










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.74 n.2 Johannesburg Mar. 2019
http://dx.doi.org/10.17159/2519-0105/2019/v74no2a1
RESEARCH
Perceptions of stress among dentists: an investigation of stress management among dental practitioners in South Africa
S BhatI; N NyathiII
IBDS (MEDUNSA), MBA (UCT), Urgent Care Dentist, Service Rendering Department, Tygerberg Oral Health Centre (Young Author. DOB: 10/APRIL/1988). Principal researcher/author, writing article, statistical analysis, distribution of questionnaire, responsible for compliance with HREC (Human Research Ethics Committee, UCT)
IIBSc (Hons) International Agribusiness Management (The Royal Agricultural College, Cirencester, UK), MA in Organisation Studies, (University of Warwick), PhD in Management (University of Leicester, UK), Senior Lecturer, Graduate School of Business, University of Cape Town. Research supervisor, active mentorship
ABSTRACT
INTRODUCTION: Stress among dentists has been well documented in international research papers, with many reporting high levels. However, there is insufficient information on perceived stress among South African dentists
AIMS AND OBJECTIVE: The aim of this research was to investigate the level of stress among South African dentists in general, to identify high occupational stressors and the choices of stress-relieving mechanisms by the dentists.
METHOD: An anonymous online cross-sectional questionnaire was undertaken using non-probability sampling, and was distributed via social media and e-mail. The questionnaire was divided into four parts: demographic information; Work Stress Inventory for Dentists (WSID); Perceived Stress Scale (PSS); and finally, a checklist of the stress- relieving coping mechanisms commonly used
RESULTS: A significant positive correlation was found between general stress and all the work-related factors. 44%-56% of dentists identified 'being perceived as an inflictor of pain'; 'coping with difficult' and 'uncooperative patients' as major (high/great deal of stress) work stressors
RESULTS: This study found that most of the dental participants were highly stressed. Since many participants indicated patient-relations as being highly stressful it is recommended that ways be sought to improve dentist patient relationship which may help with how dentists appraise situations at work as stressful
INTRODUCTION
Many people choose the profession of dentistry because of the prestige and rewards offered in the long-term career. Dentists play an important role in society, and often the career brings excellent above-average remuneration and a chance to help others.1
Although a career in dentistry is rewarding, it can also be a highly stressful profession. A study done in the UK showed that 86% of dentists found their lives to be highly stressful.2 This is mainly because dentists are in direct contact with anxious patients, a management challenge which often requires a high level of patience.3-5
Patients who have higher dental anxiety perceive their dentists to have more negative attributes and the converse applies among patients who have lower dental anxiety.6 Dentists have to ensure that patients are calm before, during and after treatment. This often requires dentists to play two roles: that of a psychotherapist and that of a manually skilled clinician,7 Research has shown that a patient-dentist relationship has a direct impact on the physical quality of treatment.8 Thus, how dentists experience and manage anxious patients plays a pivotal role in the success of the practice.
There is a one-on-one relationship between the patient and the dentist; this places pressure on the dentist as the clinician who is faced with challenges that require making independent decisions, unlike when working in a group or teams9 and thus dentistry is considered a "lone" profession.10 Furthermore, dentists quite often have to deal with incompetent staff, intrusive insurance enquiries and the running of the practice/(business) or department.11
Stress/burnout that is experienced in one part of one's life, will more often than not have an influence in other areas too, spreading to other aspects of personal life.12 It is important for both dental students and dentists to be very aware of these stressors which are associated with the occupation, in order that they may live a more fulfilling professional life.13
It has been well documented in South Africa that there is a limited number of dental professionals, and dentistry is considered a scarce skill in South Africa. According to statistics published in May 2016 by the Health Professions Council of South Africa, only 6147 dentists were registered.14 The population of South Africa, according to the World Bank, was around 56 million in 2016.15 The low ratio of dentists to the population indicates that many people in South Africa do not have sufficient access to dental care, a situation which places considerable mental and physical pressure on dentists. These pressures may contribute to low job satisfaction, affect the way dentists run their businesses and influence the quality of relationships they have with their patients.16
There is not much in the literature about the coping strategies used by dentists. According to Alexander (2001): "In one study, 24 percent of the dentists surveyed said they did nothing, 32 percent said they used physical activity to de-stress, and 13 percent reported they just "coped." Only 10 percent said they took any time off from the practice, and only six percent had a hobby".17 Another study surveyed 700 dentists and found that interacting with people, taking part in sport and forgetting about work were the top three coping strategies used by New Zealand dentists.16 The least used coping strategies were smoking, recreational drugs and prescribed drugs.
Although perceived stress among dentists has been studied in other countries, further research on the topic is required in South Africa.18 Therefore, the aim of this study was to investigate the level of general stress among South African dentists, the various contributors to high levels of work stress, and to understand what coping mechanisms dentists practiced. This will assist dental students and dentists to become more aware of the occupational issues that they may encounter, or indeed are currently facing, and to provide information on more effective coping strategies that may help them to enjoy a fulfilling professional and personal life.
METHOD
The study was conducted in a limited research time and therefore a non-probability sampling approach (snowballing, purposeful and convenience) was used in surveying general dental practitioners living in South Africa. However, the sample was wide, consisting of general dental practitioners with various lengths of experience working in the private or public sectors, and practising in rural, small-town or urban centres within the country. All were registered with the Health Professions Council of South Africa (HPCSA).
Google forms were used to create a modified questionnaire that was distributed via e-mail, Dental Facebook pages, WhatsApp and Linkedln. All response buttons were activated for each question on the Google forms, making it mandatory for all participants to answer all questions.
The responses were confidential and the researchers did not collect identifying information such as names, email addresses or IP addresses. In addition, the questionnaire complied with the latest version of The Department of Health, Ethics in Health Research: Principles, Structures and Processes (2015). The study was approved by the Human Ethics Committee of the Faculty of Health Sciences, University of Cape Town. A total of 151 questionnaires were received.
Measures
The study was based on a deductive approach, determining the choice of the following standardised sections in the questionnaires:
1. The demographic information: The questionnaire started off with eight demographic questions (age; sex; relationship status; children; area of work- rural, small-town or urban; province; the sector of work and number of years of experience).
2. The Perceived Stressed Scale (PSS): This is composed of 10 questions that measured the overall perception of stress within the last month.19
3. Work Stress Inventory for dentists (WSID)5:
This was developed to identify specific work stressors experienced by general dental practitioners.5 The original WSID consisted of 30 items divided into five factors labelled as: 'time and scheduling pressures'; 'pay-related stressors'; 'patients' unfavourable perception of dentists'; 'staff and technical problems'; and 'problems dealing with patients'. WSID Factor 2 (pay-related stressors) was slightly modified to accommodate the South African context by eliminating two questions which were: 'working constraints set by NHS' and 'the piecework system of payment'.
The final questionnaire used for the study therefore consisted of 28 items. PSS used the ordinal Likert scale ranging from 0-4 (0: no stress to 4: very high-stress) and WSID used the Likert Scale ranging from 1 (no stress) to 5 (a great deal of stress) to measure negative or positive thoughts and feelings.
4. Stress-Coping strategy checklist: This section consisted of 12 activities, participants being given the choice to check multiple options that most describe their strategies in managing their stress.
The data (PSS, WSID, and Stress-Coping strategy checklist) were analysed by descriptive analysis which was computed via IBM SPSS 23 statistics software. The descriptive statistics include cross tabulations, frequency distributions, standard deviation and means, as well as a classification of data of frequencies for non-parametric variable analyses; correlations; t-test for two categories and ANOVA for three or more categories, with the alpha level set at 0.05. For both PSS and WSID, the higher the total score, the higher the levels of stress.
RESULTS
Demographic information
Of the 151 respondents, 54% (n= 81) were female and 46% (n=70) were male. Most participants were between 26-40 years of age, making up 58.9% (n=89) of all respondents. A higher proportion of respondents had a significant other (79%; n=119), had less than five years of work experience (33.1%; n=50), worked in private practice (67%; n=101), lived in urban areas (61%; n=92) and had children (53%; n=81). Gauteng Province is the home of three of the four dental academic institutions and is the most populated province in South Africa, so it is no surprise that the highest number of participants (35%; n=53) came from this Province.
Perceived Stress Scale (PSS)
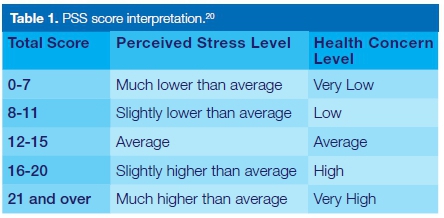
A higher stress score indicates higher stress levels, which are associated with an increased susceptibility to stress-induced illness such as depression or burnout.20Table 1 is used to interpret, analyse and discuss the PSS section of the results.
The relationship between the individual and the overall PSS score
The mean total PSS score of all 151 dentists is 19.3 (SD=7.9) with a median of 19 which indicates a high health concern and a slightly higher than average perceived stress level.
Figure 1 shows 44% of dentists scored much higher than average which was also the highest score level among the five perceived stress levels and 21% (slightly higher) than average.
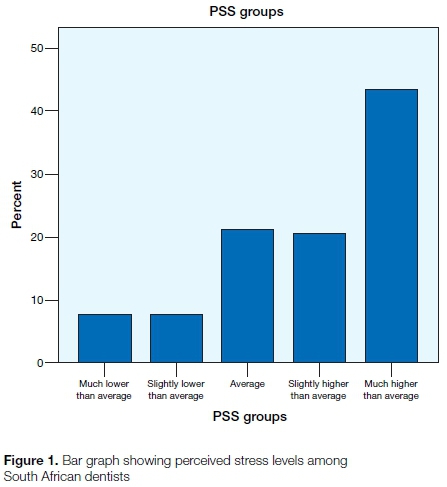
Table 2 demonstrates that most of the dentists fairly often felt that things were going their way (62; 41.1%) and felt that they were on top of things (65; 43%).
Also, one third of dentists fairly often (51; 33.8%) felt confident about their ability to handle their personal problems and almost never (49; 32.5%) felt difficulties were piling up so high that they could not overcome them. Whereas almost half of the respondents said they were sometimes (71; 47%) and fairly often (31; 20.5%) upset because of something that happened unexpectedly, and a good number of dentists very often (41; 27.2%) and sometimes (47; 31.3%) felt nervous and stressed.
The relationship between PSS scores and demographic variables
The study indicated that female dentists were found to have greater perceived stress scores (20.8) than male dentists (17.5). There was a significant difference found between male and female dentists in the total mean PSS score (p< 0.05).
The maximum mean PSS score (21) was observed in dentists who have 5-10 years of dental experience and the least mean PSS score (17) was found in those who have had more than 15 years of dental experience. Even so, the difference between the means of the four categories of years of dental experience (<5 years, 5-10 years, 10-15 years, >15 years) was found not to be significant (p>0.05).
Dentists who have children reported a lower mean PSS score (18) than dentists who didn't have children (20.6). It was observed that there was a significant difference in mean PSS scores between dentists who had children and those who didn't (p<0.05). The study also showed that male dentists are significantly more likely to have children than female dentists (Chi-square= 7.501; p<0.05).
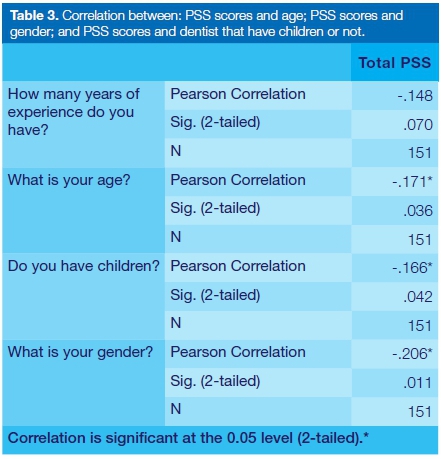
It may be deduced from the data in Table 3 that there is a negative correlation between PSS scores and: age (r=-0.171), gender (r=-0.206), dentists' parental status (r=-0.166), and experience (r=-0.148). Apart from dental experience (p>0.05), all else showed significant differences in correlation (p<0.05).
Work Stress Inventory for Dentists (WSID)
Interpretation of the scores: WSID identifies stressors that are perceived to be highly stressful among dental professionals, therefore the data for both 'high-stress and great deal of stress' have been added to identify most stressful stressors.
The researchers looked at each of the 28 items from the WSID to evaluate the percentage of work stressors which dentists reported as the most stressful ('High-stress' and a 'Great deal of stress' indicates that the participant ticked no. 4 and no. 5 respectively on the Likert Scale). Of the 28 items, the ten items which dentists stated to be the most stressful are shown in Table 4.
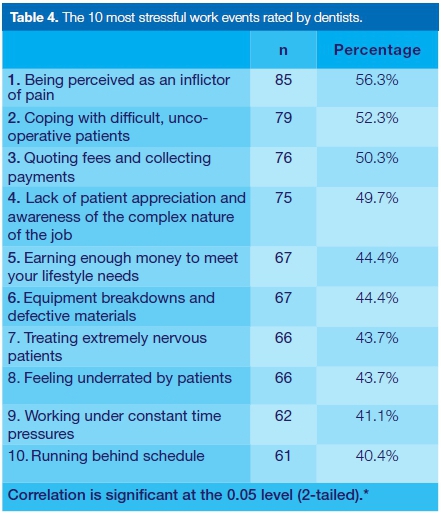
'Being perceived as an inflictor of pain' was rated as most stressful by 56.3% (n=85) of dentists, followed by 'coping with difficult, uncooperative patients' (n=79; 52.3%); 'quoting fees and collecting payments' (n=76; 50.3%); 'lack of patient appreciation and awareness of the complex nature of the job' (n=75; 49.7%); 'earning enough money to meet your lifestyle needs' (n=67; 44.4%); 'equipment breakdowns and defective materials' (n=67; 44.4%); 'treating extremely nervous patients' (n=66; 43.7%); 'feeling underrated by patients' (n=66; 43.7%); 'working under constant time pressures' (n=62; 41.1%); 'running behind schedule' (n=61; 40.4%). In addition, 'maintaining high levels of concentration for long periods and with few breaks' was also reported by 40.4% of dentists (Factor 1) as a most stressful event.
Table 5 shows the mean for each of the five dental stress factors. Of these, those related to patients' unfavourable perceptions of dentists have the highest mean work stress scores of 3.2 (SD=1.355), second to those related to problems dealing with patients (mean=3.06, SD=1.054). Staff and technical problems have the least mean work stress scores of 2.95 (SD=1.264).

The relationship between WSID scores and demographic variables.
With regards to gender, female dentists experienced a significantly (p<0.05) higher mean work stress score than did male dentists (90.59, 78.23, respectively).
We looked at 'equipment breakdowns and defective materials' (r=-0.08; P>0.05); 'treating extremely nervous patients' (r=0.04; P>0.05) and 'actually making mistakes' (r=-0.122; P>0.05) with age and experience, and found the relationships to be weak with no statistical significance.
The relationship between PSS scores and WSID scores
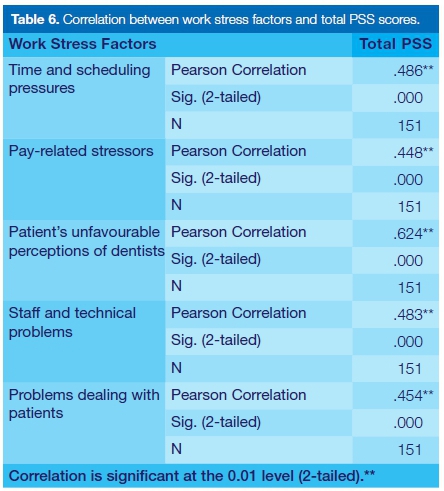
Perceived overall stress was significantly highly correlated with all the five work factors: time and scheduling pressures (r=0.49; p<0.01), pay related stressors (r=0.45; p<0.01) patient's unfavourable perceptions of dentists (r=0.62; p<0.01), staff and technical problems (r=0.48; p<0.01), and problems dealing with patients (r=45; p<0.01) (Table 6).
Coping strategies
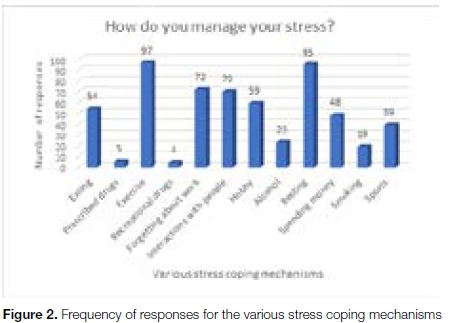
Participants were requested to tick multiple strategies that helped them to cope with their stress levels. Of the 12 coping strategies or mechanisms, exercise (n=97; 64%) and resting (n=95; 63%) were the most frequently selected by the respondents. Almost 50% of the respondents said that forgetting about work helped them cope with stress and 46% of respondents said that interactions with people assisted them in times of stress. Only 15% of respondents resorted to alcohol, 3.3% resorted to recreational drugs and 13% resorted to smoking to relieve their stress (Figure 2).
There is no significant difference found between genders for the following coping strategies: alcohol consumption, resting, interacting with people and for smoking. However, there was a significant difference found between the genders with regards to the coping mechanism of exercising (Chi-square=10.205; p<0.05), indicating that male dentists were more likely to exercise than female dentists.
Since many participants ticked 'interaction with people' as a way of reducing their stress, the authors wanted to know if the area (rural, small town or urban) in which dentists worked had an impact on whether they interacted with people or not. The study found that there was no significant difference (Chi-square=.792; p>0.05).
DISCUSSION
Perceived general stress among dentists
The results highlight the fact that dentists experienced slightly higher than average overall stress scores, indicating that dentists do experience a high perceived level of stress, with mean PSS scores also shown to be much higher than the mean PSS scores observed among US population.21 The study found that a large proportion of dentists recorded much higher than average (44%) and slightly higher than average (21%) stress scores, indicating that 65% of participants experienced high-stress levels, which meant that they had a high susceptibility to stress-induced illness such as depression or burnout.20 This finding agrees with results from Möller & Spangenberg who that found that 40% of dentists experienced extremely high-stress levels.18
When looking at the individual demographic characteristics, it was found that female dentists experienced significantly higher levels of reported stress than did male dentists. This indicated that female dentists overall perceived life situations as more stressful than male dentists. Although the study by Möller, & Spangenberg18 used a different scale to measure stress, they reported that there was no significant difference in stress levels found between the two genders.18 However, their study was done 10 years ago and 52% of the present respondents have less than 10 years of dental experience, which may indicate the presence of a trend among newer graduates. Also, Möller and Spangenberg18 included only 13% of female respondents, which may have made it more difficult to detect significant differences. Another important issue to note is that there is a larger number of female dental graduates in South Africa now than in 1996. Reports state that almost 80% of dentists graduating between 1985 and 1994 were male. This, however, changed significantly between 1995-2004, with the proportion of female dental graduates rising to 46%.22 Although random sampling was applied -offering an equal probability for any dental participant to be chosen for participation in the study - this could explain why the 1996 study had a low count of female dental practitioners.18
The lowest overall stress score was also among dentists who had had the most years of dental experience (>15 years). However, a closer look showed that there was no statistical correlation between dental experience and perceived overall or general stress. Overall perceived stress is highly likely to occur in dentists of various experience and dentists who have the most dental experience, stress less for reasons other than longevity in the profession.
The present study found a significant difference in stress experience between dentists who have children and those who don't, those with children reporting significantly less general stress than did those without children. This study also found that male dentists were significantly more likely to have children than would female dentists. One possible explanation for this comes from a study done in 1997 by De Wet, Truter and Ligthelm who found that when South African female dentists had children, they worked significantly fewer hours per week than did their male counterparts.23 It may be that male dentists were less involved with their children and relied more on their spouses. In addition, the study found that female dentists could afford to work for fewer hours because they were not the breadwinners, which may also have contributed to their lower levels of parental stress.23 However, the present study did not look at the working hours or family dynamics of each participant, opening the opportunity for new studies on stress and dental families in South Africa.
Occupational stressors for dentists
'Being an inflictor of pain' and 'coping with difficult, uncooperative patients' were also identified in much of the literature as top high stressors. 4,16,24-26 These factors, 'being an inflictor of pain' and 'coping with difficult patients', were also reflected in another study, which concluded that large numbers of the dentists found these stressors to be intensely stressful in South Africa.23 'Running behind schedule' was ranked by more than 60% of dentists as a top high stressor in many studies.8,24,26,27 However, in the present study it was ranked as the 10th highest work stressor, with 40% of respondents rating the item as causing a high-stress/great deal of stress.
Of the Ave work factors, 'staff and technical problems' caused the least amount of stress among the surveyed dentists. Also, reporting under this factor, almost 60% of dentists responded that 'interpersonal problems with work colleagues' gave them no stress/little stress. Relationships with their work colleagues were low on their list of stress causes. Similarly, this confirms a previous South African study,18 and the investigation which found office management to be the lowest cause of stress levels among Saudi Arabian dentists.28
The factors that caused the highest amounts of stress were related to an unfavourable perception of the dentist and problems dealing with patients. This agrees with Kay & Lowe's study which found that UK dentists attributed patient demand as the highest work stress factor.2 However, this is in contrast to a paper reporting on stress among Yemeni dentists which found the patient-related factor to be the lowest cause of stress.25 Another discovery was that the lowest mean score for work stress factor (staff and technical problems) found in the present study were similar to the highest mean scores for work stress factors found in both the Yemen and in Saudi Arabia.25,28 South African dentists in this study certainly perceived dentistry to be a highly stressful profession.
With regards to gender, not only were the mean general stress scores higher for female dentists than for male dentists, but also were the mean work stress scores. Female dentists perceive dentistry as being significantly more stressful than do male dentists. This corroborates findings in a UK study,24 whilst no differences in gender were found among Southern Thailand dentists.29
No significant relationship was found when observing the correlation between the number of years of dental experience and the three work stressors (equipment breakdowns, making mistakes or treating extremely nervous patients). However, this contrasts with a previous South African study.18
An important finding was that high overall perceived stress in a dentist's life were strongly associated with all five work stress factors (time and scheduling pressures, pay-related stressors, patients' unfavourable perceptions of dentists, staff and technical problems, and problems dealing with patients). Although further studies are required to determine the cause and effect, dentistry is indeed a work related stressful profession among the South African dentists who participated in this study, in concord with UK dentists.24
Coping strategies used among dentists
In contrast to other studies25,28,29 a high proportion of South African dentists, especially males, reported that they exercised (This may explain why males experienced significantly less stress than female dentists!).
More New Zealand dentists working in major cities reported interacting with people as a strategy for coping with their stress than did those working in other areas.16 The present investigation found no significant differences between these groups. Dentists are not restricted from interacting with people, wherever the venue. This study found that 15% of dentists consumed alcohol as a form of stress relief. This is much less than the report of a previous South African study18 that more than 40% of dentists drank alcohol to relieve their stress levels. This seems to indicate that the number of dentists who drink alcohol to relieve their stress has diminished. These data reflect a marked reduction in dependency on alcohol.
LIMITATIONS
Firstly, in recognition of the constraints of time, non-probability sampling (convenience or purposive) was used rather than random sampling, therefore resulting in the situation where each member of the dental population did not get an equal chance of being picked.30 Hence it will not be possible to draw inferences from the study on the general population.
Secondly, this is a cross-sectional study i.e. observing a section of the dental population at one point in time, therefore a cause-and-effect relationship cannot be determined.24 This is also one of the limitations of the PSS scale i.e. it measures stress levels within the preceding month.
CONCLUSIONS
The dentists in this study had a much higher than average overall perceived stress score and these were shown to be associated with high work stress levels. This confirms the findings of the previous South African study18 and many others5,16,18,24,28,29,32 that dentistry is a highly stressful profession.
The occupational stressors identified as highly stressful were patient related matters, indicating the need to improve dentist-patient relationships. It is therefore recommended that good patient communication skills are taught at undergraduate level and are reinforced throughout a dentist's career.
Most dentists in this study chose to manage their stress by exercising, resting, forgetting about work and interacting with people. Since many of the dentists in this study were found to be highly stressed, it is recommended that they seek healthier coping strategies and improve their dentist-patient relationship. Overall, this study indicated the stressful nature of the dental profession, therefore interventions are desirable to help dentists lessen stress in the work environment.
ACRONYMS
PSS: The Perceived Stressed Scale
WSID: Work Stress Inventory for Dentists
References
1. Garla BK. Career aspirations and reasons for choosing dentistry as a career-A survey of dental students in Gandhi Dental College and Hospital, Bhubaneswar. Ann Essences Dent. 2011;3(2):108-10. [ Links ]
2. Kay EJ, Lowe JC. A survey of stress levels , self-perceived health and health-related behaviours of UK dental practitioners in 2005. Br Dent J. 2005;204(11):E19-E19. [ Links ]
3. Newton JT, Allen CD, Coates J, Turner A, Prior J, Kent W, et al. How to reduce the stress of general dental practice : The need for research into the effectiveness of multifaceted interventions. Br Dent J. 2006;200(8):437-40. [ Links ]
4. Cooper CL, Mallinger M, Kahn R. Identifying sources of occupational stress among dentists. J Occup Psychol. 1978;51(3):227-34. [ Links ]
5. Cooper CL, Watts J, Kelly M. Occupational stress amongst general practice dentists. J Occup Psychol. 1988;61(1):163-74. [ Links ]
6. Liddell A, May B. Patients' perception of dentists' positive and negative attributes. Soc Sci Med. 1984;19(8):839-42. [ Links ]
7. Szymanska J. Occupational hazards of dentistry. Ann Agric Env Med. 1999;1(6):13-9. [ Links ]
8. Moore R, Brodsgaard I. Adult dental anxiety and related dentist beliefs in Danish private practices. Plat Surf Finnish. 1997;84(8):562-7. [ Links ]
9. Puriene A, Janulyte V, Musteikyte M, Bendinskaite R. General health of dentists . Literature review. Stomatologija. 2007;9(1):10-20. [ Links ]
10. Dhillon S, Deshpande A, Porwal P, Poonacha KS. Professional burnout in Dentistry : A review. Paedodontics 2014;6(5):28-9. [ Links ]
11. Chambers DW.The role of Dentists in Dentistry. J Dent Educ. 2001;65(12):1430-40. [ Links ]
12. Winwood PC, Winefield AH. Comparing two measures of burnout among Dentists in Australia. Int J Stress Manag. 2004;11(3):282-9. [ Links ]
13. Freeman R, Main JR, FJB. Occupational stress and dentistry: theory and practice. Part I. Recognition. Br Dent J. 1995;178(6):214-7. [ Links ]
14. Statistics [Internet]. HPCSA. 2016. Available from: http://www.hpcsa.co.za/Publications/Statistics [ Links ]
15. South Africa [Internet]. World Bank. 2016. Available from: http://data.worldbank.org/country/south-africa [ Links ]
16. Ayers KMS, Thomson WM, Newton JT, Rich AM. Job stressors of New Zealand dentists and their coping strategies. Occup Med (Chic Ill). 2008;58(4):275-81. [ Links ]
17. Alexander RE. Stress- related suicide by dentists and other health care workers:fact or folklore. J Am Dent Assoc. 2001;132(6):786-94. [ Links ]
18. Möller AT, Spangenberg JJ. Stress and coping amongst South African dentists in private practice. J Dent Assoc South Africa. 1996;51(6):347-57. [ Links ]
19. Cohen S. Perceived stress scale [Internet]. Vol. 24, Mind Garden. 1994. p. 1-2. Available from: https://www.mindgarden.com/documents/PerceivedStressScale.pdf. [ Links ]
20. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(3):385-96. [ Links ]
21. Cohen S, Janicki-Deverts D. Who's stressed ? Distributions of psychological stress in the United States in probability samples from 1983,2006, and 2009. J Appl Soc Psychol. 2012;42(6):1320-34. [ Links ]
22. McMillan W, Lalloo R, Gugushe, TS, Ligthelm AJ, Evans WG. Gender and race distribution of dental graduates (1985-2004) and first year dental students (2000-2005) in South Africa. J Dent Assoc South Africa. 2005;60(5):206-9. [ Links ]
23. De Wet E, Truter M, Ligthelm AJ. Working patterns of male and female dentists in South Africa. J Dent Assoc South Africa. 1997;52(1):15-7. [ Links ]
24. Myers HL, Myers LB. " It 's difficult being a dentist ': stress and health in the general dental practitioner. Br Dent J. 2004;197(2):89-93. [ Links ]
25. Al-Zubair NM, Al-ak'hali MS, Ghandour IA. Stress among dentists in Yemen. Saudi J Dent Res [Internet]. 2015;6(2):140-5. Available from: http://dx.doi.org/10.1016/j.sjdr.2014.09.003 [ Links ]
26. Wilson, RF, Coward PY, Capewell J, Laidler TL, Rigby AC, Shaw TJ. Perceived sources of occupational stress in general dental practitioners. Br Dent J. 1998;184(10):499-502. [ Links ]
27. Cooper CL, Watts J, Kelly M. Job satisfaction, mental health, and job stressors among general dental practitioners in the UK. Br Dent J. 1987;162(2):77. [ Links ]
28. Jamjoom HM. Stress among dentists in Jeddah , Saudi Arabia. Saudi Dent J. 2008;20(2):88-95. [ Links ]
29. Leggat PA, Yapong B. Health of dentists in Southern Thailand. Int Dent J. 2001;51(5):348-52. [ Links ]
30. Doherty M. Probability versus non-probability sampling in sample surveys. The New Zealand Statistics Review. 1994. [ Links ]
31. Mahmoud CNS, Al T, Ghada CNS, Abu M. Application of the perceived stress scale in the health care studies.An analysis of literature. Int J Acad Res. 2012;4(4):45-50. [ Links ]
32. Naidoo S. Managing stress in the dental environment. J Dent Assoc South Africa. 2015;70(9):7-8. [ Links ]
 Correspondence:
Correspondence:
Shubha Bhat
Urgent Care Dentist, Service Rendering Department, Tygerberg Oral Health Centre
Email: shubha_bhat@yahoo.com


{kind=link}