










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.74 n.9 Johannesburg Oct. 2019
http://dx.doi.org/10.17159/2519-0105/2019/v74no9a8
CLINICAL WINDOW
What's new for the clinician: excerpts from and summaries of recently published papers
Veerasamy Yengopal
BChD, BScHons, MChD, PhD, Community Dentistry Department, School of Oral Health Sciences, University of Witwatersrand, Medical School, no. 7 York Road, Parktown 2193, South Africa. ORCID Number: 0000-0003-4284-3367 Email: veerasamy.yengopal@wits.ac.za
1. Is it advisable to extend curing times beyond the manufacturer's recommendation?
M Par, I Repusic, H Skenderovic, et al. Clin Oral Invest. (2019) 23: 3777-88.
The development of high-irradiance light-emitting diode (LED) curing units has led to the shortening of time recommended for light-curing of composite materials for direct restorations.1 This has been used as a marketing tool to appeal to the practitioner's demands for time saving. Concerns about whether the curing time recommended by manufacturers is sufficient for adequate polymerization at the restoration bottom have been raised due to the evidence of inferior cure produced by adhering to the manufacturer guidelines regarding layer thickness, curing unit irradiance, and curing time.1
Additionally, it has been noted that the curing time advertised by manufacturers is usually the minimum time required for a sufficient cure in controlled laboratory conditions and may not not necessarily be optimal for the more complex clinical setting.1 Clinically, this has often led to fracture of the restoration and sensitivity and other adverse effect in the patients.
The simplest way a practitioner can overcome these issues is by extending the curing time beyond manufacturer recommendations; this approach has been shown to improve the degree of conversion and micro-hardness at the bottom of the composite layer.1 Also, extended curing time may help to mitigate the effect of spatial heterogeneity of the curing unit beam, thus producing more uniformly cured restorations.1
However, curing with high-irradiance units for extended time raises concerns regarding possible overheating of the dental pulp. Par and colleagues (2019)1 from Croatia investigated radiant energy, microhardness, and temperature rise in eight composite materials at layer thicknesses of 2 mm and 4 mm. A blue and a violet-blue LED curing
unit were activated for the longest curing "program" available (30 s), delivering radiant energies which exceeded most of the manufacturer recommendations. The null hypotheses assumed no effect of composite material, curing unit, and layer thickness on (1) radiant energy, (2) Vickers microhardness (MH), and (3) temperature rise at the bottom of the composite layer, (4) no correlation between radiant energy and MH and (5) no correlation between radiant energy and temperature rise.
ACRONYMS
LED: Light-Emitting Diode
MW: Monowave
PET: Polyethylene Terephthalate
PW: Polywave
TEC: Tetric EvoCeram
TECBF: Tetric EvoCeram Bulk Fill
MH: Vickers MicroHardness
MATERIALS AND METHODS
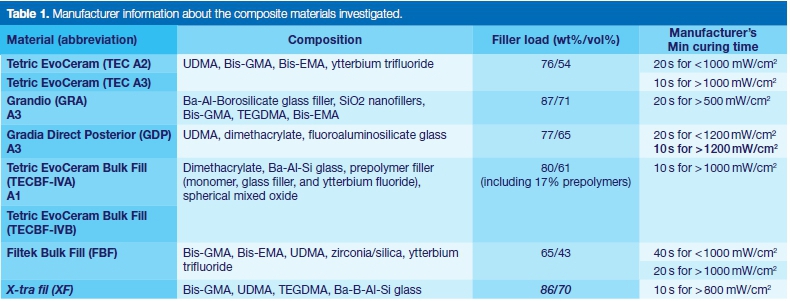
Four conventional and four bulk-fill resin composites were investigated. Detailed composition and manufacturer recommendations for curing time are shown in Table 1.
To evaluate the effect of pigment additives used for the adjustment of shade, composites Tetric EvoCeram (TEC) and Tetric EvoCeram Bulk Fill (TECBF) were investigated in two different shades. These composite types also contained additional photoinitiators besides camphorquinone/amine. Composite specimens were light-cured using either a blue or a violet-blue curing unit. The blue curing unit is also known by the name "Monowave" (MW), while the violet-blue is referred to as "Polywave" (PW).
To determine the radiant energy delivered to the bottom of 2mm and 4mm-thick composite layers, the light intensity which passed through the mould aperture was measured by integrating sphere (IS, Gigahertz Optik), and real-time monitoring of the light transmittance during light-curing of composite specimens was performed using a charge-coupled device array fibre spectrometer.
Composite specimens were prepared in black cylindrical Teflon moulds (d =8 mm, h =2 or 4 mm), covered with a polyethylene terephthalate (PET) film, and light-cured for 30 s. The light transmitted through the specimen during the light-curing was collected by a lens and led to the spectrometer which recorded irradiance as a function of time at the data collection rate of 20 s-1 using custom-made software. Radiant energy (J/cm2) was calculated by integrating the area under the irra-diance vs. time curve.
For MH measures, composite specimens of the same geometry as described for the radiant energy measurements (d =8 mm, h = 2 or 4 mm) were prepared by pressing composite pastes in black Teflon molds, covering mould apertures with a PET film and light-curing for 30 s. The specimens were then stored in dark at 37± 1°C for 24h in order to complete the post-cure reaction.
Microhardness (MH) was evaluated at specimen surface (designated as 0 mm) and at the bottom of 2mm or 4mm-thick specimens. Vickers MH was calculated using the following equation: MH = 1.8544 χ F/d2, where d is the indentation diagonal and F= mxg (g = 9.81 N/kg, m = load).
For temperature rise measures, composite specimens (d = 8 mm, h = 2 or 4 mm) were prepared in the same black Teflon moulds as had been used for radiant energy and MH measurements. Temperature rise was monitored in real time during the light-curing of 30 s by means of a T-type thermocouple which was positioned centrally at the bottom of composite specimens. The environmental temperature during all the tests was 22 ± 1°C. For each test, Ave specimens per experimental group were prepared (n = 5).
RESULTS
Radiant energy delivered from the blue and violet-blue curing unit amounted to 19.4 and 28.6 J/cm2, which was 19% and 13% lower than specified by the manufacturer. Radiant energies at bottom surfaces (0.2-7.5 J/cm2) were significantly affected by material, thickness, and curing unit.
Curing time, which seems "extended" considering the manufacturer guidelines, was in fact adequate for producing the recommended radiant energies.
All of the composites reached 80% of maximum micro-hardness at clinically relevant layer thicknesses. The benefit of using the higher-irradiance violet-blue curing unit was identified only in composites containing alternative photo-initiators. Temperature rise during curing ranged from 4.4°C to 9.3°C and was significantly reduced by curing with the lower-intensity blue curing unit and by increasing layer thickness.
CONCLUSION
Within the limitations of this study which evaluated radiant energy, curing efficiency, and temperature rise in composites which were light-cured for 30s using a blue (648mW/cm2) and a violet-blue (924mW/cm2) LED curing unit, the following can be concluded:
1. Curing with the lower-intensity curing unit produced less heat, whereas both curing units produced adequate cure at 2 mm for conventional composites and 4 mm for bulk-fill composites.
2. The conventional composites containing combined photo-initiators benefitted from the use of violet-blue curing unit, while no benefit was identified in two bulk-fill composites with combined photo-initiators.
3. Thicker composite layers may protect the pulp from thermal insult by producing lower temperature rise at the layer bottom.
4. Temperature rise was mainly determined by radiant energy, suggesting that thermal hazard can be controlled by limiting curing parameters to optimal values.
5. Most of the temperature rise occurred within 5-10 s after the start of light-curing; extending the curing time to 30s resulted in a minor additional increase.
Implications for practice:
It appears that many manufacturers underestimate the optimal curing times for their materials. It seems reasonable to allow for a 30s cure time especially for thick/ bulky composites.
Reference
1. Par M, Repusic I, Skenderovic H, et al. The effects of extended curing time and radiant energy on microhardness and temperature rise of conventional and bulk-fill resin composites. Clin Oral Invest. (2019) 23: 3777-88. [ Links ]
2. Modified vs. standard hall technique in a paediatric dentistry setting R Midani, CH Splieth, M Mustafa Ali, J Schmoeckel, SM Mourad, RM Santamaría. Int J Paediatr Dent. 2019; 29: 550-56.
A large number of studies have compared different therapeutic approaches and materials for restoring primary teeth, showing that the longevity of a restoration is a critical factor in determining treatment success.1
Therefore, preformed metal crowns (PMCs) are continually recommended in the literature for treating primary teeth with multi-surface carious lesions and after pulp therapy in high-risk children.1
About a decade ago, a different way of using PMCs - the 'Hall Technique' (HT) - was published. This particular technique has been used primarily to treat carious primary molars, but without caries removal, tooth preparation, or the use of local anaesthesia.
Since then, different clinical trials have been performed in order to prove the effectiveness of the technique, including a comparison of the Hall Technique with more conventional treatment options such as fillings. Midani and colleagues (2019)1 reported on a trial that sought to compare the conventional and modified Hall techniques of preparing and placing PMCs in primary molars.
METHODS AND MATERIALS
This retrospective study relied on the electronic records of patients who had received preformed metal crowns using the Hall Technique over a Ave year period in Germany. Inclusion criteria were healthy children between two and 11 years old, no reported baseline clinical or radiographic signs or symptoms of pulpal or peri-radicular pathology, a follow-up period of at least six months, and sufficient documentation.
Only one crown per child was included. In cases where a child had had more than one tooth treated with the HT and was eligible for inclusion, the tooth with the longest follow-up period was selected. If more than one Hall crown was performed at the same appointment, the crown of interest was randomly selected.
Recorded clinical data comprised all baseline and recall intraoral examinations, including age (years), gender, teeth treated, and caries levels (d3mft/D3MFT). In addition, initial non-cavitated carious lesions were recorded (d1-2mft/D1-2MFT), as well as any available radiographs.
ACRONYMS
HT: Hall Technique
PMCs: Preformed Metal Crowns
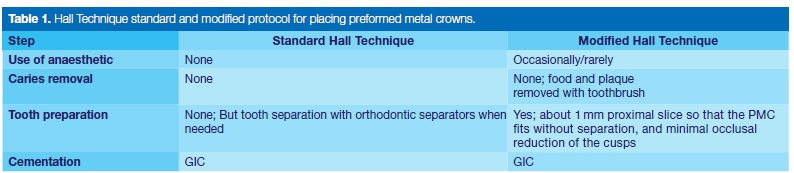
A total of 29 treating dentists (specialists n = 9; postgraduate students n =20) performed two different protocols to apply the PMCs: the standard Hall Technique and the modified Hall Technique.
The latter involved proximal tooth slicing, allowing the PMC to fit without separation and providing minimal reduction of occlusal cusps, but, however, without caries removal (Table 1).
The techniques were performed in different settings, for example, chairside, under sedation (nitrous oxide), or general anaesthesia. Outcome measures were assessed according to the following criteria:
• Success: Crown present and appears satisfactory; no intervention was required during the follow-up period. No clinical or radiographic signs or symptoms of pulpal pathology occurred.
• Minor failure: New caries (around margins), crown perforation, crown loss but the tooth is restorable. Signs or symptoms of reversible pulpitis (no spontaneous pain) treated without requiring pulpotomy or extraction.
• Major failure: Irreversible pulpitis (history of spontaneous pain or pain caused by thermal or other stimuli) or dental abscess requiring pulpotomy or extraction. Crown loss and tooth is unrestorable.
RESULTS
In total, 192 children received 295 Hall crowns during the study period. Of these, data from 181 children with sufficient documentation were included for further analysis. The majority of Hall crowns were placed in boys (60.8%; n = 110).
Patients' mean age when the crown was performed was 5.9 ±1.84, mean d3mft/D3MFT was 6.55 ±3.48/ 0.18 ±0.66 and when initial carious lesions were included, the d1-2mft/D1-2MFT was 7.83 ± 3.71/0.17 ± 0.65. The average follow-up period was 22.62 months (range: 6.01-89.07).
The majority of crowns (71.3%; n = 129 crowns) were placed following the standard Hall Technique protocol and 28.7% (n = 52) were placed using the modified technique. Local anaesthesia was used in 53.8% of the cases (n=28) in the modified technique due to reported pain.
Of these, 57.1% (n=16) were performed chairside and 42.9% (n = 12) on children receiving nitrous oxide sedation. Baseline diagnostic radiographs (mainly panoramic radiographs [OPG]) were available for 69.6%
(n=126) of the teeth.
Most children (80.7%; n=146) were treated chairside, 12.7% (n=23) under nitrous oxide sedation, and 6.6% (n=12) under general anaesthesia (GA). The standard Hall Technique was mostly performed chairside (85.3%; n=110). All Hall crowns placed under GA were performed following the standard technique protocol (9.3%;
n = 12).
Mandibular first molars were the most frequently treated teeth with the Hall Technique (36.5%; n=48); the least frequently treated were mandibular second molars (12.7%; n = 23).
During the follow-up period, the total success rate (standard HT + modified HT) was 92.3% (n = 167). In a single analysis, the success rate of the standard HT was 91.5% (n = 118) and the modified HT 94.2% (n=49). No statistical significance was found when the two methods were compared (P=0.44), even when the use of local anaesthesia (P =0.64) was considered.
In total, four crowns (2.2%) presented with minor failures (crown lost) during the follow-up period and recemen-tation were needed. All crowns presenting with minor failures had been performed with the standard HT.
In total, ten major failures were observed; the reasons were abscess/fistula or irreversible pulpitis/radiographic evidence of an apical radiolucency (5 cases or 2.8% each; Table 5). Failures with standard vs. modified HT did not show a statistically significant difference (P =0.25).
More than two-thirds of the children (n = 129; 69.6%) had diagnostic radiographs taken prior to treatment. There was however no statistically significant difference in the failure rates of teeth diagnosed at baseline with or without radiographs (P= 0.30).
In addition, no significant differences between the three groups were observed for dentist's experience level (specialist or postgraduate student: P =0.24, CI = 1.52-1.66), tooth type (first or second primary molars: P =0.484, CI = 2.31-2.61), or the setting (chair side, nitrous oxide sedation, or general anaesthesia: P=0.408, CI = 1.181.34).
The overall cumulative survival rate was 92.3% with no statistically significant differences between the standard and the modified Hall Technique (P = 0.56). The cumulative rates of minor and major failures combined were 5.8% for the modified HT (n =3) and 8.5% for the standard HT (n = 11).
CONCLUSION
The survival rate and clinical efficacy of Hall crowns (both modified and standard) were high in a secondary care-based setting. The Hall Technique is an effective and less invasive management option for asymptomatic carious primary molars.
Implications for practice
This study highlights the efficacy of Hall crowns as a long-term, durable, and successful technique for asymptomatic carious primary molars. This study also showed that the Hall Technique can be successfully used by dentists with different levels of expertise (postgraduate students/specialists) and in different treatment settings (chairside/under nitrous oxide sedation/ general anaesthesia).
Reference
1. Midani R, Splieth CH, Mustafa Ali M, Schmoeckel J, Mourad SM, Santamaría RM. Success rates of preformed metal crowns placed with the modified and standard Hall technique in a paediatric dentistry setting. Int J Paediatr Dent. 2019; 29: 550-6. [ Links ]


{kind=link}
{kind=link}