










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.76 no.10 Johannesburg Nov. 2021
http://dx.doi.org/10.17159/2519-0105/2021/v76no10a6
RESEARCH
http://dx.doi.org/10.17159/2519-0105/2021/v76no10a6
The referral system for specialist dental services at Sefako Makgatho Oral Health Centre: a cross-sectional study
SR MthethwaI; KJ RamphomaII
IBDS, MPH, PhD. Sefako Makgatho Health Sciences University. ORCID Number: 0000-0003-0420-808X
IIBChD, MChD. Sefako Makgatho Health Sciences University. ORCID Number: 0000-0001-9975-2912
ABSTRACT
BACKGROUND: The functioning of various referral systems in service delivery at district level have been described.
AIMS AND OBJECTIVES: To examine the functioning of referral system for specialist dental services at Sefako Makgatho Oral Health Centre. The prevalence of self-referrals and emergency patients and reasons for referrals were determined. The pattern of referrals for elective treatment at the clinical units was described.
DESIGN: This was a cross-sectional study.
METHOD: A structured closed questionnaire was used to collect data related to demographic characteristics, reasons for referrals to the clinic and whether patients were referred by healthcare workers or self-referred. Patients themselves or with the assistance of the research team completed the questionnaire. Data required for classifying patients into emergency and non-emergency was gathered from the service register. The classification was made based on the referral preferences of attending clinicians.
RESULTS: A substantial proportion of visitors to the hospital were self-referred (71.3%), emergency patients (69.7%). Among referred patients, the most common reason for referrals was for specialist oral and maxillofacial surgical services. The majority (64.7%) of hospital visitors received elective treatment referrals, 48.9% of which were for general dentistry.
CONCLUSION: The prevalence of self-referrals by emergency patients is extremely high.
Literature review
A hierarchical referral system is followed in the public health sector in South Africa.1 The functioning of various referral systems in service delivery at district level have been described.1-3 Very little was found in the literature concerning referral systems and dentistry. A recent national health care facilities audit found that dental services are lacking across the board at primary health care level in South Africa.4 High attendance rates were reported where services were available and accessible.5,6 However, the range of services offered was often limited to emergency treatment of pain and sepsis.7 A compliance audit performed in the district of Umgungundlovu in the province of KwaZulu-Natal found that none of the clinics were compliant with the national set of norms, standards and practice guidelines for primary oral health care.8
Sefako Makgatho University Oral Health Centre (SMU Oral Health Centre), a dental school and a comprehensive care referral hospital in the outskirts of Pretoria, is one of two public tertiary care facilities, which are part of an oral healthcare network that includes thirty-three community health clinics, in the Tshwane district.9 Referral systems for specialist dental services operate between the tertiary care facilities and community oral health/ medical services. Appropriate and timely referral is an essential part of a functioning health system.10,11 A well-functioning referral system allows for continuity of care across the different levels of care.12 It ensures that all citizens have access to the highest possible standard of health irrespective of where they access care in the health system.13 Factors such as accessibility, acceptability, efficiency and effectiveness have been identified as influential in the use of a referral system.14-16
At SMU Oral Health Centre new and repeat self-referred and referred patients routinely move between the diagnostic unit, a screening and referral clinic, where experienced dentists examine them and clinical units where dental students under faculty supervision provide treatment or treatment appointments are scheduled.
Emergency patients are triaged based on the severity of their illness, injury or pain and referred to emergency clinics. The attending dentist determines the appropriate treatment and referral options.
• Facial swelling, bleeding (trauma affecting the mouth), an accident involving damage to the mouth or teeth, or dental pain are referred to Minor Oral Surgery/ Maxillofacial and Oral Surgery.
• Restorative emergencies, dental pain and injuries to teeth and the pulp are referred to Care line clinic.
Multiple problems are also assessed. They are however not addressed in emergency appointment -referrals are made to elective clinics at that time. At emergency clinics, the dentist will aim to reduce or stop the pain experienced. Emergency clinics can make referrals to elective clinics. Prosthodontics emergencies are referred to the prosthodontics clinic.
Patients with less urgent problems are referred for general dental care and or for initial assessment in the relevant specialty clinics. They are placed on a waiting list for care and are informed when a booking becomes available.
General dental examinations and care is offered through oral hygiene, minor oral surgery and operative dentistry clinics. This dental service includes routine dental examinations or check-up, oral health advice, scale and polish, extractions, Allings, Assure sealants and root canal treatments.
Referrals for specialist dental services from community oral health / medical services also pass through the diagnostic unit. Specialist dental care is often provided as part of a treatment plan in combination with other specialty clinics.
A recent review of the functioning of referral system that operates between the diagnostic unit and clinical units found it to be inefficient - the average time lapse between consultation at the diagnostic unit and receipt of treatment in clinical units was 81.2 days with a range of just under a week (6 days) to longer than six months (184.5 days). It was also found that patients who presented for emergency treatment constituted 60% of referred patients.17
A sharp increase in the numbers of patients who present at the diagnostic unit has been observed - 1209 patients consulted in February 201317 compared with 1645 in February 201818. The increase in patients' numbers warranted a study of the effectiveness of the referral system between SMU Oral Health Centre and community oral health/ medical services with a focus on the divide between self-referred and referred patients.
OBJECTIVES OF THE STUDY
• To describe the socio-demographic characteristics of patients who consulted at the diagnostic unit of SMU Oral Health Centre between February and April 2019.
• To determine the prevalence of self-referrals.
• To determine the proportions of emergency and non-emergency patients.
• To describe the pattern of referrals for elective treatment at the clinical units.
• To determine the reasons for referrals between community oral health clinics and SMU Oral Health Centre.
MATERIALS AND METHODS
Study design
This was a cross-sectional study. Target population
The sampling frame consisted of all patients who consulted at the diagnostic unit of SMU Oral Health Centre between February and April 2019.
Study sample
The ideal sample size was estimated at 300 in Epi Info Version 7.1.0.6 software19 at the confidence interval of 95% and absolute precision of 5% assuming emergency patients comprise 60% of the total population of 1600.
Sampling method
A systematic random sample was selected i.e. a list of the entire population using hospital registration numbers was prepared in Excel; the sample size of 300 was divided into the total population (1600) to calculate the Kth number (5). A random starting point was selected (a number between 1 and 5). Every fifth person on the list will be selected from the random starting point.20
Data collection
A structured closed questionnaire was used to collect data related to demographic characteristics, reasons for referrals to the clinic and whether patients were referred by healthcare workers or self-referred. Patients themselves or with the assistance of the research team completed the questionnaire. Data required for classifying patients into emergency and non-emergency was gathered from the service register of the diagnostic unit. The classification was made based on the referral preferences of attending clinicians.
Definition of variables
Emergency patients are those who consulted at the diagnostic unit with an issue involving teeth and supporting tissues that was fixed/treated at the emergency clinics.
Emergency clinics are clinics where emergency oral and dental treatment is offered. They include the Minor Oral Surgery (MOS), Maxillofacial and Oral Surgery (MFOS), and Care line clinics.
Care line clinic is an emergency clinic where restorative emergencies, prosthodontics emergencies, dental pain and injuries to teeth and the pulp are treated.
Non-emergency patients are those who consulted at the diagnostic unit with less urgent problems, and were placed on a waiting list for care.
DATA ANALYSIS
Data was captured, coded and cleaned in Microsoft Excel software and then transferred to Statistical Package for the Social Sciences (SPSS) software for analysis. Frequencies, means and proportions were calculated. Bivariate analyses were performed. The significance level of the test was a p-value less than 0.05.
Ethical considerations
Only patients who provided informed consent were enrolled. All data collection and analysis and reporting was done without any personal identifiers. Patients had the opportunity to refuse participation at any time without any repercussion. Ethical approval for the study was granted by the Ethics Committee of Sefako Makgatho Health Sciences University (SMREC/D/309/2018). Permission to conduct the study was granted by the Chief Executive Officer (CEO) of SMU Oral Health Centre.
RESULTS
Data of a systematic random sample of 300 patients was analysed. A response rate of 100% was obtained.
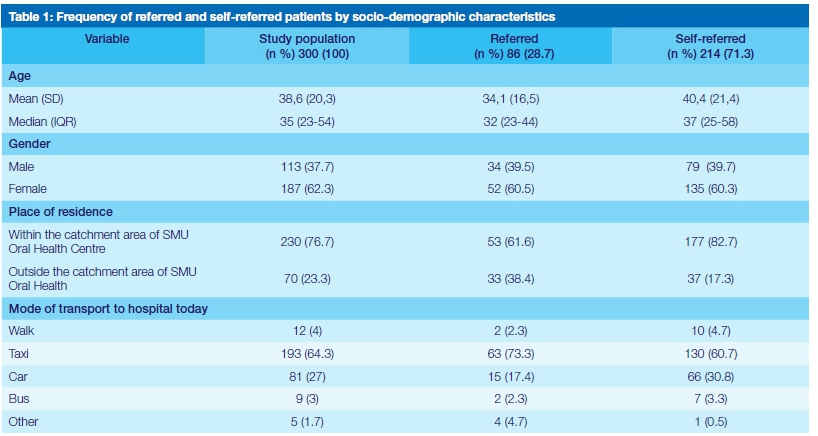
Less than thirty percent (28.7%) of patients who visited SMU Oral Health Centre were referred. The median age of the study sample was 35 years with an interquartile range of 23 to 54 years. Referred patients were younger than self-referred patients (32 vs 37 years).
Female patients constituted the majority of the study sample (62.3%), referred patients (60.5%) and self-referred patients (60.3%). The overwhelming majority (>75%) of patients resided within the catchment area of SMU Oral Health Centre. A little less than two-thirds (64.3%) of patients used taxis to get to the hospital.
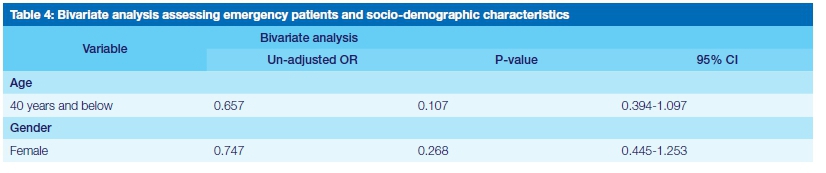
The odds of patients forty years of age and younger referring themselves were significantly lower than that for older patients. The odds of female patients referring themselves were higher than that for male patients. The increased odds were not, however, statistically significant.
A little less than seventy percent (69.7%) of patients who visited SMU Oral Health Centre were emergency patients. The median age of emergency patients was Ave years older than that of nonemergency patients (36 vs 31 years). The proportion of female emergency patients was 20.6% higher than the proportion of male patients. The odds of patients forty years of age and younger being emergency patients were lower than that for older patients. The decreased odds were not, however, statistically significant.
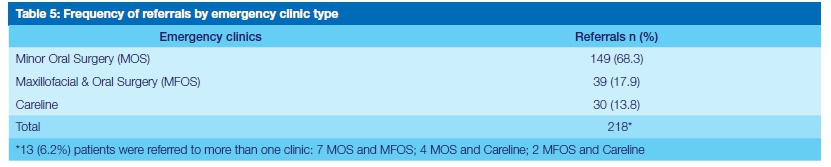
The odds of female patients being emergency patients were lower than that for male patients. The decreased odds were not, however, statistically significant. A little more than two-thirds (68.3%) of all emergency patients visited the Minor Oral Surgery clinic. Slightly more (4%) more patients visited the Maxillofacial and Oral Surgery clinic than the Careline clinic.
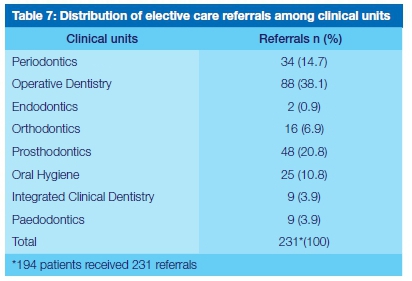
A little less than two-thirds (64.7%) of the study subjects received elective treatment referrals. Emergency patients accounted for 66% (128/194) of the referrals. The majority (51.3%) of referrals were to one clinical unit. In contrast, a little more than a tenth (13.3%) of the referrals were to multiple clinical units.
Just less than forty percent (38.1%) of all referrals were to the Operative Dentistry clinic. The second largest number of referrals (20.8%) were to the Prosthodontics clinic. The Periodontics and Oral Hygiene clinics together accounted for 25.5% of referrals. Fewer patients were referred to the Orthodontics (6.9%), Integrated Clinical Dentistry (3.9%), Paedodontics (3.9%) and Endodontics (0.9%) clinics respectively.
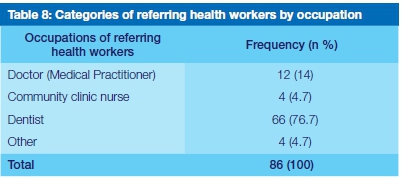
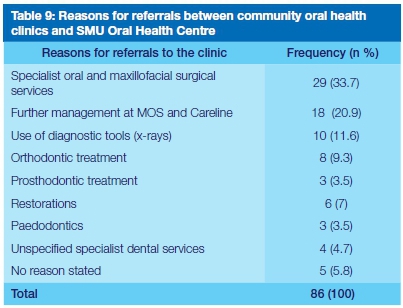
Just over three-quarters (76.7%) of all referrals were made by dentists. A significant number were made by medical practitioners. Treatment at the Maxillofacial and Oral Surgery clinic was the most common reason for referrals. Further management at the Minor Oral Surgery and Careline clinics was the reason for a fifth (20.9%) of referrals. The use of diagnostic tools constituted a significant proportion (11.6%) of referrals. Orthodontic treatment accounted for less than a tenth (9.3%) of the referrals
Referral related statistics
Number of referred patients who presented at SMU Oral Health Centre with referral letters: An overwhelming majority (89.5%) of referred patients produced referral letters. Number of referred patients who understood the purpose of their referral: An overwhelming majority (90.7%) of referred patients understood the purpose of their referral. Number of referred patients who were instructed to return for ongoing management after referred services at SMU Oral Health Centre: Only a tenth (10.5%) of referred patients were instructed to return for ongoing management after referred services at SMU Oral Health Centre.
DISCUSSION
This study set out to investigate the functioning of the referral system that operates between SMU Oral Health Centre and community oral health/ medical services.
Socio-demographic characteristics
The results of this study indicate that more women than men (62.3% female vs 37.7% male) visited SMU Oral Health Centre and that the average age of the study sample was 35 years with an interquartile range of 23 to 54 years (Table 1). The present findings seem to be consistent with other research which found a large female preponderance at dental clinics.7,21 The age structure of the study population is consistent with that described by Lesolang and colleagues.7 The results of this study show that the overwhelming majority (>75%) of patients resided within the catchment area of SMU Oral Health Centre and that a little less than two-thirds (64.3%) used taxis to get to the hospital (Table 1). These results are very encouraging for the reason that it is preferable for a patient to be seen at the hospital that corresponds to the patient's catchment area.
Prevalence of self-referrals
The current study found that a little more than seventy percent (71.3%) of patients who visited SMU Oral Health Centre were self-referred and that their average age was 37 years old (Table 1). This result has not previously been described - comparable studies were not found. However, it is significantly higher than the range (35-36%) of prevalence reported at general hospitals in Kwa-Zulu Natal.22,23 The findings of Masango-Makgobela and colleagues' (2013) study of reasons patients, from the catchment area of SMU Oral Health Centre, leave their nearest healthcare service might explain this result.24
They found that 19% of patients who had visited their nearest clinic previously said they would not return. The reasons for this were: long waiting time; long queues; rude staff; and no medication.24 Considering the number of community health clinics (33) in the Tshwane district, this finding was unexpected. The fact that data was collected during the school term accounts for the high average age of the patients. The most interesting finding was that patients older than forty years of age were more likely to self-refer (Table 2). This result is in contrast to earlier findings at general hospitals in Kwa-Zulu Natal.22,23
The current study found that female patients were more likely to self-refer (Table 2). The findings of the current study do not support the previous research at general hospitals in Kwa-Zulu Natal where it was found that the majority of self-referred patients were male.22,23
A significant number of referrals were made by medical practitioners. This finding was unexpected and suggests that dental services are lacking at some community clinics.
The results of this study indicate that an overwhelming majority (90.7%) of referred patients understood the purpose of their referral and produced referral letters. These results are very encouraging.
The results of this study indicate that only a tenth (10.5%) of referred patients were instructed to return for ongoing management after referred services at SMU Oral Health Centre. This finding is rather disappointing. It raises questions about how health providers keep track of their patient referrals throughout the care continuum.
Treatment at the Maxillofacial and Oral Surgery clinic was the most common reason for referrals. There are several possible explanations for this result. Coulthard and colleagues (2000) found that the most common reasons for general dental practice referral to specialist oral and maxillofacial surgical services were the expected difficulty of the operation, the medical condition of the patient and the lack of facilities for general anaesthesia.25 The most interesting finding was that the use of diagnostic tools accounted for just over a tenth of referrals. This finding was unexpected and suggests that some community dental clinics are not fully equipped.
Proportions of emergency and non-emergency patients
The results of this study indicate that a little less than seventy percent (69.7%) of patients who visited SMU Oral Health Centre were emergency patients (Table 3). This finding supports the previous research, which found that emergency patients comprised 59.7% of patients who consulted at the diagnostic unit of SMU Oral Health Centre.17 However, the ten percent increase in the proportion of emergency patients within 5 years indicates that symptomatic dental attendance continues to be a problem. An implication of this is that the referral system that operates between SMU Oral Health Centre and dental clinics in the Tshwane health district is not effective.
Men were more likely to be emergency patients (Tables 3 and 4). These results differ from previous research by Mthethwa and Chabikuli (2016) which found that female patients constituted 56.8% of emergency patients.17 Considering the gender distribution of patients in this study (62.3% female vs 37.7% males), it is difficult to explain this result. It is made even more so by the evidence which associates female gender with dental consultations motivated by pain.26 Further research should be done to investigate this finding.
Patients older than forty years of age were more likely to be emergency patients (Table 4). This finding is in agreement with Nazir's (2018) findings which showed that age over 35 years was a significant factor associated with dental consultations motivated by pain among adult patients.26
The majority (68.3%) of emergency patients were referred for elective treatment. The present findings are consistent with earlier findings, which showed that 68.2% of emergency patients required elective treatment.17
The current study found that a little more than two-thirds (68.3%) of all emergency patients visited the Minor Oral Surgery clinic. It is encouraging to compare this figure with that found by Mthethwa and Chabikuli (2016) who found that 79.5% of emergency patients in their study visited the Minor Oral Surgery clinic.17 The current study however produced results which corroborate the findings of a great deal of the previous work in this field i.e. a large number of self-referred emergency patients inappropriately utilising the service for basic curative services i.e. extractions, which could be satisfactorily provided at primary care facilities where available.
The bulk (58.9%) of the referrals were to the Operative Dentistry and Prosthodontics clinics (Table 7). The large number of patients who require general dental care observed in this study reflects the high levels of untreated dental caries reported in studies of dental caries prevalence in South Africa.27,28
Limitations of the study
Patient awareness of the referral policy was not investigated.
CONCLUSION
The prevalence of self-referrals to SMU Oral Health Centre by emergency patients is extremely high.
References
1. Mojaki ME, Basu D, Letskokgohka ME, Govender M. Referral steps in district health system are side-stepped. S Afr Med J. 2011; 101(2):109. [ Links ]
2. Ncana L. Evaluating the referral system between CEC ILIA MAKHIWANE HOSPITAL ART unit andits feeder sites, (Zone 2, 8 and 13 clinics 2010). [Masters Thesis]. Stellenbosch University, 2010. [ Links ]
3. Mashishi MM. Assessment of Referrals to a District Hospital Maternity Unit South Africa. [Masters Thesis]. University of the Witwatersrand, 2010. [ Links ]
4. Visser R, Bhana R, Monticelli F. National Health Care Facilities Baseline Audit, National Summary Report September 2012 Revised February 2013, Health Systems Trust. Available: www.doh.gov.za/docs/reports/2013/Healthcare.pdf [Accessed 23/07/2018]. [ Links ]
5. Bhayat A, Cleaton-Jones P. Dental clinic attendance in Soweto, South Africa, before and after the introduction of free primary dental health services. Community Dent Oral
Epidemiol 2003; 31(2): 105-10.
6. Harkinson BN, Cleaton-Jones PE. Analysis of attendance rates at Soweto dental clinics 1995-2002. S Afr Dent J 2004; 59(4): 147-9. [ Links ]
7. Lesolang RR, Motloba DP, Lalloo R. Reasons for tooth extraction at the Winterveldt Clinic: 1998-2002. S Afr Dent J 2009; 64:214-8. [ Links ]
8. Rajcoomar N. Compliance of public dental clinics in the Umgungundlovu district with norms and standards in the Primary Health Care Package for South Africa. [Masters Thesis]. University of the Western Cape, 2016. [ Links ]
9. Gauteng Department of Health. Oral Health Clinics Tshwane District. Available: http://www.gauteng.gov.za/Document%20Library/Health/Tshwane%20district%20Clinics.pdf Accessed [23/07/2018] [ Links ]
10. Naidoo S. Referrals - practitioner, patient & specialist obligations. SADJ 2016; 71(2):82- 4. [ Links ]
11. Rohde J S, Cousens M. Chopra, V et al. "30 Years After Alma-Ata: Has Primary Care Worked in Countries?" Lancet 2008; 372: 950-61. [ Links ]
12. Kamau KJ, Osuga BO, Njuguna S. Challenges Facing Implementation Of Referral System For Quality Health Care Services In Kiambu County, Kenya. Health Research Policy and Systems 2017; 4:1 [ Links ]
13. Ministry of Health - Harambee. Frequently Asked Questions (Faqs). Available: https://www.measureevaluation.org/pima/referral-systems/referral-faqs-insert Accessed [23/07/2018] [ Links ]
14. Hensher M, Price M, Adomakoh S. Referral Hospitals. In: Jamison DT, Breman JG, Measham Ar, et al., editors. Disease control Priorities in Developing countries. 2nd edition. Washington (Dc): World Bank; 2006. [ Links ]
15. Akande TM. Referrals system in Nigeria: Study of a tertiary health facility. Annals of African Medicine 2004; 3(3):130-3. [ Links ]
16. Formicola AJ, Myers R, Hasler JF et.al. Evolution of dental school clinics as patient care delivery centres. Journal of Dental education 2006; 72(2) Supplement: 110-7. [ Links ]
17. Mthethwa SR, Chabikuli NJ. The efficiency of the referral system at Medunsa Oral Health Centre. SADJ 2016; 71(10):448 - 53 [ Links ]
18. Medunsa Oral Health Centre. Diagnostic clinic patient attendance register, 2018 [ Links ]
19. Epi Info [program]. 7.1.0.6 version, 2012.
20. INDIANA UNIVERSITYBLOOMINGTON. Sampling & How to Use a Random Number Table. Available: http://www.indiana.edu/~educy520/sec6342/week_04/random_ num_table.pdf Accessed [05 /07/2018] [ Links ]
21. Singh AS, Mohamed A, Bouckaert MM. A clinical evaluation of dry sockets at the Medunsa Oral Health Centre. South African Dental Journal 2008; 63(9):490-3. [ Links ]
22. Pillay I, Mahomed OH. Prevalence and determinants of self-referrals to a District-Regional Hospital in KwaZulu Natal, South Africa: a cross sectional study. Pan Afr Med J. 2019; 33:4. [ Links ]
23. Rajman, A, Mahomed O. Prevalence and determinants of self-directed referrals amongst patients at hospitals in eThekwini District, KwaZulu-Natal 2015. South African Family Practice 2019; 61(2), 52. [ Links ]
24. Masango- Makgobela, Agnes, Indiran Govender, & John V. Ndimande. Reasons patients leave their nearest healthcare service to attend Karen Park Clinic, Pretoria North. Afr J Prim Health Care Fam Med 2013;5(1):559 [ Links ]
25. Coulthard P, Koron R, Kazakou I, Macfarlane TV. Patterns and appropriateness of referral from general dental practice to specialist oral and maxillofacial surgical services. Br J Oral Maxillofac Surg. 2000;38(4):320-5 [ Links ]
26. Nazir MA. Factors associated with dental pain related to last dental visit among adult patients. Dental and Medical Problems. 2018 ;55(1):63-8. [ Links ]
27. Singh S. Dental caries rates in South Africa: implications for oral health planning. South Afr J Epidemiol Infect 2011; 26(4) (Part II): 259-61. [ Links ]
28. Bhayat A, Chikte U. Human Resources for Oral Health Care in South Africa: A 2018 Update. Int J Environ Res Public Health. 2019;16(10):1668. [ Links ]
 Correspondence:
Correspondence:
Dr SR Mthethwa: Medunsa Campus, PO Box D24
Sefako Makgatho Health Sciences University 0204
Tel: 012 521 5888 Fax: 012 512 4274
Email: rocky.mthethwa@smu.ac.za
Author contributions:
1 . Dr SR Mthethwa: conception; design; acquisition of data; analysis and interpretation of data; drafting the article
2 . Dr KJ Ramphoma: conception; acquisition of data and revising the article critically for important intellectual content


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}