










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.76 n.10 Johannesburg Nov. 2021
http://dx.doi.org/10.17159/2519-0105/2021/v76no10a7
REVIEW
http://dx.doi.org/10.17159/2519-0105/2021/v76no10a7
A Review of the role of Nuclear Medicine Imaging in Diagnostic Dentistry
S Rajbaran SinghI; AA GuttaII
IMSc.Odont, Dip.Odont, BChD, Department of Maxillofacial and Oral Radiology, School of Oral Health Sciences, Sefako Makgatho Health Sciences University, Ga-Rankuwa, Pretoria, South Africa. Telephone: (012) 521 4902 Email: sandeepa.singh@smu.ac.za, ORCID: 0000-0002-7313-1365
IIMBChB, M.Med (Nuclear Medicine), FCNP (SA). Department of Nuclear Medicine, Sefako Makgatho Health Sciences University/ Dr George Mukhari Academic Hospital, Ga-Rankuwa, Pretoria, South Africa. Telephone: (012) 521 4626 Fax: (012) 521 4604. Email: aadil.gutta@smu.ac.za, ORCID: 00000002-7342-5419
ABSTRACT
The increasing scope of nuclear medicine imaging as a diagnostic utility is impressive. Plain film radiographs, computed tomography (CT) scans and magnetic resonance imaging (MRI) diagnostically provide high-quality images but provide little physiological information about disease processes. Nuclear medicine imaging modalities advantageously can characterise the early dynamic physiological changes in a diseased environment. Dental professionals working within the arena of integrated holistic health practices are likely to encounter patients having had procedures like conventional scintigraphy, single photon emission computed tomography (SPECT), hybrid SPECT/CT and positron emission tomography computed tomography (PET/CT). The aim of this review is to acquaint the oral health care professional with some commonly utilised nuclear medicine techniques, the principles upon which such modalities are based and their applications in the diagnosis of head and neck pathology to facilitate enhanced multidisciplinary patient management.
Key words: Nuclear medicine, Dentistry, Head and neck, Positron emission tomography (PET), Single photon emission computed tomography (SPECT), Bone scintigraphy, Lymphoscintigraphy, Hybrid imaging.
INTRODUCTION
With chronicled contributions from the diverse fields of medicine, physics, chemistry, engineering, and mathematics the scope of nuclear medicine is impressive. While extensively used in medical healthcare, the optimal utilisation of nuclear medicine in dentistry remains yet to be widely appreciated. Plain film radiographs, computed tomography (CT) scans and magnetic resonance imaging (MRI) diagnostically provide high-quality images but provide little physiological information about the disease process. Nuclear medicine imaging modalities advantageously can characterise the early dynamic physiological changes in a diseased environment. The application of procedures like conventional scintigraphy, single photon emission computed tomography (SPECT), hybrid SPECT/CT and positron emission tomography computed tomography (PET/CT) in the contemporary diagnostic arena justifies the need for an overview of the utility of nuclear medicine in diagnostic dentistry.
The aim of this review is to acquaint the oral health care professional with some commonly utilised nuclear medicine techniques in the diagnosis of head and neck pathology to facilitate enhanced multidisciplinary patient management.
Nuclear medicine is an independent medical speciality that makes use of radioactive compounds (radiopharmaceuticals) to diagnose and treat disease. Radiopharmaceuticals consist of two chemically bound components, a radioisotope and a tracer. The radioisotope undergoes radioactive decay and is responsible for the diagnostic (photon emission) or therapeutic (particle emission) effect. The tracer targets an organ or metabolic process via a physiological mechanism. In the presence of disease, the tracer will be bio-distributed or metabolised differently. Following administration of the radiopharmaceutical (usually via intravenous injection), gamma rays are emitted from the targeted organ within the patient and are detected by external detectors in the form of gamma or PET cameras. This form of 'emission imaging' is advantageous as it allows for whole-body imaging from a single radiation exposure, with the resultant ability to detect clinically and/or radiologically occult loco-regional and distant disease. Currently, hybrid or multimodality cameras are typically installed in the form of SPECT/CT, PET/CT, and more recently, PET/MRI. Post-acquisition, the anatomical and physiological images are viewed independently and superimposed as 'fused' multi-planar reconstructions. Hybrid imaging provides the 'best of both worlds', combining the high sensitivity of physiologic imaging with localisation and tissue characterisation from the anatomical component. Scintigraphy, SPECT, and PET are established physiological imaging modalities that are principled on the bio-distribution, normal physiological uptake and pathophysiological behaviour of specific radiopharmaceuticals.
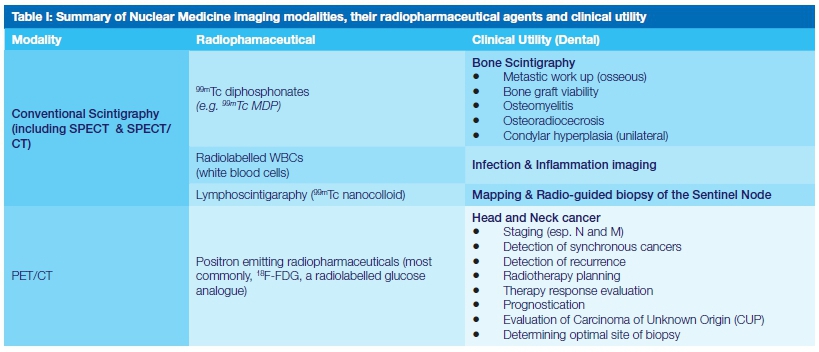
Bone Scintigraphy
While CT and MRI have evolved as excellent tools for the evaluation of bone pathology, bone scintigraphy continues to be the second greatest volume nuclear imaging procedure.1 Characterised by time efficiency, reasonable affordability, wide availability and high sensitivity, scintigraphy is an invaluable diagnostic tool that offers the advantage of total body examination, with a single radiation exposure to the patient. Whole-body imaging facilitates the detection of clinically and/ or radiologically occult bony pathology. Scintigraphic images are obtained following the intravenous administration of technetium9*" ("mTc) labelled diphosphonates.
The radiopharmaceutical circulates through the bloodstream and is either incorporated into areas of active bone metabolism or excreted via the urine. Approximately 2-6 hours after administration about half of the injected dose is localised in the skeletal system.2 The precise mechanism by which the labelled diphosphonates are incorporated into bone remains yet to be elucidated. Bone is continuously remodelled through bone resorption (osteoclastic activity) and bone deposition (osteoblastic activity). Osteoblasts produce an osteoid matrix that is subsequently mineralised with hydroxyapatite crystals. It is thought that the radiolabelled diphosphonates chemisorb and bind to hydroxyapatite crystals in proportion to local blood flow and osteoblastic activity.
Characterised by rapid localisation to bone and a short half-life the diphosphonates are therefore favourable markers of bone turnover and bone perfusion.3 Lesions can be detected when there is a 5-10% change in bone turnover and the diagnostic value of bone scintigraphy can thus be appreciated when one considers that between 30-50% of alteration to bone content is necessary for detection on conventional radiographs.4 The high sensitivity does however come at the expense of specificity. Any pathology invoking an osteoblastic response such as infection, inflammation, primary or secondary tumours, metabolic bone disease, or trauma will manifest as increased uptake on a bone scan. Fortunately, in the vast majority of cases, a definitive diagnosis can often be made based on a clinical-pathological correlation. Image acquisition involves a computed gamma camera that records the emitted gamma rays and subsequently generates an image that is displayed and processed on an advanced workstation. Normal scintigraphic findings are described as a symmetric distribution of activity throughout the skeletal system in healthy adults.
Urinary bladder activity, faint renal activity, and minimal soft-tissue activity are also normally present.2 Areas of increased bone metabolism are scintigraphically demonstrated as areas of increased tracer uptake and are referred to as "hot spots". Decreased uptake, referred to as "cold spots" are associated with metabolically inactive bone, lack of osteogenesis, or an absent vascular supply.4 Bone-imaging techniques include standard bone scan (whole body scanning), three-phase bone scan, SPECT and SPECT/CT.1,4
The power of the bone scan as a diagnostic modality is most widely appreciated in oncology where it is employed in the detection of primary skeletal tumours and osseous metastases, but other applications include the assessment of bone grafts, acute infection, osteonecrosis of the jaw and condylar hyperplasia. These applications are discussed in more detail below. Malignant bone lesions most frequently present scintigraphically as one or more randomly distributed "hot spots". The presence of multiple, randomly distributed areas of increased uptake of varying shape, size and intensity are highly suggestive of bone metastases. While these "hot spots" are not specific, their location, intensity, and pattern of distribution are analysed to exclude other causes such as traumatic injury and osteoporosis. The success of osseointegrated dental implants is largely dependent on the quality and amount of bone available for osseous integration. Bone is often grafted to support implants or to replace parts of the jaw marred by periodontal disease, trauma, tumour infiltration, cystic lesions, or congenital defects. Three-phase positive bone scans have been shown to correlate with viable bone grafts thus enhancing prognostication and planning.5
In unviolated bone, a three-phase bone scan has high diagnostic accuracy for the detection of acute osteomyelitis and is often positive days or weeks before any changes may be appreciated on plain radiographs. However, in the setting of any underlying bone pathology, the sensitivity of the scan remains high, but the specificity becomes limited.4 In such cases, second-line infection imaging needs to be performed. In current clinical practice, this involves the use of radiolabelled autologous white blood cells (WBCs), the rationale being that the bio-distribution of activated white cells can be imaged due to their active accumulation at sites of infection or inflammation.
WBCs may be radiolabelled in vitro - white blood cells are isolated from a sample of the patients' blood and radiolabelled under aseptic conditions, or targeted in vivo with radiolabelled antibodies that bind to antigens expressed by activated neutrophils. The use of regular bone scans as routine investigations for disease progression makes the bone scan an attractive predictive imaging tool for osteone-crosis of the jaw which may be caused by infection, external beam irradiation (osteoradionecrosis), or medication-related (MRONJ).6
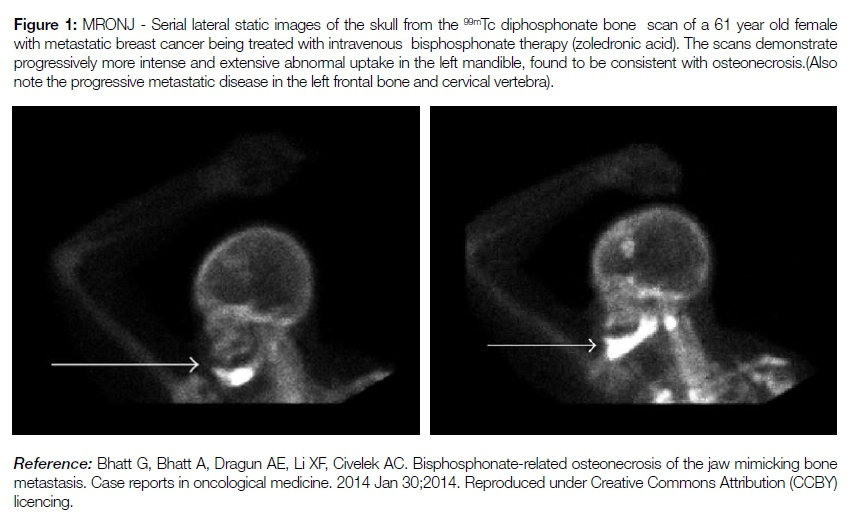
Osteoradionecrosis (ORN) is defined as irradiated bone that fails to heal over a period of 3 months without evidence of residual or recurrent tumour.7 The incidence of ORN is increasing in tandem with the rise in oropharyngeal cancers. The mean time for the development of ORN following irradiation ranges between 22 and 47 months.8 Biphosphonate induced osteonecrosis may remain asymptomatic for many weeks or months. Bisphosphonates are often used in conjunction with chemotherapy for the treatment of hypercalcaemia associated with malignancy, lytic bone metastasis, and multiple myeloma. Biphosphonates are also frequently prescribed for osteoporosis.
Bisphosphonates bind to osteoclasts in areas of active bone resorption to reduce osteoclastic recruitment; longevity and activity. During the early stages of MRONJ, areas of reduced uptake are consistent with the decreased vascularity of diseased bone.
As the disease progresses, bone scintigraphy can show areas of radionuclide uptake reflective of osteoblastic hyperactivity in a subchondral location.9 Scintigraphy is thus proposed as a screening tool by some authors to detect subclinical osteonecrosis in patients receiving bisphosphonates (see figure 1).9,10 Condylar hyperplasia (CH) is a rare bone disorder that is characterised by excessive growth of the condylar process of the mandible. It is typically a unilateral disorder (UCH), with resultant facial asymmetry, deformity, and malocclusion. It usually presents predominantly in female patients during adolescence. UCH is classified as a self-limiting condition and is characterised by a stationary and active phase. UCH is best managed during the stationary phase to prevent further deformity and unnecessary disruption of the TMJ. Functional imaging is uniquely able to differentiate between the two phases based on a qualitative and quantitative assessment of the uptake on the affected side, which will be asymmetrically higher during the active phase with a return to normal during the stationary phase.
Lymphoscintigraphy and Sentinel Node Mapping
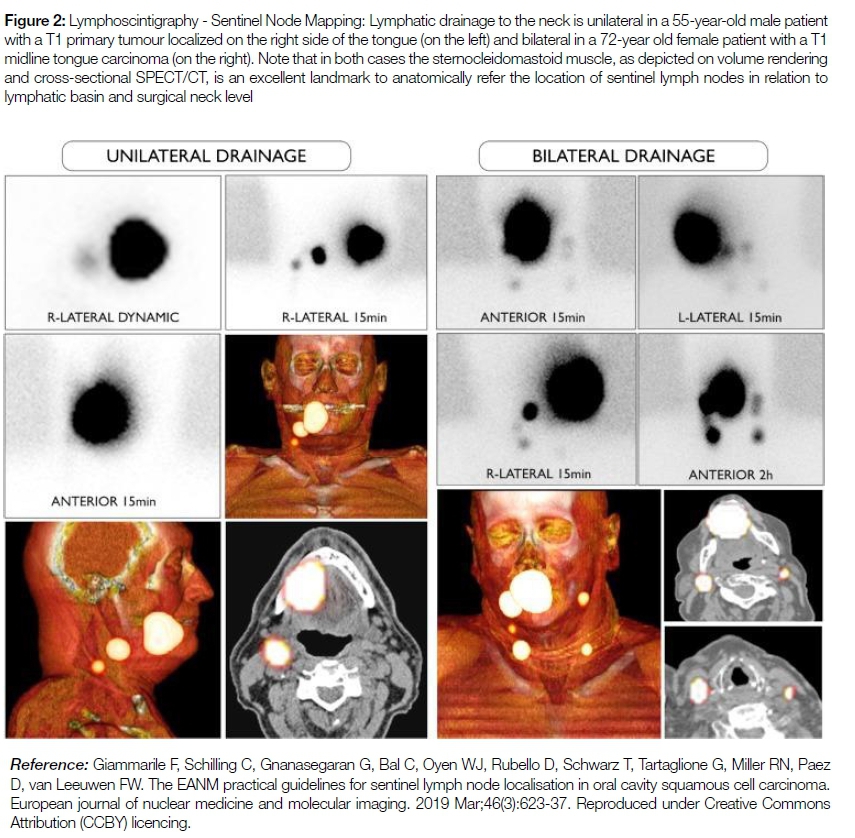
Nodal involvement is one of the most important prognostic factors in head and neck cancer. Sentinel lymph node(s) (SLN) refer to the first lymph node(s), in a lymph node group, to receive lymphatic drainage and metastasis from a tumour.
Functional imaging in the form of lymphoscintigraphy utilising radiolabelled nano-particles can identify the SLN, both preoperatively through imaging, and intraoperatively by using a hand-held gamma probe. The aim of lympho-scintigraphy is to 'map' or identify the SLN for intraoperative frozen section and pathological evaluation. If the SLN biopsy is negative, the remaining nodes may not require routine resection which reduces operative and anaesthetic time, intra- and postoperative morbidity, and recovery times. 99mTc nanocolloid is injected around the tumour and will be carried by lymph to a regional lymph node group and subsequently retained in the SLN. Regional imaging following injection allows for the preoperative delineation of lymphatic pathways and the SLN. SPECT/CT is particularly useful in SLN mapping with the SPECT component providing the high sensitivity for SLN detection and the CT allowing for anatomical localisation of the lymph node (see figure 2).
PET
PET is principled on the use of positron-emitting radioisotopes. Following intravenous administration and subsequent in-vivo localisation of a radiopharmaceutical, the PET radioisotope undergoes radioactive decay and emits a positron. The positron travels a short distance from the point of decay and interacts with an electron in the orbit of an atom in its path.
The positron and electron undergo an 'annihilation reaction' and produce two gamma photons that travel in opposite directions, which are detected by a PET camera. PET imaging has several inherent advantageous over SPECT. Higher image resolution, sensitivity, and quantification is achieved with PET because of higher energy gamma photons, electronic (rather than physical collimation) and the use of hybrid PET/CT and PET/MR scanners which allow for attenuation correction. Hybrid scanners also improve specificity through accurate localisation of tracer accumulation, tissue characterisation, distinguishing physiologic from pathologic uptake, and verifying a suspicious finding on one modality by confirmation on the other. Commonly utilised PET radioisotopes include 11C, 13N, 15O, 18F, 64Cu, 124I, and 89Zr. These radioisotopes may be used to label more organic compounds (such as glucose, amino acids, neurotransmitters, DNA nucleosides, antibodies etc.), which permit non-invasive, whole body molecular imaging of tumour biology. Molecular imaging has ensconced itself as an essential tool in both the preclinical and clinical setting in oncology, cardiology, neurology, neuroscience and pharma-cology.However, the cost and availability of PET/CT remain a challenge, particularly in resource-constrained environments.
Most clinical applications of PET employ the use of flourineflourine18-labeled flouro-2-deoxyglucose (18F-FDG), a radiolabelled glucose analogue.11 The uptake of 18F-FDG is based on the 'the Warburg effect' - neoplastic cells do not obey normal homeostatic control mechanisms that regulate growth and metabolism, thus they consume large amounts of glucose to fuel their growth and hypermetabolism.12 18F-FDG PET/CT is now a key diagnostic tool in oncology, including in (H&N) head and neck cancer (see figure 3).
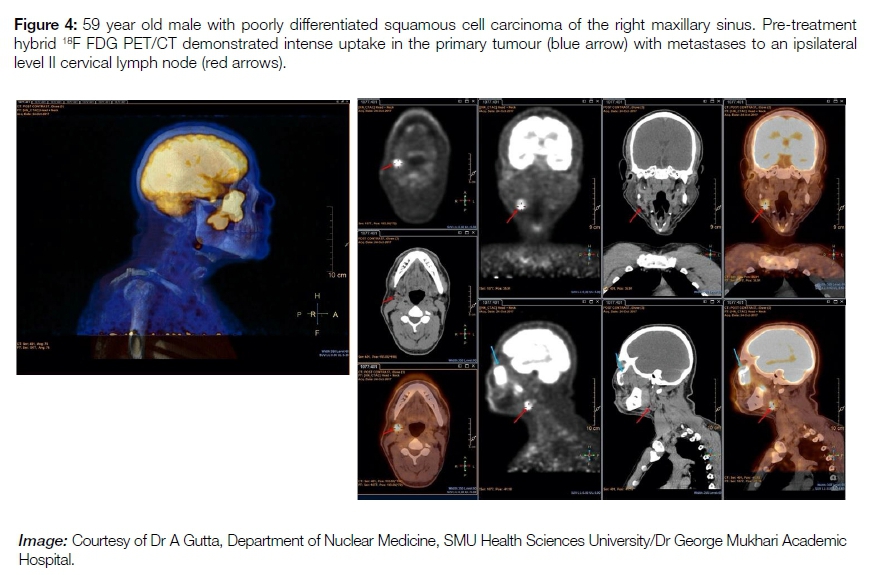
Initial staging: (see figure 4) As with any cancer, accurate initial staging plays a vital role in management and prognostication. While cross-sectional CT and MRI remain the primary imaging modalities for tumour (T) staging, 18F-FDG PET/CT plays an important role in nodal (N) and metastatic disease (M) evaluation, particularly in more advanced disease or tumours with a high metastatic risk (such as naso- or hypopharyn-geal tumours).13 Furthermore, PET/CT may be beneficial in the setting of metallic artefacts caused by dental restorative materials which may severely degrade the interpretability and diagnostic localisation of CT.14 The strength of PET/CT in N and M staging lies in its ability to detect disease in normal-sized organs (including lymph nodes), and routine whole body scanning with the capability of detecting clinically and/ or radiologically occult distant disease. Accurate N staging is especially important in oral cancer, as the presence of metastatic spread to regional lymph nodes correlates strongly with a poor overall prognosis, an increased risk of distant metastasis and a reduction in 5-year survival rates by approximately 50%.14,15
Detection of synchronous cancers:18F-FDG PET/CT is more accurate than than conventional imaging in the detection of second primary malignancies and should be considered in selected cases where conventional imaging is negative or equivocal.16,17
Detection of recurrence: It may be difficult to differentiate between post-treatment anatomical changes (such as fibrosis or necrosis) and residual and/or recurrent tumour on conventional imaging. 18F-FDG PET/CT imaging relies on a metabolic signal from viable tumour cells. It is therefore reported to be more accurate than anatomical imaging in this setting, especially if conventional modalities are equivocal.18,19
Radiotherapy planning: Imaging plays an increasingly important role in radiotherapy planning. There is a growing body of evidence that advocates for the use of 18F-FDG PET/ CT to more precisely define tumour volumes, especially in intensity-modulated radiotherapy, where accurate delineation of disease is critical.20-23 Metabolic data from the PET/CT facilitates the determination of a biological target volume. Modulated therapy can be applied in accordance with metabolic activity within the target volume.24
Therapy response evaluation: Accurate assessment of treatment response is essential in the management of patients with H&N cancer. Treatment-associated oedema, hyperaemia, scarring, and the loss of facial planes may make it difficult to differentiate between residual and/or recurrent disease and post-therapy changes on conventional CT or MRI.25 Conventional imaging relies on size as the most important criterion for response assessment. Limitations in using size include inaccurate response assessment in the setting of residual tumour necrosis and/or fibrosis. Conversely, metabolic response to therapy may be assessed using 18F-FDG PET/CT, where cellular viability is determined from a metabolic signal that is independent of size.
Prognostic value: A meta-analysis assessing the effectiveness of intra- and post-therapy FDG PET/CT in predicting long-term survival outcomes in patients treated for H&N squamous cell carcinoma found that interim and post-therapy PET/CT could accurately predict the risk of death or disease progression after two years and three to Ave years, respectively.26
Detection of recurrence / follow-up: (see figure 5) In patients with H&N squamous cell carcinoma, early and accurate post-therapy diagnosis of recurrence offers the best opportunities for salvage treatment and prognostic prediction. Due to its ability to detect local, regional nodal and distant recurrence, FDG PET/CT is a useful modality for follow-up in these patients.16'27,28 High cost and limited availability restrict the routine use of PET/CT in this setting, but the study should be considered in patients with a high clinical suspicion in whom conventional imaging is negative or equivocal.
Carcinoma of Unknown Primary (CUP): Despite extensive clinical examination, pan-endoscopy, CT and MRI, the primary tumour may not be detected in 5-10% of patients who present with cervical nodal squamous cell cancer metastases. PET/CT offers an additional 25% detection rate when compared to conventional workup.29 Lesion detection may be complicated in small volume disease in the primary tumour, normal biodistribution of FDG in the H&N and some tumours have inherently low FDG uptake.30
PET/MRI
Hybrid PET/MRI is now approved and commercially available, although current installations are limited due to the high cost and complicated installation. Early studies suggest that PET/MRI performs as well as PET/CT in the staging and restaging of H&N cancer and in radiation therapy planning. The MRI component has the advantages of high spatial resolution and soft tissue characterisation, which may assist in therapy planning, coupled with no ionising radiation, which reduces the radiation burden to the patient.31,32
CONCLUSION
Bone scintigraphy, lymphoscintigraphy, SPECT and PET are but a few of the physiological imaging modalities that serve the fundamental purposes of detection, characterisation, and potential staging of disease. Each modality plays a specific role in the diagnostic arena and is best appreciated as a diagnostic tool that is selected to best complement other clinical and laboratory findings. South African public health sector patients often present at initial consultation with advanced disease that is often complicated by infective conditions. Within this resource and financially constrained sector it becomes imperative that oral health care practitioners appreciate the value of appropriate advanced imaging to facilitate cost-effective and efficient treatment. Accurate interpretation of advanced imaging studies requires additional expertise to recognise both normal and abnormal processes in a somewhat larger field of view than in traditional dental imaging systems.33 In light of advancing diagnostic and treatment methodologies and the interdisciplinary management of patients, it is essential that the dental professional appreciates the applicability of nuclear medicine within his scope of practice.
References
1. Brenner AI, Koshy J, Morey J, Lin C, Dipoce J. The bone scan. Semin Nucl Med.2012. 299 42(1):11- 26. [ Links ]
2. Love C, Din AS, Tomas MB, Kalapparambath TP, Palestro CJ. Radionuclide Bone Imaging: An Illustrative Review. Radiographics. 2003;23(2):341-58. [ Links ]
3. Cook GJR. Imaging with radiolabelled bisphosphonates. Bone [Internet]. 2020; 137:115372. [ Links ]
4. Ferreira RI, de Almeida SM, Bóscolo FN, Santos AO, Camargo EE. Bone Scintigraphy 305 as an Adjunct for the Diagnosis of Oral Diseases. J Dent Educ. 2002;66(12):1381-7. [ Links ]
5. Schuepbach J, Dassonville O, Poissonnet G, Demard F. Early postoperative bone scintigraphy in the evaluation of microvas-cular bone grafts in head and neck reconstruction. Head Face Med. 2007;3(1):1-6. [ Links ]
6. O'Ryan FS, Khoury S, Liao W, Han MM, Hui RL, Baer D, et al. Intravenous Bisphosphonate-Related Osteonecrosis of the Jaw: Bone Scintigraphy as an Early Indicator. J Oral Maxillofac Surg. 2009;67(7):1363-72. [ Links ]
7. Chronopoulos A, Zarra T, Ehrenfeld M, Otto S. Osteoradionecrosis of the jaws: definition, epidemiology, staging and clinical and radiological findings. A concise review. Int Dent J. 2018;68(1):22-30. [ Links ]
8. Hricak H, Choi BI, Scott AM, Sugimura K, Muellner A, Von Schulthess GK, et al. Global trends in hybrid imaging. Radiology. 2010;257(2):498-506. [ Links ]
9. O'Ryan FS, Khoury S, Liao W, Han MM, Hui RL, Baer D, et al. Intravenous bisphosphonate-related osteonecrosis of the jaw: bone scintigraphy as an early indicator. J Oral Maxillofac Surg 2009; 67(7):1363-72. [ Links ]
10. Chiandussi S, Biasotto M, Dore F, Cavalli F, Cova MA, Di Lenarda R. Clinical and diagnostic imaging of bisphosphonate-associated osteonecrosis of the jaws. Dentomaxillofac Radiol 2006; 35(4):236-43. [ Links ]
11. Omami G, Tamimi D, Branstetter BF. Basic principles and applications of (18)F-FDG- PET/CT in oral and maxillofacial imaging: A pictorial essay. Imaging Sci Dent 2014; 44(4):325-32. [ Links ]
12. Vander Heiden MG, Cantley LC, Thompson CB. Understanding the Warburg effect: the metabolic requirements of cell proliferation. Science 2009; 324(5930):1029-33. [ Links ]
13. Vorster M, Doruyter A, Brink A, Mkhize S, Holness J, Malan N et al. Appropriate indications for positron emission tomography/ computed tomography. SAMJ 2015; 106(1): 105-122. [ Links ]
14. Warburton G, Nikitakis NG, Roberson P, Marinos NJ, Wu T, Sauk JJ, et al. Histopathological and lymphangiogenic parameters in relation to lymph node metastasis in early-stage oral squamous cell carcinoma. J Oral Maxillofac Surg 2007; 65(3):475-84. [ Links ]
15. Greenberg JS, El Naggar AK, Mo V, Roberts D, Myers JN. Disparity in pathologic and clinical lymph node staging in oral tongue carcinoma. Implication for therapeutic decision making. Cancer 2003; 98(3):508-15. [ Links ]
16. Kim Y, Roh JL, Kim JS, Lee JH, Choi SH, Nam SY et al. Chest radiography or chest CT plus head and neck CT versus 18F-FDG PET/CT for detection of distant metastasis and synchronous cancer in patients with head and neck cancer. Oral Oncol. 2019: 1; 88:109-14. [ Links ]
17. Rohde M, Nielsen AL, Johansen J, Sorensen JA, Nguyen N, Diaz A et al. Head-to-head comparison of chest x-ray/head and neck MRI, chest CT/head and neck MRI, and 18F- FDG PET/CT for detection of distant metastases and synchronous cancer in oral, pharyngeal, and laryngeal cancer. Journal of Nuclear Medicine. 2017: 1;58(12):1919-24. [ Links ]
18. Kim SA, Roh JL, Kim JS, Lee JH, Lee SH, Choi SH et al. 18F-FDG PET/CT surveillance for the detection of recurrence in patients with head and neck cancer. Eur J Cancer. 2017 :1; 72:62-70. [ Links ]
19. Driessen JP, Peltenburg B, Philippens ME, Huijbregts JE, Pameijer FA, de Bree R et al. Prospective comparative study of MRI including diffusion-weighted images versus FDG PET-CT for the detection of recurrent head and neck squamous cell carcinomas after (chemo) radiotherapy. Eur J Radiol. 2019:1; 111:62-7. [ Links ]
20. Daisne JF, Duprez T, Weynand B, Lonneux M, Hamoir M, Reychler H et al. Tumor volume in pharyngolaryngeal squamous cell carcinoma: comparison at CT, MR imaging, and FDG PET and validation with surgical specimen. Radiology. 2004 Oct;233(1):93-100. [ Links ]
21. Geets X, Tomsej M, Lee JA, Duprez T, Coche E, Cosnard Get al. Adaptive biological image-guided IMRT with anatomic and functional imaging in pharyngo-laryngeal tumors: impact on target volume delineation and dose distribution using helical tomotherapy. Radiotherapy and Oncology. 2007 Oct 1;85(1):105-15. [ Links ]
22. Moule RN, Kayani I, Moinuddin SA, Meer K, Lemon C, Goodchild K et al. The potential advantages of 18FDG PET/CT-based target volume delineation in radiotherapy planning of head and neck cancer. Radiotherapy and Oncology. 2010 Nov 1;97(2):189- 93. [ Links ]
23. Berthon B, Evans M, Marshall C, Palaniappan N, Cole N, Jayaprakasam V et al. Head and neck target delineation using a novel PET automatic segmentation algorithm. Radiotherapy and Oncology. 2017;1;122(2):242-7. [ Links ]
24. Alongi P, Laudicella R, Desideri I, Chiaravalloti A, Borghetti P, Quartuccio N et al. Positron emission tomography with computed tomography imaging (PET/CT) for the radiotherapy planning definition of the biological target volume: PART 1. Crit Rev Oncol Hematol. 2019;1; 140:74-9. [ Links ]
25. Subramaniam RM, Truong M, Peller P, Sakai O, Mercier G. Fluorodeoxyglucose- positron-emission tomography imaging of head and neck squamous cell cancer. AJNR Am J Neuroradiol. 2010;1;31(4):598-604. [ Links ]
26. Sheikhbahaei S, Ahn SJ, Moriarty E, Kang H, Fakhry C, Subramaniam RM. Intratherapy or posttherapy FDG PET or FDG PET/CT for patients with head and neck cancer: a systematic review and meta-analysis of prognostic studies. AJR Am J Roentgenol. 2015;205(5):1102-13. [ Links ]
27. Sheikhbahaei S, Taghipour M, Ahmad R, Fakhry C, Kiess AP, Chung CH, Subramaniam RM. Diagnostic accuracy of follow-up FDG PET or PET/CT in patients with head and neck cancer after definitive treatment: a systematic review and meta-analysis. AJR Am J Roentgenol. 2015;205(3):629-39. [ Links ]
28. Kim JW, Roh JL, Kim JS, Lee JH, Cho KJ, Choi SH et al. 18F-FDG PET/CT surveillance at 3-6 and 12 months for detection of recurrence and second primary cancer in patients with head and neck squamous cell carcinoma. Br J Cancer. 2013;109(12):2973-9. [ Links ]
29. Rusthoven KE, Koshy M, Paulino AC. The role of fluorodeoxy-glucose positron emission tomography in cervical lymph node metastases from an unknown primary tumor. Cancer.2004; 1;101(11):2641-9. [ Links ]
30. Goel R, Moore W, Sumer B, Khan S, Sher D, Subramaniam RM. Clinical practice in PET/CT for the management of head and neck squamous cell cancer. AJR Am J Roentgenol. 2017;209(2):289-303. [ Links ]
31. Szyszko TA, Cook GJ. PET/CT and PET/MRI in head and neck malignancy. Clinical radiology. 2018. Jan 1;73(1):60-9. [ Links ]
32. Olin AB, Hansen AE, Rasmussen JH, Ladefoged CN, Berthelesen AK, Hakansson K et al. Feasibility of multipara-metric positron emission tomography/magnetic resonance imaging as a one-stop shop for radiation therapy planning for patients with head and neck cancer. International Journal of Radiation Oncology*Biology*Physics.2020 Dec1;108(5):1329-38. [ Links ]
33. Benson BW, Flint DJ, Liang H, Opatowsky MJ. Advances in diagnostic imaging for pathologic conditions of the jaws. Head Neck Pathol 2014; 8(4):383-91. [ Links ]
 Correspondence:
Correspondence:
Dr Sandeepa Rajbaran Singh
Telephone: (012) 521 4902
Email: sandeepa.singh@smu.ac.za
The role played and the respective contribution:
1 . Dr Sandeepa Rajbaran Singh: First author - contributed to the write-up and editing of the text and images: 50%
2 . Dr Aadil Abdulaziz Gutta: Second author - contributed to the write-up and editing of the text and images: 50%


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}