










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Dental Journal
versión On-line ISSN 0375-1562
versión impresa ISSN 0011-8516
S. Afr. dent. j. vol.77 no.3 Johannesburg abr. 2022
http://dx.doi.org/10.17159/2519-0105/2022/v77no3a6
REVIEW
An evidence-based guide to occlusion and articulation. Part 3: A guide to functional occlusion: teeth vs joint.
Owen CP
BDS, MScDent, MChD, FCD(SA), Professor Emeritus, Faculty of Health Sciences, University of the Witwatersrand Johannesburg, South Africa, ORCID: 0000-0002-9565-8010
SUMMARY AND PREAMBLE TO THE SERIES
Although this is essentially a review, it has not been written in the passive, third-person style normally associated with scientific writing, as it is intended to be thought-provoking and, hopefully, educational. It has therefore been written in more of a conversational style, and is aimed at students, dentists and dental technicians who are receptive to a slightly different view of occlusion and articulation, based on evidence.
Occlusion is a topic that has become a kind of archaic minefield of conflicting ideas, propositions, and above all, solutions, most of which are based on a complete lack of understanding of the evolution and development of teeth, and by extension, of clinically objective evidence.
That in itself is a statement of conflict (and perhaps even heretical), but it is by way of warning that this guide is not going to be much like anything you will And in standard text-books of dentistry or dental technology. It is, rather, an attempt to help you navigate through what you will read elsewhere, in the hope that eventually you will And an understanding that you can live with. It will appear as a sequential series in 7 Parts.
A guide to functional occlusion: teeth vs joint
Thousands and thousands of words have been written on the form of the teeth and their arches, and here we are in the 21st century of the present era, and still we use terminology from the pioneers of the early 20th century! This is a problem, because it gives rise to a purely mechanistic approach, especially when replacing all the teeth with complete dentures. Yes, the teeth are not upright when viewed from the front (coronal) nor are they in a straight line when viewed from the side (sagittal). But why? If you understand that, hopefully after reading this, you will not refer to 'curves of Wilson, Monson, Spee' but to curves that compensate for the arcs of movements of the mandible: just coronal and sagittal compensating curves.
To work out how it all happens, we have to go back to how our teeth functioned whilst they were wearing down under natural conditions of eating unrefined, coarse and abrasive food. We first started with cusps, which helped guide the teeth to contact the opposing arch, because of two forces: a continuous eruption force, and a mesial vector of force which directs the eruptive force forwards. Both the eruptive force and alveolar bone growth continue throughout life, which may explain why our faces get longer if we don't wear our teeth down. 1 Natural (pre-refined foods) dentitions, such as in Fig. 1, show occlusal wear, but also, because of the mesial force vector, interproximal wear.
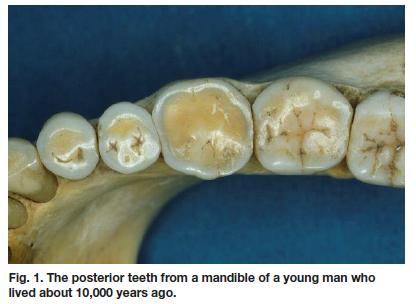
Note how flat the interproximal surfaces between the teeth are. All this was pointed out in 1954 already, when it was calculated that this wear is the equivalent of the mesio-distal width of a first molar;2 hence there is always room for the third molar. How many people do you know who have not had to have their third molars extracted because there was no room for them?
So as the dentition wore down under the effects of chewing, so then did the chewing gradually take place more evenly, and the forces became distributed throughout the arch. This applied to all teeth, including the incisors, so that the concept of an "intercuspal position" became pretty meaningless. Interestingly, the inclination of teeth helped this. To those of you who have been taught mechanistically, this may not make sense as it seems the wrong way round. The teeth are inclined not only because of the forces of eruption but also because this will create the best and most efficient pattern of wear, given the varied movements of the mandible, which are never in a straight line, but in a pattern under the control of the central pattern generator in the brainstem.
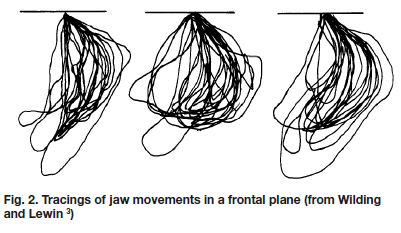
These patterns have been shown graphically by tracing either a point of light attached to the lower incisors, or electronically by tracing a magnet attached there.3 And they confirm that, the omnivores that we are, our mandibles have vertical and horizontal phases, closing mostly on one side, and then opening by moving to the other side. Fig. 2 shows tracings of jaw movements made by the same subject from three separate occasions in a frontal plane while chewing on the right side.
These movements, and the wear of the teeth, are also reflected in the adaptability of the joint itself, and in particular in the condyle of the mandible, which is capable of remodelling throughout life, as a necessary response to the changes occurring in the dentition: the faceting of the condyle has been correlated to the wear of the teeth in naturally worn dentitions. 4 This can also apply, though to a lesser extent, to the fossa,5 and the articular eminence can show a flattening with tooth wear.6
Understanding cusp angles and joint angles
It is somewhat ironic that, with our unworn dentitions, to understand how they end up with a pattern of tooth wear that provides contacts on both sides of the arch, which they do, and which the mechanistically oriented would be horrified to see (more of that later), dentists and dental technicians first learn how to construct complete dentures.
It is generally agreed that an even distribution of forces around the arch would assist in the stability of the dentures, especially mucosa-borne dentures, which exist by 'floating' on a layer of saliva over a surface of varying degrees of softness and sponginess. The challenge is to set the artificial teeth, whether with cusps or not, such that they will contact as much as possible at any reasonable position of the mandible, by compensating for the curving movements of the mandible. So I will try to explain this by means of a series of diagrams, which are re-drawn and based on a long-ago text book first published in 1976.7 We simplify the mandibular movements into a forward protrusive movement, and a lateral one.
Protrusive movements
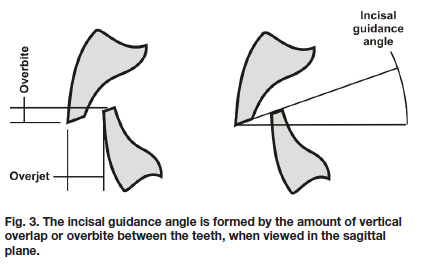
There are two determinants of mandibular movement in any forward direction, the incisal guidance angle and the sagittal condylar guidance angle. The incisal guidance angle (IGA) is formed by the vertical overlap (overbite) between the teeth (Fig. 3). It is only dependent on the amount of horizontal overlap (overjet) to the extent that there is no guidance until the teeth actually contact. In natural teeth, these dimensions of overbite and overjet are determined by the positions of the teeth; in complete dentures, they are determined by other factors, mainly aesthetics, phonetics, and function. This means they can be controlled by the dental technician and the dentist, within the limitations of the other factors that determine overall tooth position (mainly the need to achieve stability).
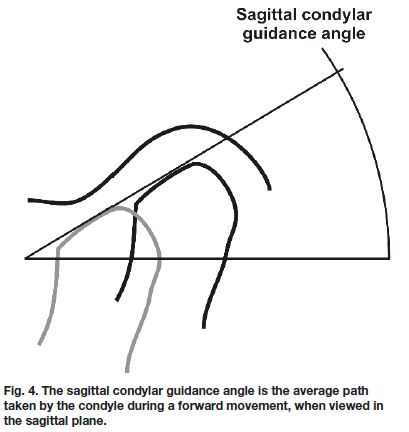
The sagittal condylar guidance angle (SCGA) (Fig. 4) is not under the control of the dentist at all, and is determined purely by the biomechanics of the joint itself. This is the net result of the condyle-disc assembly passing forwards and downwards, under the influence of the anterior slope of the glenoid fossa. As we have already discussed, the condyles do not traverse along a straight-line path as in the diagrams given here, but take a very shaky zig-zagging pathway, the net result of which can be represented by a somewhat artificial straight line as the difference between the starting and end points of the movement.
The form of the condyle and fossa means that any forward movement of the mandible is also a downward movement: if record blocks are placed midway between the incisors and condyles on a flat plane, they will separate if the mandible moves forwards. This is the so-called "Christensen phenomenon" (Fig. 5).
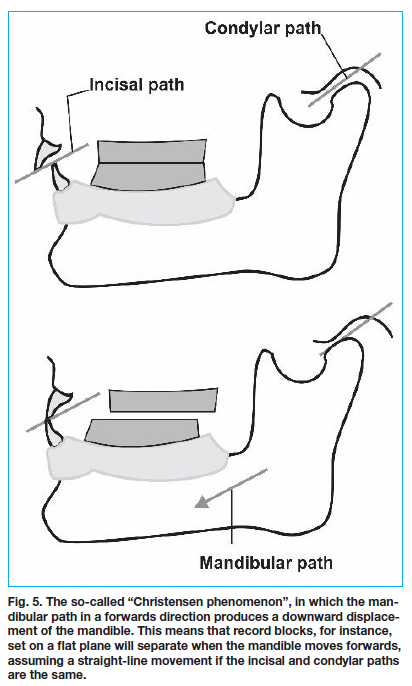
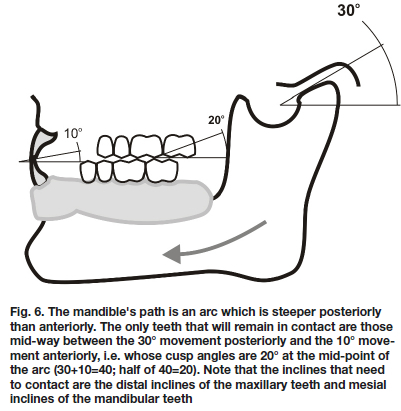
Now, if teeth are placed in place of flat record blocks, again on a flat plane, they will also separate, unless they can have inclines that may fit in with the geometry of the path of movement of the mandible. Fig. 5 is, though, misleading in that is shows a straight mandibular path, and we know it is not. It is also misleading in that it shows the same path for both incisors and condyles, and in reality these paths are not the same. The incisal guidance angle is less than the condylar guidance angle, so the average movement of the mandible under the influence of both of these will be a curve, that is steeper posteriorly than anteriorly. So if we are to set teeth, and they are to maintain contact in protrusion, they must be set in such a way that the inclines of their cusps will also vary and be shallower anteriorly and steeper posteriorly. But artificial teeth all have the same inclines or cusp angles (usually 20° or 33°). So if we set the teeth on the flat record block, the geometry of the situation means that most of the teeth will no longer contact. This is shown in Fig. 6 where the sagittal condylar guidance angle is 30° and the incisal guidance angle is 10° so only the teeth with cusp inclines of 20°half way between them would remain in contact.
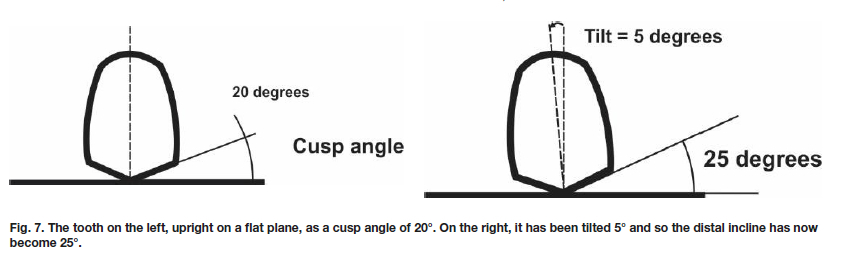
Now if you want all the teeth to contact, then those nearer to the condyle would need steeper inclines, and a tooth nearer the incisors would need shallower inclines. To change those angles, you would have to grind the teeth, but in such a way that they will be in harmony with the curve of movement of the mandible. Clearly this makes no sense, but interestingly, this is what happens in the natural dentition: as the teeth wear, they all contact in all movements. But back to the denture teeth: rather than grinding everything, you can change the angles of the cup inclines if you change the inclination of the whole tooth, as shown in Fig. 7.
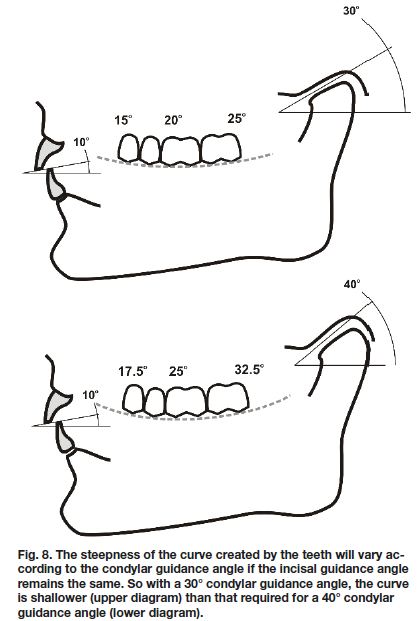
Back to the geometry: if steeper inclines are needed nearer the condyle, and shallower ones nearer the incisors, then the teeth nearer the condyle must be tilted to create that, and the teeth nearer the incisors need to be tilted in a different direction. If you do this, and join up the cusp tips, you will have created a curve that will allow the teeth to remain in contact, and therefore compensate for the curvature of the mandible as it moves forwards. This is shown very diagrammatically in Fig. 8.
You can call this compensating curve the "curve of Spee" if you want: the teeth are in positions that, if they are to remain in contact, must compensate for the curving movement of the mandible as it moves downwards and forwards. There are biomechanical advantages to this too, in terms of the efficiency with which occlusal forces are applied 8 and it is logical, given now our (your, I hope) understanding of natural teeth and tooth wear. It is entirely not logical to ascribe any other purpose to this curve as you may if you still think mechanistically, and as has been done even comparatively recently. 9
Lateral movements
These are a little more complicated, again because of the way the mandible moves sideways which, as you may have gathered by now, is also never a pure sideways movement in function, but includes forward and back movements during chewing. However, to understand how cusps must work if the teeth are to remain in contact, it is useful again to look at the edentulous situation and the need to have as many of the teeth contacting as possible.
As I am sure you know, when the mandible moves sideways, the side to which it moves is called the working side, and the opposite side of the arch, moving now towards the mid-line is the nonworking, or balancing side. The term "non-working" is also a misnomer and also steeped in the mechanistic theories that said that teeth should only contact on one side when the mandible moves sideways. This has been shown to be not the case, and is certainly not the case in natural, worn, dentitions, in which there are multiple contacts on both sides - which is what we need in complete dentures. It would be far better to refer to chewing and non-chewing sides which emphasises the function, as it appears that even in unworn dentitions (our 'modern' ones) there are contacts during chewing on both sides.10 This has been known, but largely ignored, for a long time.
But for now, I will try to use all the terms to make sure we are quite sure which side we are referring to. Consider a movement of the mandible to the left. As in protrusion, this movement is also not a flat one, but is under the influence of posterior and anterior determinants. The anterior determinant in this case will be any vertical overlap at the corners of the arch, i.e. at the canines. As with the incisal guidance angle, this canine guidance angle is under the influence of the operator but subject to the similar constraints of aesthetics, arch form, etc. The posterior determinant is, again, dependent on the anatomy of the joint, as the condyle-disc assembly now comes under the influence of the angulation of the medial wall of the glenoid fossa.
So, as it moves to the left, the left (working, chewing side) condyle hardly moves at all, and mostly seems to rotate. This makes the arc of movement of this side of the mandible shallow, influenced by the lateral wall of the left fossa (Fig. 9).

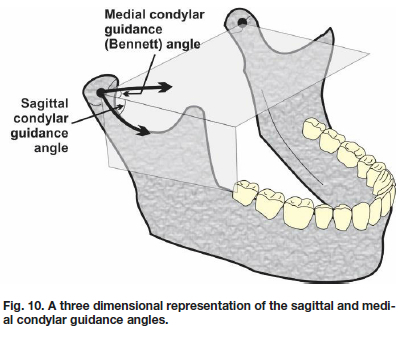
However, on the other side, the right (non-working, non chewing, balancing) side, the condyle has to move more downwards as well as sideways and is now under the influence of the medial wall of the fossa and the movement is therefore quite steep, or at least steeper than the other side. The average path taken is the medial condy-lar guidance angle, when viewed coronally, which is also referred to as the Bennett angle (after Norman Bennett who first described it in 1908 Fig. 10 shows this and the sagittal condylar guidance angle three-dimensionally.
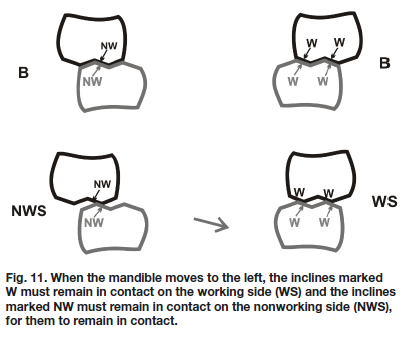
Precisely the same geometric principles as followed for protrusive movements can be used to explain the necessary changes in tooth morphology required to ensure tooth contact during these lateral mandibular movements. But first we must be sure we are referring to the correct inclines of the cusps, just as in protrusive we found that it was the distal inclines of the maxillary teeth and the mesial inclines of the mandibular teeth that needed to remain in contact. In lateral movements it gets a bit more complicated. Fig. 11 shows which inclines of which cusps must remain in contact.
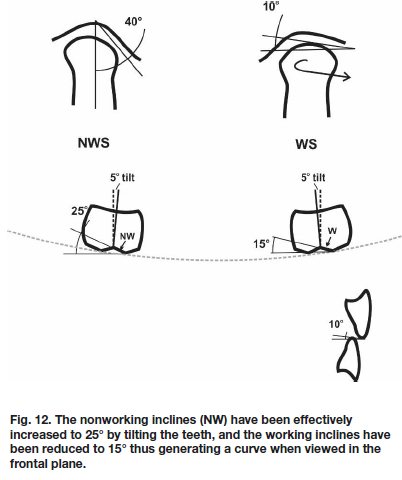
Using the geometry as before, because of the curved arc of movement, it means that the working (chewing) side inclines must be shallow, and the non-working (balancing, non-chewing) inclines must be steeper. So we have the same problem with denture teeth, in that all the inclines are the same. Is the solution the same? Yes, but only to a certain extent. Fig. 12 shows (again, very dia-grammatically) a medial condylar guidance angle of 40°, lateral condylar guidance of 10° and a canine guidance angle of 10°. So half way, as we did with protrusion, we need to increase the angle of the non-working cusp inclines, and decrease the angle of the working cusp inclines and we do that by tilting the teeth relative to a horizontal plane to make the non-working inclines steeper and the working side inclines shallower.
And lo and behold, we have another curve! The tilt of the teeth are again compensating for the curvature of the arc of movement of the mandible. You can call this the curve of Wilson or Monson if you like.
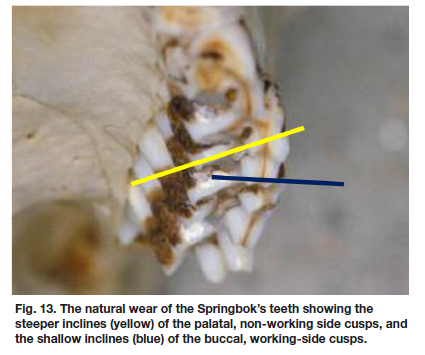
There's only one problem though, when it comes to complete dentures and that is that the tilt that provides steeper non-working (balancing, non-chewing) inclines doesn't really make the working side inclines shallow enough, as any dental student and dental technologist will tell you as they find it impossible to produce full balance without having to grind those working side inclines. It might be easier to understand if we look again at the animal kingdom, and those chewers par excellence, the herbivores. Fig. 13 is the maxillary dentition of a Springbok (the antelope which has become the symbol of South African Rugby). The yellow line Is against the Inclines of the palatal cusps, which are the non-working cusps, and the blue line is against the incline of the buc-cal, working-side cusp.
This difficulty is the reason that alternative methods have emerged to provide a balanced articulation in complete dentures, although the evidence for the absolute need for this has been challenged by some short-term studies with few patients in which lateral contacts were provided only on the canines.12 The patients adapted, but in doing so experienced much more ulceration and worse maxillary denture retention than with the occlusally balanced dentures, which a moment's thought would show to be logical, because the dentures would be moving around considerably. Not necessarily when chewing, but certainly if the patient has any parafunctional habits like clenching and grinding.
So there have emerged other schemes, and my preference is that of lingualised occlusion for complete dentures, as there is now evidence that patients may prefer this over other schemes,13-15 and it is in fact much easier to set up and adjust for both the dental technician and the dental clinician. A full explanation is available at www. appropriatech.com. 16
REFERENCES
1. Tallgren A. Changes in adult face height due to ageing, wear and loss of teeth and prosthetic treatment. Acta Odontol Scand 1957; 15(Suppl 4): 73 [ Links ]
2. Begg PR. Stone age man's dentition: With reference to anatomically correct occlusion, the etiology of maloc-clusion, and a technique for its treatment. Am J Orth-od. 1954; 40(4): 298-312 [ Links ]
3. Wilding RJ, Lewin A. A computer analysis of normal human masticatory movements recorded with a sirog-nathograph. Arch Oral Biol. 1991; 36(1): 65-75. doi:10.1016/0003-9969(91)90055-y. [ Links ]
4. Owen CP, Wilding RJC, Osborn JW. Changes in mandibular condyle morphology related to tooth wear in a prehistoric human population. Archives of Oral Biology, 1991; 36(11): 799-804. doi: 10.1016/0003-9969(91)90029-t. [ Links ]
5. Owen CP, Wilding RJC, Adams LP. Dimensions of the temporal glenoid fossa and tooth wear in prehistoric human skeletons. Archives of Oral Biology, 1992; 37(1): 63-67. doi: 10.1016/0003-9969(92)90154-z. [ Links ]
6. Granados JI. The influence of the loss of teeth and attrition on the articular eminence. J Prosthet Dent 1979; 42(1): 78-85. doi: 10.1016/0022-3913(79)90333-0. [ Links ]
7. Watt DM, MacGregor AR. Designing complete dentures. WB Saunders, Philadelphia. 1976. [ Links ]
8. Osborn JW. Orientation of the masseter muscle and the curve of Spee in relation to crushing forces on the molar teeth of primates. Am J Phys Anthropol. 1993; 92(1): 99-106. doi: 10.1002/ajpa.1330920108. [ Links ]
9. Xu H, Suzuki T, Muronoi M, Ooya K. An evaluation of the curve of Spee in the maxilla and mandible of human permanent healthy dentitions. J Prosthet Dent. 2004; 92(6): 536-9. doi: 10.1016/j.prosdent.2004.08.023 [ Links ]
10. Woda A, Vigneron P, Kay D. Nonfunctional and functional occlusal contacts: a review of the literature. J Pros-thet Dent 1979; 42(3): 335-341 doi: 10.1016/0022-3913(79)90226-9. [ Links ]
11. Bennett NG. A Contribution to the Study of the Movements of the Mandible. Proc R Soc Med. 1908;1(Od-ontol Sect):79-98. Reprinted in J Prosthet Dent 1958; 8(1): 41-54 [ Links ]
12. Peroz I, Leuenberg A, Haustein I, Lange KP. Comparison between balanced occlusion and canine guidance in complete denture wearers-- a clinical, randomized trial. Quintessence Int. 2003; 34(8): 607-12. PMID:14620212. [ Links ]
13. Clough H.E., Knodle J.M., Leeper H.L., Pudwill M.L. and Taylor D.T. (1983): A comparison of lingualized occlusion and monoplane occlusion in complete dentures. J Prosthet Dent 1983; 50: 176-179. [ Links ]
14. Sutton AF, McCord JF. A randomized clinical trial comparing anatomic, lingualized, and zero-degree posterior occlusal forms for complete dentures. J Prosthet Dent. 2007;97(5):292-8. Erratum in: J Prosthet Dent. 2007; 98(1): 16. [ Links ]
15. Loh PJ, Levey C. Occlusal schemes for complete dentures. Evid Based Dent 2018; 19(4): 116-117. doi: 10.1038/sj.ebd.6401346. [ Links ]
16. Owen CP. Lingualised Occlusion. An eBook module. Available at www.appropriatech.com [ Links ]
 Correspondence:
Correspondence:
CP Owen
Professor Emeritus, Faculty of Health Sciences
University of the Witwatersrand Johannesburg
South Africa
Cell: +27 83 679 2205
Email: peter.owen@wits.ac.za


{kind=link}