










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.75 n.6 Johannesburg Jul. 2020
http://dx.doi.org/10.17159/2519-0105/2020/v75no6a6
CASE REPORT
Visual assessment is no substitute for radiographic analysis - A forensic case report
L RobinsonI; C NelII; H BernitzIII
IBChD, PDD (Maxillofacial Radiology), PDD (Forensic Odontology), Department of Oral Pathology and Oral Biology, School of Dentistry, Faculty of Health Sciences, University of Pretoria, Pretoria, South Africa. ORCID Number: 0000-0002-0549-7824
IIBChD, MSc (Maxillo-facial and Oral Radiology), Department of Oral Pathology and Oral Biology, School of Dentistry, Faculty of Health Sciences, University of Pretoria, Pretoria, South Africa. ORCID Number: 0000-0003-4047-6356
IIIBChD, Dip (Odont), MSc, PhD, Department of Oral Pathology and Oral Biology, School of Dentistry, Faculty of Health Sciences, University of Pretoria, Pretoria, South Africa. ORCID Number: 0000-0003-1361-1225
CASE REPORT
The details of this case have been omitted in order to maintain anonymity.
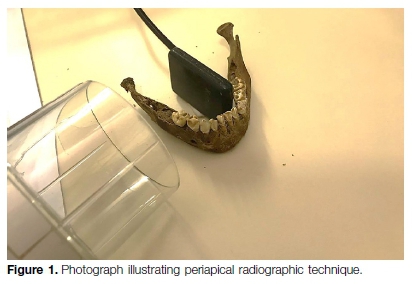
While preparing the foundations for a new house, a builder happened to find a small mandible buried just below the surface. Human skeletal remains in the form of a mandible were submitted to the forensic odontology unit at the University of Pretoria for age assessment.
On initial macroscopic examination, all mandibular deciduous teeth were present and fully erupted. Both mandibular permanent first molars were visible, due to the exposed overlying alveolar bone, but were still fully submerged with no evidence of eruption. At this stage, a dental age estimation of approximately 4-5 years was proposed based on the presence of all mandibular deciduous teeth and the exposure of the mandibular permanent first molars.
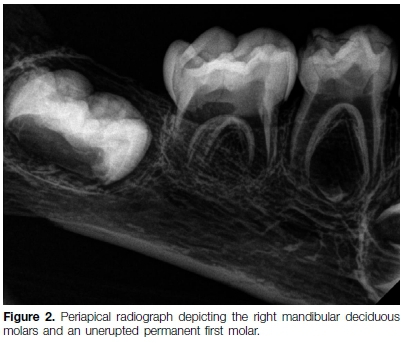
A radiographic analysis followed (Figure 1), whereby it was noted that the mandible was less mature than initially suspected from the visual examination (Figures 2-4). The developmental stages of the relevant teeth were analysed according to the methods of AlQahtani et al., London Atlas of Human Tooth Development and Eruption, 20101, and the Developmental Atlas of the Human Dentition (Oral Anatomy, Histology and Embryology), 4th Edition, 2009.2


Al Qahtani et al, London Atlas of Human Tooth Development and Eruption (2010)1 (Figure 5)-
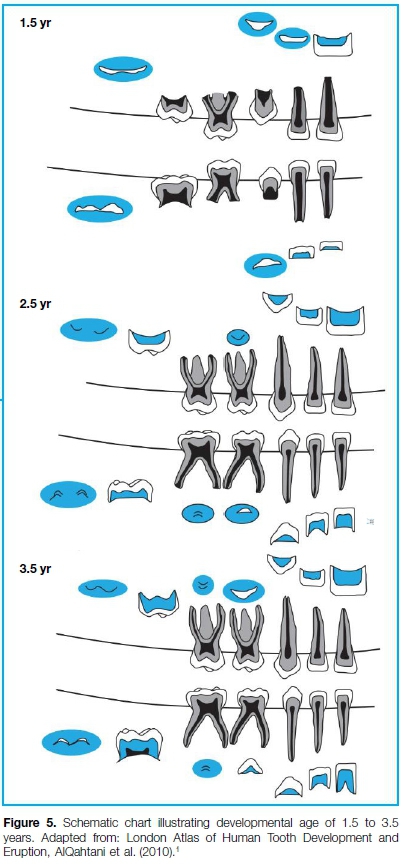
The development of the teeth 36, 75, 74, 33, 32 and 31 correspond closest to the development seen at age >1.5 years and <2.5 years. It must be stated that the development stages are only given in yearly intervals. It is important to note that the radiographs taken of the mandibular teeth showed no initial crypt development of teeth 34 and 35. This strongly indicates an age of less than 2.5 years. An age of >1.5 but <2.5 years can therefore be considered reliable.
Developmental Atlas of the Human Dentition, Oral Anatomy, Histology and Embryology, 4th Edition (2009)2
The development of the teeth 36, 75, 74, 33, 32 and 31 correspond closest to the development seen at age >2 years and < 3 years. An age of 2.5 years with a 6-month dispersion can therefore be considered reliable using this method. This method was used as a quality control understanding its limitations.
It was therefore concluded, that according to both methods, an age of < 2.5 years with a 6-month dispersion could be considered reliable for the mandibular remains.
DISCUSSION
Dental age estimation of living and deceased individuals has been the subject of extensive research worldwide. In recent years, population specific standards have been sought to assist in meeting rigorous legal requirements.3
Calculation of the biological age of an individual has many applications in the field of dentistry. It can be used to determine appropriate timing of orthodontic treatment, to analyse the developmental stage of an individual relative to the general population in cases of disturbed growth; and to estimate the age of a living or deceased individual for forensic purposes.1,4-5
Teeth are often used for identification purposes as well as age estimation as they survive inhumation well and show less variability than bones used in skeletal age estimation. Hence, the developing dentition is considered superior to other developmental indicators for age estimation up to maturity.1 Accurate estimation of age at the time of death may be a crucial component in the identification of human remains, and can significantly narrow the field of possibilities in establishing a positive identification.6
Over the years, many authors have recognised the use of systems of age estimation based on dental development. As early as 1935, Schour and Hoffman found that the pattern of calcification of dentition under normal conditions followed a reliable sequence of growth, allowing for age estimation.3,6 This led to the widespread use of dental development-based age-estimation systems. While accurate, many of the techniques require additional training and experience to ensure precision.3-4 Some methods are destructive to tooth tissue and are therefore considered inappropriate in many instances.
Schour and Massler later published an important study that summarised the development of the human dentition in an atlas-style chart consisting of 21 diagrams with an age range from 5 months in utero to 35 years.1 This method involved comparison of a radiograph of the maxillary and mandibular dentitions against diagrams depicting the stage of development. This system was simple to follow, required no major specialised training, and made use of readily available diagnostic aids, i.e periapical radiographs.4 The drawbacks of using an atlas-based system are that they are based on the premise of 'one size fits all'.
Clinicians are required to make a qualitative assessment of the case at hand and match it to the closest suitable diagram, thus a high risk of error exists. Moorrees et al. published research providing norms of formation of ten permanent teeth, namely, the maxillary incisors and all eight mandibular teeth. The findings provided ages of attainment for fourteen selected stages of tooth development, taking into account crown, root and apex development.7
Demirjian et al., in 1973, developed a method using panoramic radiographs for estimating dental maturity based on the stage of development of each tooth present in the jaws. The data was based on measurements obtained from a sample of boys and girls of French Canadian parentage.5 Their method referenced eight tooth developmental stages (A-H) in a chart format, and was considered significantly less complicated than the approach previously published by Moorrees et al.5,8 Unfortunately, this method, although simple in ts application, has been shown by subsequent studies to be inaccurate on population samples of different ethnic heritage.6,9 However, the well-defined stages and objective evaluation still makes Demirjian's method one of the most suitable for forensic purposes.9
Ubelaker's dental chart was produced in 1978 and attempted to modify and improve upon the original chart produced by Schour and Massler.110 Again, this method is not without its limitations, as owing to issues with identification of sex, no differentiation was made between males and females.4 Ubelaker's charts have since been modified for modern Australians, with separate charts created for males and females by adjusting the age of each drawing.4
More recently, work published by AlQahtani et al., based on cases taken from a range of sources, assessed for stages of development using the system devised by Moorrees et al.1 The main advantage of this work over previous methods is the availability of diagrams for each year of development from ages 1 to 23. Each developmental stage is illustrated radiographically and clarifled by the addition of written descriptions.1
As with any categorical system of assessment, the larger number of diagrams results in more accurate estimations of age. This work culminated in the establishment of the so-called 'London Atlas of Human Tooth Development and Eruption', which has subsequently been validated using predominately modern samples with accurate results.3
A recent study compared results from older charts with the more modern London Atlas. Age was estimated more accurately with greater precision, and the percentage correctly aged was higher for the London Atlas compared with Schour and Massler and Ubelaker.10 In spite of these findings, one major limitation with the London Atlas is that age is expressed as a midpoint of an age category and not a point estimate with no measure of dispersion provided in the atlas.
CONCLUSION
Age estimation charts are useful tools to estimate age at time of death. The datasets on which these charts were developed are based upon significant sample sizes and are in many instances sex specific.
In spite of the inherent limitations of the atlas style, these charts are recommended for use as an initial screening tool, especially in a mortuary setting or mass disaster situation. More precise and detailed age estimation analysis should be undertaken when time and other pressures of the forensic environment have subsided.4 This case report highlights an example where the initial visual impression of skeletal remains could have clouded the judgment of the investigators, leading to a miscarriage of justice.
References
1. AlQahtani SJ, Hector MP, Liversidge HM. Brief communication: The London Atlas of Human Tooth Development and Eruption. Am J Phys Anthropol. 2010; 142(3): 481-90. [ Links ]
2. Berkovitz BKB, Holland GR, Moxham BJ. Oral Anatomy, Histology and Embryology. 4th ed. Edinburgh: Mosby/ Elsevier; 2009. [ Links ]
3. Baylis S, Bassed R. Precision and accuracy of commonly used dental age estimation charts for the New Zealand population. Forensic Sci Int. 2017; 277: 223-8. [ Links ]
4. Blenkin M, Taylor J. Age estimation charts for a modern Australian population. Forensic Sci Int. 2012; 221(1-3): 106-12. [ Links ]
5. Demirjian A, Goldstein H, Tanner JM. A new system of dental age assessment. Hum Biol. 1973; 45(2): 211-27. [ Links ]
6. Blenkin MR, Evans W. Age estimation from the teeth using a modified Demirjian system. J Forensic Sci. 2010; 55(6): 1504-8. [ Links ]
7. Moorrees CF, Fanning EA, Hunt EE, Jr. Age variation of formation stages for ten permanent teeth. J Dent Res. 1963; 42: 1490-502. [ Links ]
8. Olze A, Reisinger W, Geserick G, Schmeling A. Age estimation of unaccompanied minors. Part II. Dental aspects. Forensic Sci Int. 2006; 159 Suppl 1: S65-7. [ Links ]
9. Cunha E, Baccino E, Martrille L, Ramsthaler F, Prieto J, Schuliar Y, et al. The problem of aging human remains and living individuals: A review. Forensic Sci Int. 2009; 193(1): 1-13. [ Links ]
10. AlQahtani SJ, Hector MP, Liversidge HM. Accuracy of dental age estimation charts: Schour and Massler, Ubelaker and the London Atlas. Am J Phys Anthropol. 2014; 154(1): 70-8. [ Links ]
 Correspondence:
Correspondence:
Herman Bernitz
Department of Oral Pathology and Oral Biology, University of Pretoria
Pretoria, South Africa
Email: bernitz@iafrica.com
Author contributions:
1 . Liam Robinson: Principle author - 50%
2 . Chané Nel: Radiographic acquisition and analysis - 20%
3 . Herman Bernitz: Forensic report and advisor - 30%

