply without understanding the full implications or how to adapt". DE 3
"Including diverse stakeholders will ensure that [the] framework is understood by all, but also helps the development of competencies through multidisciplinary and interdisciplinary collaboration". DE 3
"Dentistry is multifaceted in its clinical structure and disciplines; the expertise and experience of senior academics will be enhanced with innovation on a technology level from junior academics. Ensuring the team is diversified from a clinical discipline perspective is important to ensure a student that qualifies with competencies in all fields of dentistry". DE 8
"Equal opportunities - all staff are expected to understand and enact the faculty's commitment to ensuring equality and diversity in all activities". DE 10
"All stakeholders play a role in owning and crafting a sound academic programme/curricula". DE 12
"Young academics see the industry very differently and should be key drivers in shaping it for the future". DE 12
From the above comments, it appears that dental experts agree that the inclusion of diverse stakeholders is important to ensure the successful implementation of the AfriMEDS competency framework in dental schools/ faculties. It is suggested that the exclusion of all levels of academics (particularly junior) in curriculum changes and accreditation processes contributes to the overall lack of knowledge and understanding of the implementation of AfriMEDS. The views of junior academics appear to be ignored and devalued. However, no consensus was reached, and no suggestions or alternative statements were offered. Statement 2 was rephrased for better clarity and included in the second round of the Delphi study.
Delphi round 2
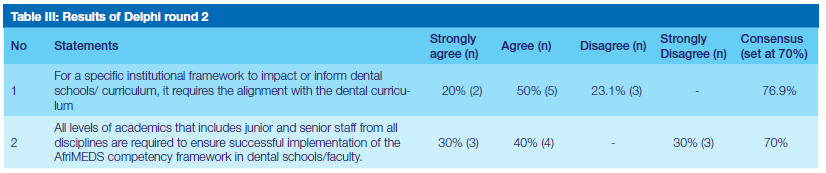
Round 2 of the Delphi survey was sent to the selected dental experts that responded in the first round. Consent was completed again, and the same demographic information was included. Following the results of round 1, only two statements were included in this round of the Delphi study, as illustrated in Table III.
Round 2 of the Delphi study
In this round, four sets of invitations were mailed to the dental experts. Ten (10) participants responded and participated in the second round of the Delphi study. Consensus of 70% (Table III) was reached for both statements included in round 2.
Comments from the dental experts who agreed with statement 1 are included below:
"For consistency, faculty plans must be in place". DE 2
"Institutional documents set the context for faculty curricula". DE4
"Most are still run in the way they always have but with a lot more paperwork and red tape to make them look different". DE 5
A dental expert who disagreed with statement 1 mentioned the following:
"In line with the above research, to answer the question why institutional documents does not impact faculty curricula, faculty curricula supported by research validated by rigour may be perceived as less relevant and is often not implemented or sustained widely, because it does not fit nuanced, real-world context[s] such as the university and classrooms; and (i) evidence-based practices that are perceived [as] relevant, but less rigorous are liable to promote ineffective practices". DE 3
Comments from the dental experts who agreed with statement 2 are indicated below:
"Generic competencies like that are taught by everybody". DE 2
"Need buy-in from everyone". DE 5
"For a plan to work, every person must buy in". DE 6
The dental experts who disagreed with statement 2 stated that:
"We have not implemented this curriculum at our faculty, it has not informed our teaching & learning practise". DE 1
"But only if all levels understand the desired outcomes". DE 3
DISCUSSION
Consensus was reached regarding the statement that the AfriMEDS core competency framework informs or impacts dental schools or faculties. Of those who disagreed, dental experts expressed their concern about dental academics, especially junior academics' knowledge of AfriMEDS and how this translates to meaningful attributes for their students. In addition, some dental experts commented that this framework had no significant impact on dental schools. Dental experts expressed concern that dental academics are only trained in the dentistry discipline and not as teachers. The recent shift in pedagogic focus towards a more student-centred education impacts the educator.16 Similarly, the shift to CBE in South Africa impacts the dental educator. The suggested exclusion of all levels of academics in curriculum related matters and the accreditation process contributes to the lack of understanding and knowledge of AfriMEDS.
Furthermore, the dental experts in this study supported faculty development, specifically in teaching and learning that would benefit the transition of CBE and alignment of the AfriMEDS core competency framework with the undergraduate dental curricula. The areas of competence identified for dental educators include educational theories, principles and methods, assessment and feedback, curriculum and evaluation, management, healthcare system, and professionalism.16 Teachers also need pedagogic education to be able to implement changes, therefore dental schools should organise a variety of ongoing training activities for teachers.17 Individual educators may not need to be competent in every area but should be competent in areas relating to their specific roles.16
From the comments, it was suggested that the AfriMEDS competency framework was not completely understood and integrated in the dental curriculum and was only a superficial exercise related to the HPCSA accreditation process.
Interestingly, there were comments to more than one statement that related to dental academics. Inclusion and training of all dental academics in curriculum matters, AfriMEDS, faculty development, and other educational faculty development was suggested. Experiences or views of some dental experts were that only selected dental academics were involved in curriculum changes and accreditation. However, previous research has focused on educational change processes, rather than preparing educators to support changes.16 Inclusion and faculty development relating to curriculum changes and accreditation would result in improved understanding and cooperation of dental academics. It is important for educators to understand curriculum evaluation, which is required for curriculum development and implementation. However, leadership and teamwork are needed to manage change, solve institutional problems, and secure the future profession.16 In this study, dental experts reached consensus that implementation of AfriMEDS requires dental schools/faculty leadership support. Similarly, the transition towards CBME requires a strong leadership for change.18
Most (69%) of the dental experts agreed that the specific institutional framework impacts or informs dental schools/ faculties. Although consensus was not reached on this point, there were no disagreements; therefore, this statement was reframed and included in the second round of this Delphi study. Results from the second round showed that the dental experts reached consensus (70%) that the institutional framework impacts or informs the dental schools. Following the rephrase of the second statement in round 2, the dental experts reached consensus (70%) relating to all levels of academics, which includes that junior and senior staff from all disciplines are required to ensure successful implementation of the AfriMEDS competency framework in dental schools/faculties.
The transition towards a competency framework must be supported by a systematic approach of curriculum mapping, which will provide the transparency necessary for students, teachers, and the medical school to know what is taught and/or should be learned by when.18 Complete consensus (100%) was reached that curriculum mapping provided a comprehensive picture of the dental undergraduate curriculum. Coordinated use of a common framework to evaluate the implementation within different medical schools, combined with the curriculum mapping process, would be an excellent basis to learn from each other and to be able to compare the different curricula.18 The role and impact of institutional frameworks on the four dental schools varied. This is understandable as the focus and background of the four institutions differed. For example, the university rankings, graduate offerings, and demographics of staff and students impact the underpinning of the institutional framework. From the responses of the experts, it was suggested that the institutional framework did not align or impact on the dental schools' curriculum. Van Melle et al.,9 suggest that educational innovations such as CBME are often complex, and highly sensitive to context, thus aligning with the varied impact of the institutional framework on dental schools in this study. From the comments from the dental experts, the AfriMEDS competency framework and CBE have not been implemented in their dental schools. In a study by Sohrmann et al.,18 which introduced a new competency framework into undergraduate medical curricula, the importance of developing a shared understanding of the concepts underlying CBME and their implications for teaching and learning were highlighted.
Similarly, in this study another dental expert suggested that consideration of the AfriMEDS competency framework is a "paper exercise" related to HPCSA accreditation visits. The varied comments regarding the AfriMEDS core competency framework amongst dental experts from all four schools suggest that there is no common understanding relating to this.
CONCLUSION
The results suggest that the proposed framework to align and implement the AfriMEDS core competency framework in an undergraduate dental curriculum was feasible. However, from the comments of the dental experts, there seems to be no common understanding, implementation, and alignment of institutional frameworks with the AfriMEDS core competency framework. In addition, to address the overall lack of understanding and knowledge of AfriMEDS, leadership of dental schools in South Africa need buy-in and support for a specific faculty development workshop. These faculty development workshops should explore how the AfriMEDS core competency framework translates and aligns to the undergraduate dental curriculum in order to establish a common understanding and buy-in from all dental academics. In doing so, the inclusion of all dental academics in these workshops have the potential to facilitate the success of the implementation of the AfriMEDS core competency framework across all four dental schools in South Africa. In turn, it would allow a more meaningful engagement of all dental academics with the AfriMEDS core competency framework and its alignment to the dental curriculum as part of the accreditation processes. Since institutional frameworks and the contexts of dental schools vary, this needs to be considered and included in the HPCSA accreditation process.
REFERENCES
1. Rich JV. Do professions represent competence for entry-to-practice in similar ways? an exploration of competence frameworks through document analysis. IJSTL. 2019; 13(3):5. [ Links ]
2. Medical and Dental Professions Board (MDB) of the Health Professions Council of South Africa (HPCSA). Core competencies for undergraduate students in clinical associate, dentistry and medical teaching and learning programmes in South Africa. [2014]. Available from: http://www.hpcsa.co.za/uploads/editor/UserFiles/downloads/medical_dental/MDBCoreCompetencies - ENGLISH-FINAL2014.pdf [ Links ]
3. Gruppen LD, Burkhardt JC, Fitzgerald JT, Funnell M, Haftel HM, Lypson ML et al. Competency-based education: Programme design and challenges to implementation. ME. 2016; 50(5):532-539. https://doi.org/10.1111/medu.12977 [ Links ]
4. Frank JR, Danoff D. The CanMEDSinitiative: implementing an outcomes-based framework of physician competencies. MT. 2007; 29(7):642-647. https://doi.org/10.1080/01421590701746983 [ Links ]
5. Mejicano GC, Bumsted TN. Describing the journey and lessons learned implementing a competency-based, time-variable undergraduate medical education curriculum. AM. 2018; 93(3):S42-S48. [ Links ]
6. Koster A, Schalekamp T, Meijerman I. Implementation of Competency-Based Pharmacy Education (CBPE). Pharm. 2017; 5(1):10. https://doi.org/10.3390/pharmacy5010010. [ Links ]
7. Batalden P, Leach D, Swing S, Dreyfus H, Dreyfus S. General competencies and accreditation in graduate medical education. HA. 2002; 21(5):103-111. [ Links ]
8. Hawkins RE, Welcher CM, Holmboe ES, Kirk LM, Norcini JJ, Simons KB et al. Implementation of competency-based medical education: are we addressing the concerns and challenges? Med Educ. 2015; 49(11):1086-1102. [ Links ]
9. Van Melle E, Frank J, Holmboe ES, Dagnone D, Stockley D, Sherbino, JA Core components framework for evaluating implementation of competency-based medical education programs. AM. 2019; 94(7):1002-1009. https://doi.org/10.1097/ACM.0000000000002743 [ Links ]
10. De Villiers MR, De Villiers PJ, Kent AP. The Delphi technique in health sciences education research. MT. 2005; 27(7):639-643. [ Links ]
11. Cohen L, Manion K, Morrison K. Research methods in education. 7th ed. London and New York: Taylor & Francis; 2011. [ Links ]
12. Hsu C, Sandford B. The Delphi Technique: Making sense of consensus. PARE. 2007; 12(10):1-8. [ Links ]
13. Linstone HA, Turoff M, editors. The Delphi method: Techniques and applications. Reading, MA: Addison-Wesley; 1975. [ Links ]
14. Goodman CM. The Delphi technique: a critique. JAN. 1987; 12(6):729-734. [ Links ]
15. Keeney S, Hasson F, McKenna H. Consulting the oracle: ten lessons from using the Delphi technique in nursing research. JAN. 2006; 53(2):205-212. [ Links ]
16. Chuenjitwongsa S, Oliver RG, Bullock AD. Developing educators of European undergraduate dental students: towards an agreed curriculum. EJDE. 2018; 22(3):179-191. [ Links ]
17. Oliver R, Kersten H, Vinkka-Puhakka H, Alpasan G, Bearn D, Cema I et al. Curriculum structure: principles and strategy. EJDE. 2008; 12:74-84. [ Links ]
18. Sohrmann M, Berendonk C, Nendaz M, Bonvin R. Swiss Working Group for Profiles Implementation. Nationwide introduction of a new competency framework for undergraduate medical curricula: a collaborative approach. SMW, 2020; 150:p.w20201. [ Links ]
 Correspondence:
Correspondence:
Dr Ronel Maart
Private Bag XI, Tygerberg, 7505. South Africa
Email: rmaart@uwc.ac.za.
Tel: +27 21 937 3181
South Africa
Author contributions:
4. Ronel D Maart: Principle author 50%
5 . Razia Z Adam : co-author 25%
6 . Jose M Frantz : co-author 25%


{kind=link}
{kind=link}
{kind=link}
{kind=link}