










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.74 n.8 Johannesburg Sep. 2019
http://dx.doi.org/10.17159/2519-0105/2019/v74no8a5
CLINICAL WINDOW
What's new for the clinician: excerpts from and summaries of recently published papers
Veerasamy Yengopal
BChD, BScHons, MChD, PhD, Community Dentistry Department, School of Oral Health Sciences, University of Witwatersrand, Medical School, no. 7 York Road, Parktown 2193, South Africa. ORCID Number: 0000-0003-4284-3367 Email: veerasamy.yengopal@wits.ac.za
1. Efficacy of Endo-Ice followed by intrapulpal ice application as an adjunct to inferior alveolar nerve block in patients with symptomatic irreversible pulpitis - a randomized controlled trial
Koteeswaran V, Ballal S, Natanasabapathy V, Kowsky D. Clin Oral Invest. 2019; 23: 3501.
Endodontic treatment among patients with symptomatic irreversible pulpitis (SIP) in lower molars is often associated with pain as the failure rate of the inferior alveolar nerve block (IANB) ranges between 44% and 81%.1
A wide range of additional methods have been employed to improve the anesthetic efficacy of IANB in SIP. The percentage of success of these techniques is highly variable.
The techniques include the use of pre-anesthetic medication, increasing the volume of anaesthesia, intra-mucosal administration of drugs like ketorolac, tramadol, and magnesium sulphate, adding mannitol to ligno-caine, intraosseous, intraligamentary, and intrapulpal anesthetic injections.1
Cryoanalgesia has been successfully used in the field of medicine for managing both acute and chronic pain. The application of cold decreases the tissue temperature, resulting in vasoconstriction, reduction in the tissue metabolites, and downregulation of inflammatory mediators and neuropeptides, thereby reducing pain.
Cryoanalgesia is a simple, relatively inexpensive and non-invasive adjuvant for pain management. Cryoanalgesia has numerous applications in dentistry. Topical cold application (in the form of Endo-Ice) at the injection site prior to palatal anaesthesia has been employed to reduce the pain on injection. However, to date, there are no clinical trials evaluating the effect of cold when used for supplementary anaesthesia in reducing intraoperative pain during pulp extirpation. Koteeswaran and colleagues (2019)1 reported on a trial that sought to evaluate the efficacy of Endo-Ice followed by intrapulpal ice application for relieving pain during pulp extirpation in mandibular molars with symptomatic irreversible pulpitis (SIP). The secondary objective was to evaluate the effect of Endo-Ice followed by intrapulpal ice application in reducing dental anxiety.
ACRONYMS
DAS-R: Corah's Dental Anxiety Scale-Revised
IAN: Inferior Alveolar Nerve Block
SIP: Symptomatic Irreversible Pulpitis
MATERIALS AND METHODS
After initial screening of 94 patients, a total of 60 patients who met the inclusion criteria participated in this randomized controlled single blinded study. Baseline parameters such as age, gender, vitality status, pre-operative pain, and dental anxiety scores were recorded prior to treatment.
The level of pre- and post-intervention pain was recorded as a continuous data using simple Visual Analogue Scale (VAS). The VAS consisted of a line of 10cm length anchored by two extremes with 0 signifying no pain and 10 representing the worst pain imaginable. The dental anxiety of the patient was measured using the Corah's Dental Anxiety scale-revised (DAS-R) before and after intervention.
Patients were included into this randomized single-blind controlled trial if they were diagnosed with SIP planned for endodontic treatment in mandibular molars, were within the age group of 20-50 years with a preoperative VAS score > 4 (Moderate to severe pain). Patients not willing to participate in the study, age > 50 years, patients who reported with a history of pain on cold application, immature young permanent teeth, teeth that did not respond to traditional vitality tests, acute apical abscess, calcified pulp chamber and root canals, previously filled root canals, chronic apical abscess with or without sinus, periodontally compromised teeth, cases of necrotic pulp, medically compromised patients, patients with a history of intake of analgesics, steroids, and/or antibiotics in the recent past 48 h were excluded.
Patients were randomly assigned to any of the three following groups:
• Control group (IANB): Standard inferior alveolar nerve block was administered using a self-aspirating 27-gauge needle with 2 ml of 2% lignocaine hydrochloride with adrenaline 1:80000 (Lignospan Special, Septodont).
• Articaine group (IANB-A): Inferior alveolar nerve block was administered as described in the control group. Supplementary buccal infiltration with 2 ml of 4% arti-caine with adrenaline 1:100000 (Septanest, Septodont) was administered in the mucobuccal fold using a self-aspirating 27-gauge needle against the tooth of interest, deposited over a period of 2min (1 ml/min).
• Cold group (IANB-C): Standard IANB was administered as described previously. Two forms of cold (Endo-Ice and Ice sticks) were used. Prior to access opening, Endo-Ice was applied on the buccal, lingual (three seconds per surface), and occlusal surfaces (four seconds) for a total of 10 seconds and access opening was performed immediately. The pulp was exposed and deroofing was done. Following which, Ice sticks (8 m diameter and 2 cm length) were carried with the help of a tweezer and directly placed on the pulp chamber for a period of four minutes (two Ice sticks for two minutes each).
In all the groups, topical anesthetic gel (20% benzocaine) was applied for 60 seconds at the site of injection prior to administration of IANB.
Throughout the trial, the patients were asked to quantify the level of pain to the outcome assessor at 3 intervals, i.e., preoperative, during access opening and immediately after pulp extirpation. The root canals were medicated with Calcium hydroxide and temporarily sealed with IRM.
The patients were given the DAS-R questionnaire and their level of anxiety was noted. The endodontic treatment was completed one week later. Patients who required additional anaesthesia during treatment were administered intraligmentary injection and intrapulpal injection (if required) and were excluded for final analysis.
RESULTS
A total of 60 patients were included for the final analysis (32 females and 28 males). The baseline parameters including age, gender, and preoperative VAS score and dental anxiety scores were not statistically significant among the three groups (p > 0.05).
The mean VAS score during access opening was least for articaine followed by cold and control group (p value = 0.02). However, there was no significant mean difference in VAS values between cold and control group (p value = 0.95). The mean VAS scores during pulp extirpation were higher in the control group compared with the cold group and articaine group (p value = 0.001).
The difference in the VAS scores between the two test groups during pulp extirpation was statistically insignificant (p value = 0.99). Further, cold significantly reduced the level of anxiety when compared with the articaine or control group (p value=0.001).
CONCLUSIONS
The authors concluded that the Endo-Ice application on the tooth surface did not produce adequate anaesthesia during access opening when compared with buccal infiltration with articaine. However, supplementary buccal infiltration with articaine or intrapulpal ice application improved anaesthesia during pulp extirpation in symptomatic irreversible pulpitis (SIP). Additionally, cold significantly reduced the dental anxiety after treatment.
Implications for practice:
Cold may be considered as a simple, cost-effective, chairside supplementary anesthetic technique for effective management of endodontic pain and anxiety.
Reference
1. Koteeswaran V, Ballal S, Natanasabapathy V, Kowsky D. Efficacy of Endo-Ice followed by intrapulpal ice application as an adjunct to inferior alveolar nerve block in patients with symptomatic irreversible pulpitis - a randomized controlled trial. Clin Oral Invest. 2019; 23: 3501. [ Links ]
2. Esthetic, clinical, and radiographic outcomes of two surgical approaches for single implant in the esthetic area - one-year results of a randomized controlled trial with parallel design
Huynh-Ba G, Hoders AB, Meister DJ, Prihoda TJ, Mills MP, Mealey BL, Cochran DL. Clin Oral Implants Res. 2019; 30: 745-59.
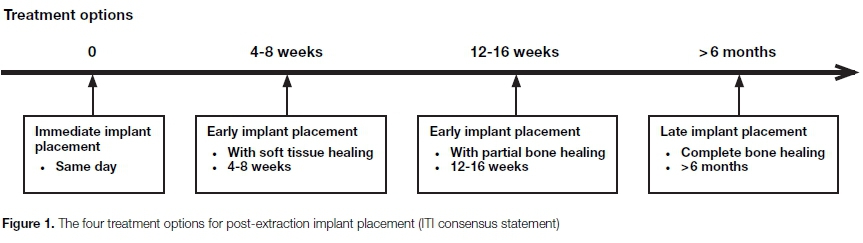
The timing of implant placement in relation to tooth extraction remains a topic of much debate. A consensus conference of the International Team for Implantology (ITI) defined four types of implant placement (Type 1 to Type 4) based on the amount of healing time and the corresponding soft and hard tissue healing obtained following tooth extraction (Figure 1).
Studies suggested that similar implant survival rates can be obtained irrespective of timing of implant placement.
However, the emphasis on aesthetic outcomes in determining clinical success has gradually increased over the years, leading to the development of tools allowing the assessment of implant-supported restoration aesthetics.
Among existing objective aesthetic parameters, those fre-quently used include the pink and white aesthetic scores (PES/WES) and the mid-facial marginal soft tissue level.
Huynh-Ba and colleagues (2019)1 reported on their follow-up data at one year following final crown delivery, comparing aesthetic, clinical, and radiographic outcomes of immediately (Type 1) and early placed implants (Type 2). The primary outcome was the mid-facial soft tissue level margin and the initial hypothesis upon which the study was designed was that following Type 1 implant placement significantly different mid-facial recession would be observed as compared with Type 2 implant placement.
METHODS
Fifty patients requiring tooth extraction and replacement with a dental implant were enrolled in this study.
Patients were considered for study inclusion if they were 18 years of age or older, had one tooth in either the anterior maxilla or mandible, including incisors, canines, and premolars, requiring extraction leading to a single-tooth gap to be replaced by means of an implant.
Neighbouring teeth had to be periodontally healthy with no interproximal bone loss. The walls of the extraction socket had to be intact. Patients were excluded from the study if they were currently smoking more than 10 cigarettes per day, had significant untreated periodontal disease or a history of treated periodontitis, had a medical condition or were taking medications which affected soft tissue and bony healing (e.g., history of oral/IV bisphosphonates, poorly controlled diabetes, chemotherapeutic and immunosuppressive agents).
Prior to extraction, a customized radiographic film holder was fabricated for each prospective implant site allowing the examiners to record standardized periapi-cal radiographs throughout the study using a long-cone parallel technique. Alginate impressions were made and initial study casts were obtained.
Photographs were taken perpendicularly to the facial surface. The same methodology and settings on a single camera were used throughout the study.
Following tooth extraction and confirmation of the integrity of the alveolar socket, an envelope containing the concealed treatment group allocation was opened by the surgeon to allocate the patient to immediate (Type 1) or early (Type 2) implant placement protocol following the generated random sequence.
All the surgical procedures were performed under local anaesthesia with or without parenteral sedation based on patient preference. Prior to surgery, patients were instructed to rinse for one minute with a 0.12% Chlor-hexidine rinse. Implants used were bone level titanium implants with a sand-blasted, acid etched, and chemically modified hydrophilic surface (Straumann®).
In patients randomized to the Type 1 group, the integrity of the socket walls was evaluated and if intact, the surgeon would proceed with implant placement. A limited full-thickness envelope flap (up to 5mm beyond the crest of bone) was reflected to allow for bone measurements and the implant bed was prepared according to manufacturer recommendations.
A conical healing abutment of height and diameter based on the operator's preference was then placed on the implant and the gap between the implant and the internal walls of the socket was grafted using mineralized freeze dried bone allograft (Straumann®), and covered by a resorbable collagen membrane (BioGide®). The flap was coronally advanced and sutured. Primary closure of the wound was not a requirement.
For patients allocated to the Type 2 placement protocol, a collagen plug (Ora-plug®) was placed into the extraction socket and sutures were placed over the extraction site using resorbable sutures.
Following 4-8 weeks of healing, a muco-periosteal flap was elevated which consisted of a full-thickness flap which was extended mesio-distally 1-2 teeth adjacent on each side of the implant site and a single vertical releasing incision on the distal aspect of the flap.
The implant was placed and a simultaneous guided bone regeneration procedure was performed using freeze dried bone allograft (Straumann®) to over-contour the bone on the facial aspect of the implant.
The grafted area was covered with a resorbable collagen membrane (BioGide®) and a periosteal releasing incision was performed to coronally advance the flap. A cover screw or a short conical healing abutment (<2 mm) was placed based on operator's preference with the requirement that tension-free primary flap closure would be achieved.
Immediately after implant installation and prior to any grafting procedure in both treatment groups, bone measurements were recorded using the following landmarks:
• S = Implant shoulder
• BC = Top of the bone crest
• IB = Internal border of the top of crest
• EB = External border of the top of crest
• D = Base of the defect
All patients received systemic antibiotics: amoxicillin 500 mg, three times per day for seven days. If allergic to penicillin, patients were prescribed doxy-cycline 100 mg twice per day for seven days, azithro-mycin 500 mg on the first day followed by 250 mg once per day for days two through Ave, or clindamycin 150 mg four times per day for seven days based on surgeon's preference. Choice of pain medication prescribed was based on the operator's preference.
Patients were instructed to rinse with 0.12% Chlorhexi-dine twice per day for two weeks. Patients were also prescribed 4 mg Medrol Dosepak (methylprednisolone) to limit post-operative swelling based on surgeon's preference.
All patients returned for suture removal and postoperative assessment at 7-14 days after surgery. Further follow-up visits were scheduled at one and two months post-implant placement.
Four months following implant placement, patients returned for the second stage uncovering procedure. Following an uneventful 7-14 days of healing, the patient was referred back to the primary care provider for the restorative phase. The patients were recalled after final crown delivery, three, six, and 12 months.
The aesthetic outcomes were evaluated in two ways:
(a). Soft tissue dimensions were recorded using digital photograph of the casts and the Gingival Status Software to measure the level of the mid-facial mu-cosal margin and the height of the papillae prior to extraction, three and 12 months after final crown delivery.
(b). The PES/WES as described by Belser et al. (2009) were determined by three independent examiners (ABH, GHB, BSD), two of whom were blinded as to which of the Type 1 or 2 placement protocol was used (GHB, BSD).
A calibration session consisting of the evaluation of 15 anterior implant cases unrelated to the study was performed prior to the assessment.
Clinical parameters including probing pocket depth (PPD) recorded to the nearest millimeter, modified plaque index (mPI), and modified sulcus bleeding index (mSBI) were recorded using an UNC-15 probe at four sites around the implant.
Radiographic bone level changes were evaluated using standardized radiographs made from customized plastic film holders Radiographs were taken immediately following crown delivery as well as at 12 months post-loading.
The distance of the first bone to implant contact in relation to the implant shoulder defined the bone level on the mesial and distal of the implant surface.
Patient satisfaction related to the aesthetic outcome, timing of implant placement, pain, and swelling associated with the procedure was evaluated by filling out a questionnaire at the three months after final crown delivery visit.
Answers were recorded on a visual analogue scale (VAS) ranging from 0 to 10 labelled with "completely satisfied," "no pain," "no swelling" at the zero point and "not satisfied," "extreme pain," "extreme swelling" at the ten end point. Patients were also asked whether or not the implant restoration affected their ability to speak or to eat.
RESULTS
Fifty patients were enrolled to participate in the study. Four patients were exited prior to randomization:
Two patients were withdrawn due to buccal bone dehiscence and/or fenestration observed at the time of extraction, one patient was withdrawn due to a localized infection and one patient was withdrawn due to adjacent tooth fracture after enrolment and prior to extraction.
After randomization, two patients in the immediate implant placement group (Type 1) were exited. One patient was withdrawn due to lack of primary stability and another one due to unacceptable proximity between the implant and the mental foramen.
Forty-four patients (22 in each group) received a dental implant and nine additional patients were lost to follow-up or did not receive restorations: Two patients (one Type 1, one Type 2) never pursued restorative treatment, two patients (two Type 2) did not report to the three-month follow-up, two patients (two Type 2) did not report to the six-month follow-up, two patients (two Type 2) did not report to the 12-month follow-up and one patient (Type 1) was lost due to fracture of the adjacent tooth prior to 12-month follow-up. Thirty-five patients completed the 12-month post-implant loading evaluation, including 20 Type 1 patients and 15 Type 2 patients.
The reasons for extraction included external root re-sorption, deep recurrent decay on previously restored teeth and fractures at or below the gingival margin of the tooth. Except for two teeth, all the teeth treated within the study were maxillary anterior teeth.
All the lateral incisors sites (n = 12) received a 3.3 mm diameter implant and the remaining sites a 4.1 mm diameter implant. The implants were of 10, 12 or 14mm in length.
At the one-year follow-up, all implants were well integrated resulting in a 100% implant survival for both Type 1 and Type 2 implant placement. The surgical procedure was well tolerated by the patients with the exception of two patients in the Type 2 group who experienced significant swelling and bruising following surgery, which resolved by the time of the 2-week post-operative appointment.
At the time of implant placement, significantly greater horizontal defect dimension and vertical defect depths were observed on the buccal and palatal aspect of the implants in the Type 1 group compared with the Type 2 group. Conversely, the level of the buccal bone in relation to the implant shoulder was significantly more apical in the Type 2 group where buccal dehiscences were consistently observed at the time of implant placement. Despite these initial differences at the time of implant placement, resolution of these defects was observed at the time of Stage Two surgery and no significant differences were observed for any of the osseous measurements performed between the two treatment groups.
The overall soft tissue changes were evaluated relative to each of the following parameters: mid-facial gingival margin location and the mesial and distal papillae height.
For the mid-facial gingival margin, some recession was observed from baseline to the 12-month follow-up visit and amounted to 1.03 mm ± 0.24 mm in the Type 1 group and 1.37 mm ± 0.28 mm in the Type 2 group which did not reach statistical significance (p = 0.17).
Conversely, the level of the mesial papillae receded significantly more for the Type 2 group (1.08 ±0.33 mm) at 3 months compared to the Type 1 group (0.55 ± 0.21 mm, p=0.02). At the 12-month follow-up, no significant difference was found between the two treatment groups and both papillae had receded about 1 mm.
The aesthetic outcome of the final restoration was evaluated at the 12-month follow-up visit using the PES/ WES criteria previously defined by Belser et al. (2009).
The inter-examiner agreement rate was characterized by an intraclass correlation of 0.87 and 0.85 for Type 1 and 2, respectively. None of the five individual parameters of the PES or WES, nor the total PES or WES were significantly different when comparing the outcome following Type 1 and Type 2 implant placement.
When the threshold for clinical acceptability was set at PES > 6, the percentage of clinically acceptable cases was 55% for the Type 1 group and 40% for the Type 2 group. Taking the same threshold for the WES, the percentages of clinically acceptable cases were 45% and 27% for the Type 1 and 2 group, respectively. None of these differences were statistically significant (p > 0.05).
At the 12-month follow-up examination, the recorded peri-implant clinical parameters showed mostly no significant difference between groups in all cases. These parameters reflected non-inflamed tissue with probing depths (PPDs) less than 3mm, minimal bleeding on probing and limited amounts of plaque.
Radiographic peri-implant bone levels at baseline were on average at 0.1-0.2mm from the shoulder of the implant with no significant difference between the two groups. These levels remained stable in both groups over the 12-month observation period.
Patients were overall very satisfied in both treatment groups. Both groups reported low levels of pain and swelling associated with the surgical procedure and a similar fraction in both groups reported some impairment in their ability to speak or eat following treatment (Table 7). None of the differences between groups were statistically significant.
ACRONYMS
ITI: International Team for Implantology
mPI: Modified Plaque Index
mSBI: Modified Sulcus Bleeding Index
PES/WES: Pink and White Aesthetic Scores
PPD: Probing Pocket Depth
VAS: Visual Analogue Scale
CONCLUSIONS
Previously reported results demonstrating that few differences were observed in clinical, aesthetic, and patient-centered outcomes three months after final crown delivery on implants placed according Type 1 or Type 2 implant placement protocols, were further substantiated at the one-year timeline. Additionally, stable radiographic crestal bone levels with no difference between treatment groups were documented.
Implications for practice
This study suggests that immediate and early implant placement protocols are two treatment alternatives with no significant differences in outcomes at one year following crown delivery.
Reference
1. Huynh-Ba G, Hoders AB, Meister DJ, Prihoda TJ, Mills MP, Mealey BL, Cochran DL. Esthetic, clinical, and radiographic outcomes of two surgical approaches for single implant in the esthetic area: 1-year results of a randomized controlled trial with parallel design. Clin Oral Implants Res. 2019; 30: 745-59. [ Links ]


{kind=link}