










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.75 no.2 Johannesburg Mar. 2020
http://dx.doi.org/10.17159/2519-0105/2020/v75no2a5
NARRATIVE REVIEW
Teething symptoms and management during infancy - A narrative review
YI KarjikerI; JA MorkelII
IBCHD (UWC), Department of Maxillo-Facial and Oral Surgery, Faculty of Dentistry, University of the Western Cape, South Africa. ORCID Number: 0000-0003-4495-3594
IIBChD, MBChB, MChD(Cum Laude), Academic Head: MFOS and Anaesthesioloy & Sedation, Department of Maxillo-Facial and Oral Surgery, Faculty of Dentistry, University of the Western Cape, South Africa. ORCID Number: 0000-0001-8637-5660
ABSTRACT
Even though teething is a normal part of infant development, surprisingly, little is known about the causes and management of its signs and symptoms. Due to the paucity of knowledge in this area, the purpose of this review was to provide clarity on teething symptoms and management options.
A PRISMA flow chart revealed 13 studies that were reviewed which reported on teething symptoms and signs as well as treatment and management options. The databases searched were EMBASE, Medline, PubMed, Google Scholar and the Cochrane Library.
The review showed that although conventional and generic treatment options are constantly in use, there remains no concrete evidence to prove signs and symptoms of teething nor evidence to disprove it. However, in this review, symptoms such as irritability, increased salivation, runny nose, loss of appetite, diarrhoea, rash, sleep disturbance and gum rubbing were most apparent.
Further studies are needed to ascertain these findings objectively and conclusively. Future research is also required to understand and investigate the efficacy of treatment methods and approaches among children with teething symptoms.
Keywords: Teething, infancy, symptoms, treatment, review.
BACKGROUND
The effect of teething on infant health has been debated for at least 5000 years, and traditional beliefs on the issue have still not been entirely supported by scientific literature.1
It is widely believed that pain and other discomfort associated with tooth eruption among infants should and can be managed by pharmacological and non-pharmacological means, but this has yet to be proven.2 The eruption of primary teeth usually begins around 4-8 months of age with the eruption of the lower incisors, and is complete at around 30-36 months of age when second primary molars erupt. However, the timing of tooth eruption varies by as much as six months.3,4
Teething disturbances are transient but may recur repeatedly during 4 to 36 months of age. Evidence regarding teething signs and symptoms are mostly subjective comments from parents, childcare workers and/or health professionals.2,5-12
Generally, studies on teething have been small, retrospective, descriptive and cross-sectional in nature. Studies of larger cohorts13 show no causal association between teething and infection, fever, or diarrhoea.2 In some children, teething may be associated with increased drooling, sucking of digits and rubbing of gingivae. Nevertheless, more recent prospective studies reveal that most systemic teething signs and symptoms (fever, vomiting, facial rashes, sleep disturbances, stool looseness, decreased appetite for liquids, and cough) are due to other causes.14-18
Examples of these alternate causes are well documented in the literature,19-24 and include meningitis, bacterial infections, and herpes simplex virus infections. The latter are painful in their own right.20-23
Teething disturbances may also be caused by development changes, including the decline of maternal antibodies,25-27 while wakefulness and night crying may be due to separation anxiety from a parent or attention seeking.
AIM
Even though teething is a normal part of infant development, surprisingly, little is known about the causes and management of its signs and symptoms. Due to the paucity of knowledge in this area, the purpose of this review was to provide clarity on teething symptoms and management options.
METHODS
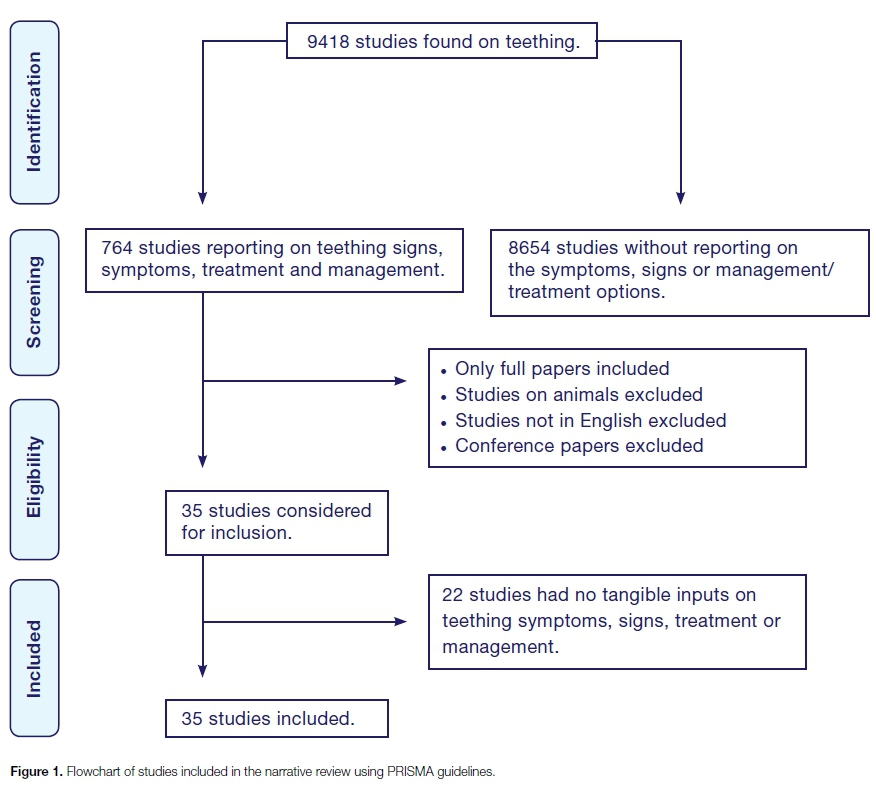
A systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.28
Data Sources and searches
While this was not intended to be a formal systematic review, a search strategy was used to identify the relevant literature. The databases searched were EMBASE, Medline, PubMed, Google Scholar and the Cochrane Library with the keyword search of "teething", "teething symptoms", "teething signs", "teething management", "teething treatment", and "teething children".
A preliminary scoping exercise was undertaken. It indicated that the studies available were too heterogeneous to permit a systematic review or meta-analysis of the interventions developed to tackle the number of children who presented with teething symptoms, eruptions or extractions. Therefore, a narrative review of the literature over a 20-year period (1999-2019) was conducted.
Studies were selected that considered child patients only (as teething symptoms mainly occur between six months and three years of age), had a defined intervention and methodology of patients who presented with varied teething symptoms, a treatment measure, management option or a measured outcome.
The titles and/or abstracts were reviewed to exclude any clearly irrelevant studies. The full texts of the remaining studies were then retrieved and read in full independently to determine whether the studies met the inclusion criteria or not.
Inclusion criteria
In the search, both primary sources and systematic reviews were prioritised as these synthesise the evidence and are at the top of the evidence-based literature as well as studies from the local context. As a second strategy, key scholars from the literature review and institutions were identified, and searched for their recent critical publications, as well as new authors citing them, and which references they had used.
Data extraction and synthesis
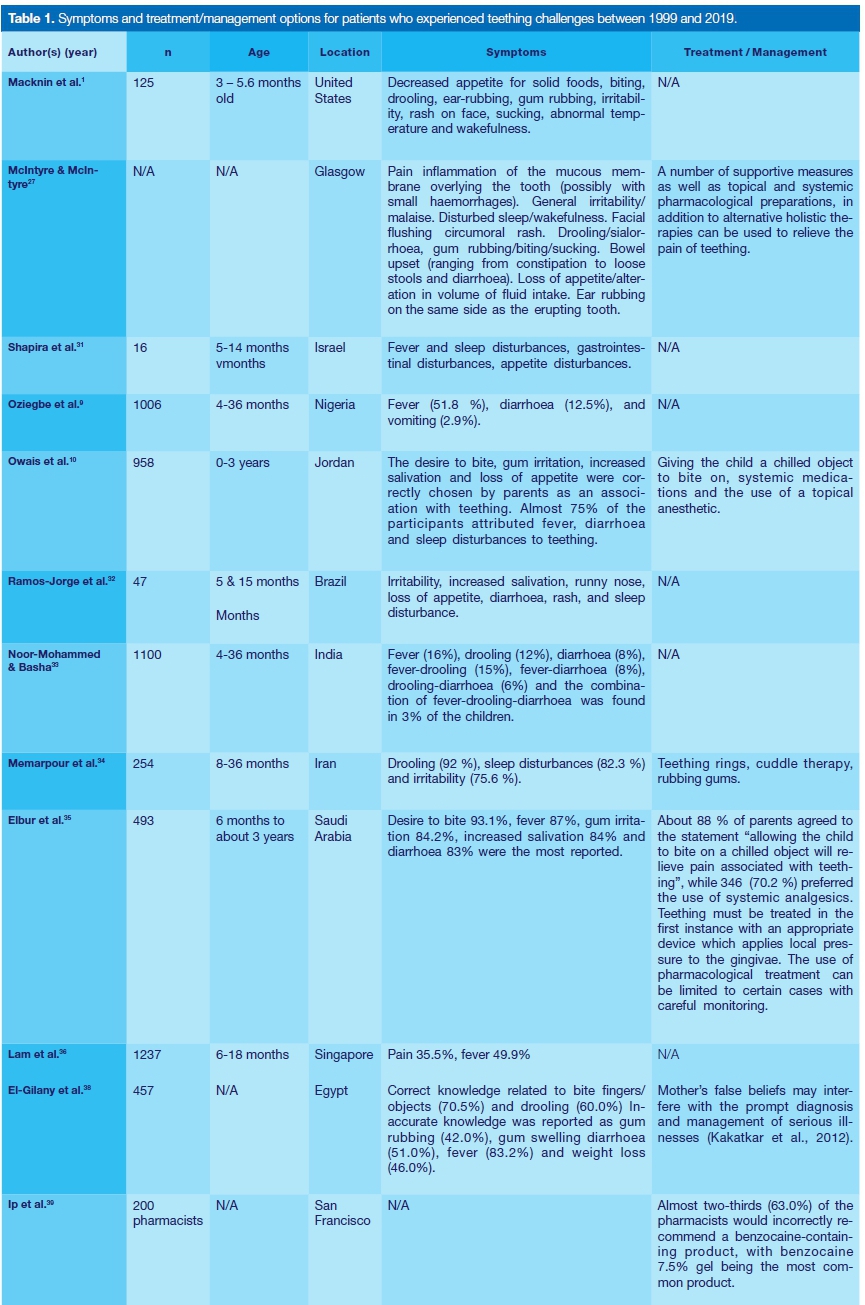
Using a standardised data extraction sheet, the following information (if available) was extracted and recorded from studies: authors and year of publication; sample size of participants; age or age range; location; symptoms and management or treatment options.
Quality assessment
The PRISMA guidelines were used to examine the quality of the studies. These include adequacy of study design; recruitment of sample; and findings. The quality of the studies was not summarised with a score, as this approach has been criticized for allocating equal weight to different aspects of metho-dology,29 but a formal assessment of the risk of bias and strength of evidence according to the Agency for Healthcare Research and Quality (AHRQ) guidelines was conducted.30 A study was considered to be of high quality if the study design was prospective in nature, consecutive or a random sampling method was used.
RESULTS
Study selection
The flowchart is shown in Figure 1 for the study selection of which the literature search resulted in 9418 studies. After a review of their titles and abstracts, 764 studies met the inclusion criteria and were retrieved for full text reading.
Of these, 751 studies were excluded from the narrative review as they no longer met the inclusion criteria. A total of 13 studies were included in the review, and the extracted data are summarized in Table 1.
DISCUSSION
This narrative review investigated the available evidence about primary tooth eruption and local and systemic signs and symptoms, along with treatment and management options.
Signs and symptoms
It is now generally accepted that the eruption of the deciduous teeth is accompanied by a number of relatively minor symptoms (Table 1).27 General irritability, disturbed sleep, gum inflammation, drooling, loss of appetite, diarrhoea, circumoral rash, intra-oral ulcers, and increase in body temperature, increased biting, gum-rubbing, sucking, wakefulness and ear-rubbing, have all been identified as being temporally related to teething (Table 1).27
McDonald et al.,14 described tooth eruption as a physiological process, which does not justify its association with fever and systemic disorders. Fever and respiratory tract infections in this period of life may happen at the same time as eruption but are not associated with it. In the submucosal phase, the number of mast cells is significantly higher than in the intraosseous phase of tooth eruption, and in the submucosa of the normal oral mucosa not associated with teeth. The consequent degranulation and the local release of mediators, such as histamine, leukotrienes, prostaglandins, proteases, cytokines and growth factors, contribute to the understanding of signs and symptoms assigned to tooth eruption, such as itching, inflammation, local redness and sialorrhoea.14
Macknin et al.,1 conducted a prospective study that investigated the symptoms associated with infant teething. It was revealed that tooth eruption is associated with a slight temperature elevation, facial rash, sleep disturbance, and ear rubbing. In their study, symptoms of decreased appetite for solid foods, biting, drooling, ear-rubbing, gum rubbing, irritability, rash on face, sucking, abnormal temperature and wakefulness were found to have some association with the teething process.1
In 2009, Oziegbe et al.,9 conducted a cross-sectional study consisting of 1,013 mothers of children between the ages four to 36 months who visited the immunization clinics at the Community Health Centres in Ife Central and Ife East Local Government areas in Nigeria.
A total of 765 mothers (75.5%) reported systemic signs and symptoms in their children. Fever (51.8%), diarrhoea (12.5%), and vomiting (2.9%) were the most prevalent symptoms and signs reported after eruption. However, there was no association between teething and symptoms such as fever or diarrhoea.9
In another study, most of the children had one or more signs and symptoms during tooth eruption.34 The most frequent teething symptoms were drooling (92%), sleep disturbances (82.3%) and irritability (75.6%).
These symptoms were more pronounced in low birth weight children.34 Low grade increases in body temperature were observed only on the day of eruption (36.70 ±0.39 °C), when body temperature was significantly different compared to the day before and on the day.34
Interestingly, in Singapore, significant early-life factors affecting the child's susceptibility to teething-related pain and fever were commonly reported among infants.36 These factors included infants of Chinese ethnicity, who were exposed to tobacco smoke during pregnancy, had childbirth via Caesarean section and infants that had elevated levels of prenatal plasma vitamin D.36
Much of the information gathered about teething is based on subjective parental information. According to Shapira et al.,31 during the teething period, behavioural problems were observed in 50% of the infants, compared to 16% in the control period p<0.01); fever was observed in 24% of the infants during tooth eruption and in 8% of the infants during the control period (p =.04); and coughing was observed in 12% during tooth eruption compared to 2% (p=0.06) of the infants during the control period. Correlations were also found between high levels of IL-1ß and fever, gastrointestinal disturbances, sleep disturbances, and appetite disturbances.31
During the same period, a correlation was observed between high levels of IL-8 and gastrointestinal disturbances. High levels of Tumour Necrosis Factor (TNF) were also correlated with fever and sleep disturbances. The Gingival Crevicular Fluid (GCF) cytokines were correlated to some of the clinical symptoms of teething. IL-1ß and TNF are correlated with fever and sleep disturbances, IL-1ß and IL-8 with gastrointestinal disturbances, and IL-1ß with appetite disturbances.31
Owais et al.,10 stated that there are side effects from teething, but any real cause-and-effect relationship is doubtful. In addition, it was also postulated that high body temperature (higher than 39°C) should not be attributed to teething and should be further investigated. Plutzer40 conducted a randomized controlled trial on how first-time mothers perceive and deal with teething symptoms. It was revealed that teething symptoms, which are at the very root of the problem, are still poorly understood, despite many commendable efforts over the last 10 years to address them.
Their physiological or pathophysiological basis is not in doubt, butwhat they lead to in terms of discomfort is poorly understood. Partially, this is due to the confusion between the signs and symptoms. Symptoms are what a patient experience, but children getting their first few teeth can only communicate these through signs and signals that their caregivers can interpret.
Memarpour et al.,34 conducted a clinical trial of non-pharmacological remedies with regards to the signs and symptoms associated with primary tooth eruption. It was found that most of the children in the study had one or more signs and symptoms during tooth eruption. The study found that tooth eruption was accompanied by local disturbances such as drooling and the urge to chew on objects.34
An association has also been shown between general objective signs (drooling, fever, and diarrhoea) and the eruption of primary teeth with fever being the most prevalent sign followed by drooling and a fever-drooling combination.33 It was further stated that most signs appeared during the eruption of the primary incisors.33 Furthermore, when an infant at teething age has some symptoms, they may be attributed to teething, but other possible causes must be ruled out first.33
Another study had results that demonstrated associations between teething and sleep disturbance, increased salivation, rash, runny nose, diarrhoea, loss of appetite, irritability, and a slight rise in temperature.32 These associations were significant on the day of eruption and one day after eruption. Therefore, it is not possible to predict eruption through the observation of signs and symptoms because there were no associations on the day before eruption.
The findings of this study contribute towards supporting the concept that teething is not associated with severe signs and symptoms. Therefore, health professionals involved in the care of infants should seek other causes before attributing severe signs and symptoms to teething.32
Based on the current limited evidence by Massignan et al.,37, there are signs and symptoms during primary tooth eruption. Gingival irritation, irritability, and drooling were the most common.
For body temperature analyses, it was possible to evaluate that eruption of primary teeth is associated with a rise in temperature, but it was not characterized as fever. There are also results which showed a wide gap in knowledge and misconceptions with regards to the ascribed signs and symptoms and practices used to manage infant teething problems.35
Treatment and management options
Aside from teething signs and symptoms, there has been a number of recommended options suggested for management and treatment.
El-Gilany et al.,38 studied mothers' teething beliefs and treatment practices in Egypt. Their study showed that 13.6% of mothers did not give any treatment for teething problems. Analgesics/antipyretics, pacifiers and antibiotics were the most frequently given treatments (71.3%, 31.3% and 24.3%; respectively).
Relatives, friends and health care workers were the most frequent source of mothers' information about teething problems and their treatments. Deciduous tooth eruption has already been inaccurately associated with several health disorders, such as sleep disruption, ear and cheek itching, primary herpetic gingivostoma-titis, cough, croup, bronchitis, diarrhoea, fever, convulsions and (in severe cases) even death.
Objectively, Memarpour et al.,34 presented two main methods - pharmacological and nonpharmacological -which have been recommended as treatments during tooth eruption. Non-pharmacological remedies were used because of the parents' attitudes towards using remedies which do not threaten their child's health. According to their results, some methods such as teething rings, cuddle therapy and rubbing the gums were more effective than others. However, none of the methods was completely effective in dealing with all the teething problems that was reviewed.
Teething rings and rubbing the gums reduced gingival irritation and finger sucking. in the present study.3 The pressure caused by biting teething rings or pacifiers and gingival massage may decrease pain by overwhelming the sensory receptors. Biting or sucking cold or frozen objects including fruits, vegetables or other foods causes localised vasoconstriction and decreases inflammation; in addition, the pressure on the gums reduces pain. However, it is suggested that these remedies should be used only for children who are able to eat solid foods. Also, foods that are very hard should not be used, to avoid pain caused by bruising the gum.4 Moreover, parental supervision is needed to prevent choking on small pieces of food.34
In 2018, Ip et al.,39 mentioned that the Food and Drug Administration (FDA) issued a warning to avoid the use of any benzocaine-containing products for infant teething treatment owing to a risk of methaemoglobi-nemia. Despite the release of this drug safety warning regarding the use of benzocaine-containing products in infant teething treatment, the majority of pharmacists in their study indicated that they would still incorrectly recommend a benzocaine containing product. Further education is warranted to ensure that all pharmacists, health care providers, and consumers are aware to avoid benzocaine, viscous lidocaine, and homeopathic products for infant teething treatment.
Limitations
This study has several limitations. The included studies were not specifically designed to answer prospectively the question as to what tangible symptoms and signs as well as treatment options there are for teething and, therefore, a large diversity in studies, study designs, patient categories with different diagnoses, definitions, subjective insights from parents and severity of teething were combined.
Some studies with a low sample number were also included as it matched the inclusion criteria either for children who presented with signs and symptoms of teething, or where there were adequate options for treatment and management of teething. Due to the limited number of studies included in the review, the findings from this study are not generalizable to a number of population groups and patient settings.
CONCLUSION
This review has shown that although conventional and generic treatment options are constantly in use, there still remains no concrete evidence to prove signs and symptoms of teething nor evidence to disprove it. However, in this review, symptoms such as irritability, increased salivation, runny nose, loss of appetite, diarrhoea, rash, sleep disturbance and gum rubbing were most apparent. Further studies are needed to ascertain these findings objectively and conclusively. Future research is also required to understand and investigate the efficacy of treatment methods and approaches among children with teething symptoms.
Funding
The authors have no financial interests to declare. No external funding given to the work.
Declaration
Authors have no potential conflict of interest to declare.
Compliance with ethical standards
This research is compliant with ethical research standards.
Ethical approval
Ethical approval for this type of study and formal consent is not required. This article does not contain any studies with humans or animals performed by any of the authors.
References
1. Macknin ML, Piedmonte M, Jacobs J, Skibinski C. Symptoms associated with infant teething: a prospective study. Pediatr. 2000; 105(4): 747-52. [ Links ]
2. Tsang AK. Teething, teething pain and teething remedies. Int Dent South Africa. 2010; 12(5): 48-61. [ Links ]
3. Marks, SC. The basic and applied biology of tooth eruption. Conn Tiss Res. 1995; 32(1-4): 149-57. [ Links ]
4. Wise GE, Marks SC, Zhao L. Effect of CSF-1 on in vivo expression of c-fos in the dental follicle during tooth eruption. Eur J Oral Sci. 1998; 106 (Suppl. 1): 397-400. [ Links ]
5. Peretz B, Ram D, Hermida L, Otero MM. (2003). Systemic manifestations during eruption of primary teeth in infants. J Dent Child (Chic). 2003; 70(2): 170-3. [ Links ]
6. Baykan Z, Shin F, Beyazova U, Ozcakar B, Baykan A. Experience of Turkish parents about their infants' teething. Child Care Health Dev. 2004; 30(4): 331-6. [ Links ]
7. Cunha RF, Pugliesi DM, Carvalho G, Dias L, Murata SS. Systemic and local teething disturbances: prevalence in a clinic for infants. J Dent Child. 2004; 71(1): 24-6. [ Links ]
8. Denloye O, Bankole OO, Aderinokun GA. Teething myths among community health officers. Odonto-Stomatol Trop. 2005; 28(109): 19-22. [ Links ]
9. Oziegbe EO, Folayan MO, Adekoya-Sofowora CA, Esan TA, Owotade FJ. Teething problems and parental beliefs in Nigeria. J Contemp Dent Pract. 2009; 10(4): 75-82. [ Links ]
10. Owais AI, Zawaideh F, Bataineh O. Challenging parents' myths regarding their children's teething. Int J Dent Hyg. 2010; 8(1): 28-34. [ Links ]
11. Wake M, Hesketh K., Lucas J. Teething and tooth eruption in infants: a cohort study. Pediatr. 2000; 106(6): 1374-479. [ Links ]
12. Markman L. Teething: facts and Action. Pediatr Rev. 2009; 30(8): e59-e64. [ Links ]
13. Tasanen A. General and local effects of the eruption of deciduous teeth. Ann Paediatr Fenn. 1968; 14(Suppl 29): 1- 40. [ Links ]
14. McDonald RE, Avery DR, Dean JA. Eruption of the teeth: local, systemic and congenital factors that influence the process. In: Dean JA, McDonald RE, Avery DR. (Eds). Dentistry for the child and adolescent. 9th ed. St Louis: Mosby. 2010. 155-76. [ Links ]
15. Wake M, Hesketh K. Teething symptoms: cross sectional survey of Ave groups of child health professionals. Brit Med J. 2002; 325: 814. [ Links ]
16. Sarrell EM, Horev Z, Cohen Z., Cohen HA. Parents' and medical personnels' beliefs about infant teething. Patient Educ Couns. 2005; 57(1): 122-5. [ Links ]
17. Seward MH. The treatment of teething in infants. Brit Dent J. 1972; 132: 33-6. [ Links ]
18. Jaber L, Cohen IJ, Mor A. Fever associated with teething. Arch Dis Child. 1992; 67(2): 233-4. [ Links ]
19. Swann IL. Teething complications, a persisting misconception. Postgrad Med J. 1979; 44(639): 24-5. [ Links ]
20. King DL, Steinhauer W, Garcia-Godoy F, Elkins, CJ. Herpetic gingivostomatitis and teething difficulties in infants. Pediatr Dent. 1992; 14: 82-5. [ Links ]
21. King DL. Teething revisited. Pediatr Dent. 1994; 16(3): 179-82. [ Links ]
22. Pruksananonda P, Hall CB, Insel RA, McIntyre K., Pellett PE, Long CE, Schnabel KC, Pincus PH, Stamey FR, Dambaugh TR. et al. Primary human herpesvirus 6 infection in young children. New Engl J Med. 1992; 326(22): 1445-50. [ Links ]
23. De Bolle L, Neasens L, De Clercq E. Update on human herpesvirus 6 biology, clinical features and therapy. Clin Microbiol Rev. 2005; 18(1): 217-45. [ Links ]
24. Zerr DM, Meier AS, Selke SS, Frenkel LM, Huang ML, Wald A, Rhoads MP, Nguy L, Bornemann R, Morrow RA, Corey L. A population-based study of primary human herpesvirus 6 infection. New Engl J Med. 2005; 352(8): 768-76. [ Links ]
25. Castiglia PT. Teething. J Pediatr Health Care. 1992; 6(3): 153-4. [ Links ]
26. Schechter NL. Management of common pain problems in the primary care pediatric setting. In: Schechter NL, Berde CB, Yaster M. (Eds). Pain in infants, children and adolescents. 2nd ed. Philadelphia: Lippincott Williams & Wilkins. 2003. 693-706. [ Links ]
27. McIntyre GT, McIntyre GM. Teething troubles? Brit Dent J. 2002; 192(5): 251-5. [ Links ]
28. Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009; 6:e1000097. [ Links ]
29. Jüni P, Altman DG, Egger M. Systematic reviews in health care: assessing the quality of controlled clinical trials. Brit Med J. 2001; 323: 42-6. [ Links ]
30. Owens DK, Lohr KN, Atkins D. AHRQ series paper 5: grading the strength of a body of evidence when comparing medical interventions - agency for healthcare research and quality and the effective healthcare program. J Clin Epidemiol. 2010; 63: 513-23. [ Links ]
31. Shapira J, Berenstein-Ajzman G, Engelhard D, Cahan S, Kalickman I, Barak V. Cytokine levels in gingival crevicular fluid of erupting primary teeth correlated with systemic disturbances accompanying teething. Pediatr Dent. 2003; 25(5): 441- 8. [ Links ]
32. Ramos-Jorge J, Pordeus IA, Ramos-Jorge ML, Paiva SM. Prospective longitudinal study of signs and symptoms associated with primary tooth eruption. Pediatr. 2011; 128(3): 471- 6. [ Links ]
33. Noor-Mohammed R, Basha S. Teething disturbances; prevalence of objective manifestations in children under age 4 months to 36 months. Med Oral, Patol Oral Cir Bucal. 2012; 17(3): e491. [ Links ]
34. Memarpour M, Soltanimehr E, Eskandarian T. Signs and symptoms associated with primary tooth eruption: a clinical trial of nonpharmacological remedies. BMC Oral Health. 2015; 15(1): 88. [ Links ]
35. Elbur AI, Yousif MA, Albarraq AA, Abdallah MA. Parental knowledge and practices on infant teething, Taif, Saudi Arabia. BMC research notes. 2015; 8(1): 699. [ Links ]
36. Lam CU, Hsu CY, Yee R, Koh D, Lee YS, Chong MF, Cai M, Kwek K, Saw SM, Gluckman P, Chong YS. Early-life factors affect risk of pain and fever in infants during teething periods. Clin Oral Inv. 2016; 20(8): 1861-70. [ Links ]
37. Massignan C, Cardoso M, Porporatti AL, Aydinoz S, Canto GD, Mezzomo LA, Bolan M. Signs and symptoms of primary tooth eruption: a meta-analysis. Pediatr. 2016; 137(3): e20153501. [ Links ]
38. El-Gilany AH, Abusaad FE. Mothers' teething beliefs and treatment practices in Mansoura, Egypt. Saud Dent J. 2017; 29(4): 144-8. [ Links ]
39. Ip EJ, Patel PB, Chi JJ, Shah-Manek B, Lau B. What are pharmacists recommending for infant teething treatment? J Amer Pharm Ass. 2018; 58(1): 79-83. [ Links ]
40. Plutzer K, Spencer AJ, Keirse MJ. How first-time mothers perceive and deal with teething symptoms: a randomized controlled trial. Child: care, health and dev. 2012; 38(2): 292-9. [ Links ]
 Correspondence:
Correspondence:
Yunus I Karjiker
Department of Maxillo-Facial and Oral Surgery
Faculty of Dentistry, University of the Western Cape
South Africa
Email: ykarjiker@gmail.com
Author contributions:
1 . Yunus I Karjiker: Primary author - 60%
2 . Jean A Morkel: Secondary author - 40%


{kind=link}
{kind=link}