










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.75 no.9 Johannesburg Out. 2020
http://dx.doi.org/10.17159/2519-0105/2020/v75no9a2
CASE REPORT
Schwannoma of the infratemporal fossa - A rare case report
S BansalI; D BasavanthappaII; P PrasadIII; MS RautIV; RS DesaiV
IMDS., Associate Professor, Department of Oral Pathology and Microbiology, Nair Hospital Dental College, Mumbai, India. ORCID Number: 0000-0003-1163-5418
IIMDS., Consultant, Oral and Max-illofacial Surgeon, Seven Hills Hospital, Mumbai, India
IIIMDS., Assistant Professor, Department of Oral Pathology and Microbiology, Nair Hospital Dental College, Mumbai, India
IVMDS., Assistant Professor, Dept of Oral and Maxillofacial Pathology, Nair Hospital Dental College, Mumbai, India
VMDS., Professor and Head, Department of Oral Pathology and Microbiology, Nair Hospital Dental College, Mumbai, India
ABSTRACT
Schwannoma is a benign nerve sheath tumour that originates from schwann cells of the peripheral nerve. In spite of constituting 25-40% of head and neck tumours its in-traoral presentation is rare which accounts for only 1%.
The purpose of this case report is to highlight the rarity of this lesion, to emphasize the significance of an accurate diagnosis and to include tumours of nerve sheath origin in the differential diagnosis of facial asymmetry.
Keywords: Schwannoma, nerve sheath, head and neck region.
INTRODUCTION
Schwann cells intimately ensheath all neurons of both myelinated and non-myelinated nerves in the peripheral nervous system.1 Schwannomas occurring in the head and neck region constitute 25-45% of head and neck tumours.2
The present case of schwannoma is limited to the in-fratemporal fossa, which is a rare location, arising from the extradural division of the trigeminal nerve. Trigeminal schwannomas account for about 0.2% of all intracranial, tumours and 0.8% and 8% of intracranial schwan-nomas.3 Surgically a zygomatico-temporal approach was planned to provide access to such a cryptic anatomical region whilst ensuring a satisfactory cosmetic result.
CASE REPORT
An 18-year-old female reported with a main complaint of a gradually increasing painless swelling on right side of the face of 4 months duration. It extended from right ala of nose to preauricular notch, anteroposteriorly, and from right maxillary buccal vestibule to right infraorbital region, superioinferiorly (Fig. 1).

Intraorally, the right maxillary buccal vestibule was obliterated. The swelling was Arm on palpation and the patient presented with difficulty in opening of mouth. There were no neurological signs on the right side of the face.
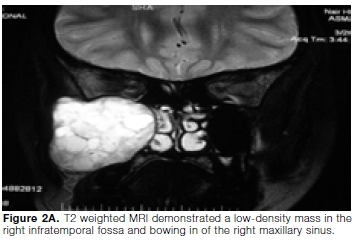
T2 weighted MRI demonstrated a large well defined, hete-rogeneously enhanced mass measuring 5x4.4x4.2 cm in right infratemporal fossa. The posterior wall of the right maxillary antrum was bowed anteriorly and the floor of the orbit was attenuated by the mass (Fig. 2A). The lesion showed extension into the right cavernous sinus. Widening of foramen rotundum was noted.
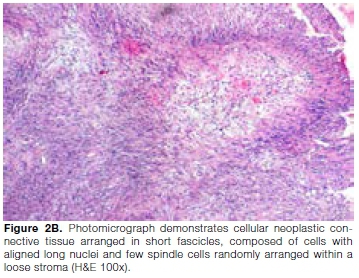
Based on the clinical and radiological findings, a provisional diagnosis of a benign soft tissue neoplasm in the right infratemporal fossa was made. An intraoral incision biopsy was performed under local anaesthesia from right maxillary molar region. Histopathologically, connective tissue was shown to be composed of numerous spindle cells arranged in fascicles and in a palisading pattern depicting hypercellular Antoni A arrangement.
The spindle cells were characterized by flattened elongated and tapered nuclei. Presence of chronic inflammatory infiltrate was seen; neural bundles were also evident in a few areas of the stroma consistent with a diagnosis of spindle cell neoplasm (Fig. 2B). Immuno-histochemical analysis showed S100 positivity (Fig. 2C). Based on the clinicopathological and immunohistolog-ical features, a final diagnosis of the spindle cell lesion Schwannoma was established.

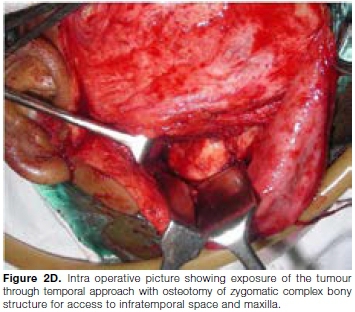
The tumour resection was planned through zygomatico-temporal approach with osteotomy of zygomatic complex bony structure for access to infra temporal space and maxilla (Fig. 2D) for ensuring a satisfactory cosmetic result. The whole zygomatic complex bony structure was retracted laterally to expose the tumour in the infra temporal fossa. The tumour was enucleated as a single mass. After excision the tumour, a rigid fixation of osteotomised bony complex back in premarked position was done with miniplates. Healing was uneventful. A 5-year follow-up showed no sign of recurrence.
DISCUSSION
Schwannoma (neurilemmoma) is a rare, benign, encapsulated perineural tumour of neuroectodermal origin that is derived from the Schwann cells of the neural sheath. Earlier, Verocay4 referred to it as a "neuronoma." Later, Stout used the term, "neurilemmoma," believing that this tumour originated from the Schwann cells.4
Twenty-five to forty-eight percent of all cases of schwannomas occur in the head and neck region.5-7 It is more common between 30 and 50 years of life.8 William et al.9 showed that in 83% of the cases studied by them, schwannomas presented in males, while for Lucas, there was a greater predilection for females which is in accordance to our case and for Hatziotis9 and Asprides, Enzinger and Weiss,9 there was an equal distribution.4,9 Within the head and neck region, the tongue, palate, cervical and pharyngeal regions are frequently involved, but a lesion in the infratemporal fossa is relatively rare.8,10,11
Clinically Schwannoma presents with symptoms related to the nerve involved maybe associated with pain along with other symptoms such as hearing loss, hoarseness and dysphagia, depending on the site of involvement. However, lack of symptoms is common when the lesion originates from the trigeminal nerve and is located in the infratemporal fossa which is in accordance to our case report.11
Trigeminal schwannomas account for about 0.2% of all intra cranial tumors, and 0.8% and 8% of intracranial schwannomas.3 In the present case, the tumour showed evidence of originating from the second division of the fifth cranial nerve near the foramen rotundum. They can originate from any section of the fifth cranial nerve, from the root to the distal extracranial branches, but the majority develops at the Gasserian ganglion, usually growing in the middle cranium.3 In our case, though intra-cranial extension into the right cavernous sinus was seen, during surgery the duramater was found to be intact. It was concluded that the tumour primarily originated within infratemporal fossa.
The infratemporal region is the irregular retromaxillary space, inaccessible by virtue of its relatively concealed location, and is remote for clinical examination.12 Tumours in this clinically silent area always pose a problem in diagnosis and management. They cannot be seen clinically while they are still confined within the boundaries of the fossa, and localizing signs and symptoms usually do not become apparent until the tumour reaches a significant size.11 In the present case, the patient was asymptomatic, radiographs showed erosion of the bony walls of infratemporal fossa, thinning of floor of orbit and extension into the sphenoid sinus.
CONCLUSION
Though rare, the treatment of infratemporal schwannomas provide a great surgical challenge. The low incidence of schwannomas often leads to the omission of the tumour in the differential diagnosis of soft tissue tumours of the oral cavity. We have presented a unique case of a schwannoma of the infratemporal fossa to stress its rarity and importance of ruling out neurogenic tumours in differential diagnosis of facial asymmetry without paraesthesia.
Declaration
The authors of this manuscript declare no conflict of interests.
Ethics statement
Ethics approval is obtained. All details of the patient have been anonymized.
References
1. Huang YF, Kuo WR, Tsai KB. Ancient schwannoma of the infratemporal fossa. J Otolaryngol. 2002; 31: 236-8. [ Links ]
2. Ansari I, Ansari A, Graison AA, Patil AJ, Joshi H. Head and Neck Schwannomas: A Surgical Challenge - A Series of 5 Cases. Case Rep Otolaryngol. 2018. [ Links ]
3. Politi M, Toro C, Sbuelz M. A giant trigeminal schwanno-ma of the infratemporal fossa removed by transmandibular approach and coronoidectomy. Oral Maxillofac Surg. 2016; 2: 10-3. [ Links ]
4. Piyush P, Mohanty S, Ghosh S, Gupta S. A rare report of two cases: Ancient schwannoma of infratemporal fossa and verocay schwannoma of buccal mucosa. Ann Maxillofac Surg. 2017; 7: 140. [ Links ]
5. Ross C, Wright E, Moseley J, Rees R. Massive schwannoma of the nose and paranasal sinuses. South Med J. 1988; 81: 1588-91. [ Links ]
6. Hillstrom RP, Zarbo RJ, Jacobs JR. Nerve sheath tumors of the paranasal sinuses: electron microscopy and histo-pathologic diagnosis. Otolaryngol Head Neck Surg 1990; 102: 257-63. [ Links ]
7. Das Gupta TK, Brasfield RD, Strong EW, Hajdu SI. Benign solitary schwannoma (neurilemmomas) Cancer 1969; 24: 355-66. [ Links ]
8. Shinohara T, Miyashita K, Yoshimi M. On cases with neuri-lemmoma in Otolaryngol. 1970; 13: 11-7. [ Links ]
9. Martins MD, et al. Intra-oral schwannoma: Case report and literature review. Indian J Dent Res. 2009; 20: 121. [ Links ]
10. Gibbons SD, Wiesenfeld D, Millar H, Busmanis IA. Removal of a retromaxillary schwannoma via a temporal approach. J Oral Maxillofac Surg. 1991; 49: 191-3. [ Links ]
11. Al-Ghamdi S, Black MJ, Lafond G. Extracranial head and neck schwannomas. J Otolaryngol. 1992; 21: 186-8. [ Links ]
12. Tiwari R, Quak J, Egeler S, Smeele L, vd Waal I, vd Valk P, Leemans R. Tumors of the infratemporal fossa. Skull Base Surg. 2000; 10: 1-10. [ Links ]
 Correspondence:
Correspondence:
Shivani Bansal
Associate Professor, Department of Oral Pathology and Microbiology, Nair Hospital Dental College
Dr. AL Nair Road, Mumbai, 400 008, India
Email: bshivani2000@gmail.com
Author contributions:
1. Shivani Bansal: Examined the patient; conceiving the idea for the case report, contributed to writing the case report, edited the case report and approved the final draft - 20%
2. Dilipkumar Basavanthappa: Treated the case, approved the final draft of the case report - 20%
3. Pooja Prasad: Lead the writing of the case report, approved the final draft - 20%
4. Mugdha S Raut: Lead the writing of the case report, approved the final draft - 20%
5. Rajiv S Desai: Examined the patient; conceiving the idea for the case report, approved the final draft - 20%

