










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.73 no.10 Johannesburg Nov. 2018
http://dx.doi.org/10.17159/2519-0105/2018/v73no10a2
RESEARCH
The effectiveness of a tooth brushing programme for children in the Ehlanzeni district of Mpumalanga
M van der WaltI; PJ van WykII; JK BesterIII; PJ BeckerIV
IBChD, PG Dip Dental (Community Dentistry), Department of Health, Mpumalanga Provincial Government and Department of Community Dentistry, University of Pretoria
IIBSc, MChD, PhD, Department of Community Dentistry, University of Pretoria
IIIBChD, PG Dip Dental (Endodontics), Department of Health, Mpumalanga Provincial Government
IVMSc, PhD, Research Office, Biostatistics, Faculty of Health Sciences, University of Pretoria
SUMMARY
PURPOSE: To evaluate the effectiveness of a tooth brushing programme in a community trial in the Ehlanzeni district, Mpumalanga
METHODOLOGY: Two samples of 250 children, 8-10 years old and in grade 3, were randomly selected from schools in the district. The intervention group comprised children who had taken part in the brushing project since it was incepted in 2012. The control group comprised children who had not participated. Caries was scored according to WHO Criteria (1997) and odontogenic infections using the PUFA/ pufa index. These data and the treatment needs of the two groups were compared statistically
RESULTS: The prevalence of dental caries (primary and permanent teeth) was 57.2%, intervention group and 74.8%, control group. The intervention group recorded DMFT of 0.15 and a dmft of 1.82, whilst the control group recorded 0.38 and 2.50 respectively
Odontogenic infections occurred in 22% of the intervention group (mean 0.40), compared with 36% in the non-intervention group (mean 0.82). The intervention group presented with 30.8% less dental caries and 63.6% less odontogenic infections than the control group.
CONCLUSION: The results of the study show that this targeted population approach resulted in significantly less caries in the intervention group than in the control group
Keywords: Dental caries, prevention, tooth brushing programmes, effectiveness.
Role played by each author
M. van der Walt: Drafting of proposal and final report, overall supervisor of the planning and execution phase of the project, examiner, data analysis.
P.J. van Wyk: Assisting with the planning of the project, calibrator and trainer, assisting with data analysis and final drafting of proposal and report.
P.J. Becker: Statistical analysis.
J.K. Bester: Assisting in drafting of proposal, examiner.
INTRODUCTION AND BACKGROUND
Dental caries and gingivitis are the most common oral diseases among children with 60-90 % of children being affected globally.1 The results of the last National Children's Oral Health Survey, conducted in South Africa between 1999 and 2002, indicated that 39.7% of the 6-year-old children were caries free, which was below the goal of 50% set by the Department of Health and WHO for the year 2000.2,3
Dental caries is a progressive disease and if left untreated can negatively affect the quality of life of affected children. Pain resulting from decayed teeth, can compromise a learner's concentration and participation in school activities, hampering their development and denying them the full benefit of schooling.4
Although dental caries in South Africa reduced significantly during the last three decades as indicated in data obtained from three National Oral Health surveys, the high levels of untreated caries in all age groups is an alarming cause for concern.5,6 More than 80% of caries in children are untreated according the Unmet Treatment Need Index.3
The World Health Organisation emphasizes the importance of public health approaches for the prevention of dental caries through the effective use of fluorides, including implementation of water fluoridation.7 Fluoridated drinking water has been shown to be the most common method for systemically applied fluoride and to be effective in reducing the severity of dental decay in entire populations.8
To this day, water fluoridation has not been implemented in South Africa, with the local authorities expressing concern in the past regarding cost of implementation and effectiveness of such an intervention.9 A study conducted in 2012 concluded that water fluoridation in South Africa remains a viable option to prevent and reduce the prevalence of dental caries.9
There is a global consensus that regular use of fluoride toothpaste is critical in child dental health. Most experts are of the opinion that the dramatic decline in caries during the last decade of the 20th century is due to the use of fluoride toothpaste.10
Health promotion programmes that involved tooth brushing have been among the most successful educational programmes in caries prevention.11,12Cross-sectional surveys, clinical trials and experiments related to tooth brushing research studies involving populations of 1450-1545 children have found that tooth brushing twice a day resulted in increased tooth retention.11
South Africa is unique as its health care system needs to provide services to a wide spectrum of the population, ranging from poor, historically disadvantaged, groups to sections of the population with a high socioeconomic status.13 There is little evidence that caries in children is addressed adequately through efforts of policy and of service provision.14
Due to persistent inequalities in the access to oral health care, the public sector is under constant pressure to deliver equitable, cost effective primary oral preventive services.15 Prevention through the use of fluoride is suggested to be the most cost effective way of reducing this public health burden.16
In the absence of water fluoridation schemes in South Africa, the introduction of tooth brushing programmes with fluoridated toothpaste in schools located in low socio-economic neighbourhoods could be a realistic way of preventing the high incidence of untreated dental caries. Although several studies have indicated that caries prevalence and severity can be reduced by brushing programmes, very little is known about the effectiveness of such an intervention in the South African public school set up.
LITERATURE REVIEW
The benefits of fluoride in caries prevention have generally been accepted by researchers. The effect is achieved in at least three ways: remineralization of early damage to enamel caused by acid produced by the plaque bacteria; improving the chemical structure of enamel and therefore rendering it more resistant to acid; reducing the ability of plaque bacteria to produce acid.17
Schools are considered as important settings for health education programmes, directed at controlling the growing burden of oral diseases and promoting oral health.18
As children spend a considerable proportion of their lives in education, schools can play a significant role in promoting both general and oral health of their pupils.19 The World Health Organization strongly recommends that children's oral health should be promoted through schools.20
Several studies indicate that daily tooth brushing using fluoride toothpaste reduces tooth decay if adopted early, becoming a routine. A longitudinal study conducted in Jordan aimed at testing the efficacy of a school-based caries preventive programme, which compared the dental caries status of two groups, where the experimental group received intensive sessions of oral hygiene instruction and where daily tooth brushing using fluoridated tooth paste was supervised.
The control group received only oral hygiene instruction sessions. After four years, the caries status of the children in the experimental group was lower than that of the control group. The difference was statistically significant (P-value<0.001).21
A study on children in the London Boroughs of Kensington, Chelsea and Westminster showed that a programme of daily teacher-supervised tooth brushing with fluoride toothpaste can be effectively targeted into socially deprived communities and that a significant reduction in dental caries can thereby be achieved, especially among caries-susceptible children.
A total of 517 children with a mean age of 5.63 years participated in the study that was conducted over 21 months. All the schools in the study had catchments areas from socially deprived neighbourhoods. The study coordinator visited the schools twice a term to ensure the programme is carried out as prescribed.22 The intervention group brushed daily at school with commercially available toothpaste containing 1,450 ppm fluoride while the control group did not participate in the brushing programme.
Reduction of caries prevalence was higher in primary dentition compared with permanent dentition. Significant reduction (p<0.01) was noticed in the decayed, missing and filled components of the proximal surfaces with a non-significant effect noticed on the occlusal and smooth surfaces.22
A recent study in Thailand confirmed the positive effect from the usage of fluoride toothpaste administered by schoolteachers in a brushing programme undertaken as part of an enhanced school oral health programme, with up to 34% reduction in caries for all schools participating and up to 41% for the most cooperative schools.
The study involved 3 706 children in 15 schools over a period of two years. There was significant less plaque reported in the intervention group. Teachers continued to encourage their new pupils to brush daily even after the project finished and indicated after completion of the project that they felt more confident in providing children with oral health education.23
A two-year study conducted on 534 Scottish children (mean age 5.3) in deprived areas reported a significant reduction in caries among high caries-risk children after they had participated in a supervised tooth brushing programme with fluoridated toothpaste at schools. Twelve schools participated.
Children were also issued with toothbrushes and toothpaste for home use. Each school had one randomly selected intervention class that participated in the daily brushing and a parallel control class that did not participate. Significantly less caries developed in the first permanent molars in the intervention group compared with the control group with reductions ranging between 32% to 56%.
It is noteworthy that the mothers were trained in infection control procedures and record keeping and served as the brushing activity supervisors rather than teachers. The mothers were financially compensated for the one hour per school day during which they undertook supervision.11
The Colgate Bright Smile Bright Future tooth brushing programme was introduced in low socio-economic areas in the Ehlanzeni district of Mpumalanga for children in grades R to 3 in June 2012. This provided an ideal opportunity to evaluate the effectiveness of a tooth brushing programme in primary schools (community trial) in the South African public school setup. Children were provided with toothbrushes and toothpaste and were allowed to brush their teeth once a day, after break, during the school week, under supervision of a teacher. Due to a lack of oral health human resources the supervising oral health professional only visited the school every four to six weeks. The execution of the tooth brushing programme was therefore not entirely under the control of the oral health professional.
The objective of this study was to evaluate the effectiveness of this programme as a community trial in the Ehlanzeni district of Mpumalanga and to assess the impact on the incidence of dental caries by comparing the caries status of children who had taken part in the trial since 2012, with the caries status of a comparable group of children from the same district who had not taken part in the brushing programme in the three years prior to the survey.
MATERIALS AND METHODS
A quasi-experimental comparison group post-test-only design was used to achieve the objectives of the study.24
Two samples of 300 children each, aged 8-10 years, were randomly selected from children in grade 3. The first sample was drawn from six schools whose pupils had taken part in the brushing project since the commencement of the project in 2012.
The second sample was drawn from children in six schools, in the same district and in close proximity to the intervention schools, who had not participated in the programme. Within each of the schools (both samples), a list of all children in grade three was obtained. The children in each list were numbered consecutively and the required number of children per school was drawn randomly by using a table of random numbers.
The required number of children per school was based on the proportion of children per school who were in grade three. Consent for the examination of each child was obtained from the parent or legal guardian, and assent from the child concerned as well as consent from the Principal of the school were confirmed. The protocol as well as the relevant annexures were submitted to the Ethics Committee of the Faculty of Health Sciences of the University of Pretoria, for approval, which was granted (Protocol 342/2015).
Two dental examiners, two record clerks and a dental assistant to assist with sterilisation procedures were involved in the study. The examiners are employees of the Mpumalanga Health Department and the survey was conducted under supervision of author MvdW.
Data were collected using the DMFT/dmft (permanent and primary dentition) index according to the WHO guidelines.25 Data for odontogenic infections was collected by making use of the PUFA/pufa index and was used according to the standard procedure.26 PUFA/pufa is an index used to assess the presence of oral conditions and infections resulting from untreated caries in the primary (pufa) and permanent (PUFA) dentition.
Various WHO forms were combined into a single form for the collection of the demographic, dental caries and PUFA/ pufa data. The examiners were trained and calibrated prior to the survey and only those who achieved the reliability of a Kappa value of 0.6 and higher were allowed to take part in the survey.
During the survey 10% of the sample was re-examined to test for intra- and inter examiner reliability.
The data were captured using Excel. During data analysis the results of the study groups (intervention and control) were compared and the level of significance was set at 0.05.
RESULTS
Sample realization and sample description
After capturing the data, the composition of the samples of the intervention and the control groups were compared and it was observed that there was an over representation of eight-year-old children in the intervention group and an over representation of nine-year-old children in the control group.
To address this issue, both samples were reduced to 250. This was done by systematically removing every third eight-year-old in the intervention group and every third nine-year-old from the control group. In order to regain the proportional distribution per school, the sample was weighted using school size divided by sample from school.
The age and gender distribution of the final realized samples of the intervention and control groups were compared and no statistically significant differences were observed. The 12 schools that participated in the study were all located in low socio-economic areas. According to the school quintile system, schools are annually classified according to poverty levels of the specific geographical area into one of Ave quintiles. Quintile 1, 2 and 3 schools are classified as no fees schools which children may attend without payment.27 All the schools that participated in this study were quintile 2 or 3 schools and were therefore comparable in terms of socio-economic factors.
Reliability of the data
As indicated in the study methodology, 10% of the sample were re-examined to test for inter- and intra-examiner reliability, using Kappa statistics. Values for inter- and intra-examiner reliability were 0.76 and 0.96 respectively.
Effectiveness of tooth brushing
The prevalence of caries in the two groups
The prevalence of dental caries (primary and permanent teeth) in the intervention group was 57.2% and in the control group, 74.8%. The difference between the two groups was statistically significant (p<0.05). The results of the study show that the intervention group presented with 30.8% less dental caries than the control group.
The severity of caries in the two groups
The severity of dental caries, expressed as the DMFT and the dmft, of the two groups is shown in Table 1.
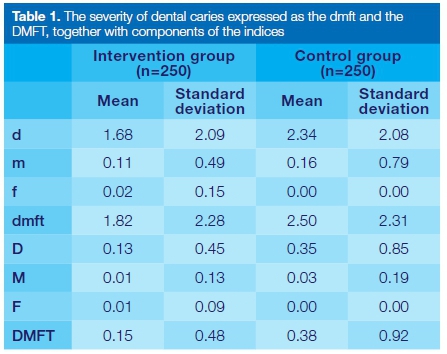
The mean DMFT's (permanent teeth) of 0.15 and 0.38 obtained in the intervention and control groups respectively were low compared with the matching dmft's (primary teeth) of 1.82 and 2.50. The mean DMFT and dmft of the intervention group were significantly lower than those of the control group. P-values of <0.05 were recorded for both comparisons.
The mean number for missing teeth due to caries was higher in the control group (m = 0.16, M = 0.03) than in the intervention group (m = 0.11, M = 0.01) for both primary and permanent teeth (Table 1). The mean number of filled teeth was negligible for all the age groups with no restorations recorded in the primary or permanent teeth of the control group (Table 1).
The Unmet Treatment Need Index (UTN) is expressed as a percentage calculated by dividing the D(d) component by the DMFT (dmft) value.
The UTN ranged from 86.7% for permanent teeth in the intervention group to 93.6% for primary teeth in the control group. For all children in the study more than 85% of all caries went untreated.
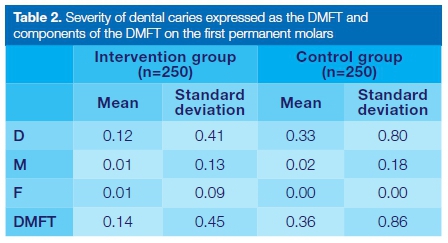
The severity of dental caries expressed as the DMFT and components of the DMFT on the first permanent molars are shown in Table 2.
If the mean DMFT of dental caries on the first permanent molars of the intervention (0.14) and the control groups (0.36) (Table 2) are expressed as a percentage of the mean DMFT of the intervention group (0.15) and control group (0.38) (Table 1), the results show that caries on the first permanent molars constitute more than 93% of all caries present in the permanent teeth of children in this age group.
Of the caries on the permanent molars, 64% occurs on the mandibular first permanent molars. First permanent molars can therefore be regarded as very vulnerable teeth at this stage and although tooth brushing may provide valuable protection, additional measures are necessary.
The prevalence and severity of odontogenic infections in the two groups
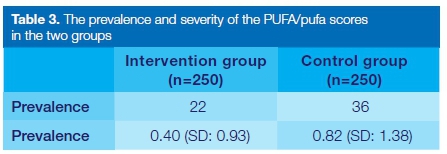
PUFA/pufa is used to assess the presence of oral conditions and infections resulting from untreated caries in the primary (pufa) and permanent (PUFA) dentition. The PUFA score for the permanent dentition was very low and PUFA and pufa were therefore combined into one score, PUFA/pufa. The prevalence and severity of the PUFA/pufa scores is shown in Table 3.
Odontogenic infections as reflected in the PUFA/pufa index were lower in children of the intervention group, twenty-two per cent of whom presented with odontogenic infections (mean 0.40) compared with 36% of children in the control group (mean 0.82).
When comparing the differences in the PUFA/pufa-scores between the intervention group and control group, the independent sample t-test yielded a P-value of 0.00, which is highly significant.
Treatment needs
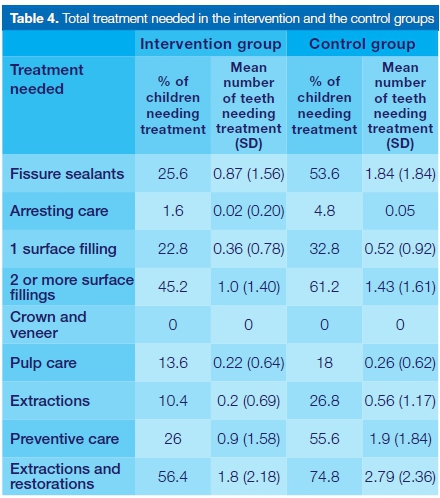
The treatment needed for children in the intervention group and control groups are indicated in Table 4.
The proportions of children in need of two or more surface restorations were noticeably high in both the intervention (45.2%, mean 1.0) and control groups (61.2%, mean 1.43). In relative terms, the number of children in need of one surface restorations were low in both the intervention (22.8%, mean 0.36) and control groups (32.8%, mean 0.52). Two or more surface Allings therefore constitute 66.5% and 58.8% of the restorative treatment needed in the intervention and the control groups respectively. Treatment needs as specified in Table 4 were higher in all categories of children in the control group compared with children in the intervention group.
The need for extractions (26.8%, mean 0.56) in the control group was higher than the need for pulp care (18%, mean 0.26), while in the intervention group, pulp care (13.6%, mean 0.22) was needed more than extractions (10.4%, mean 0.2). The need for Assure sealants in the control group (53.6%, mean 1.84) was considerably higher than in the intervention group (25.6%, mean 0.87). Overall the combined need for extractions and restorations was still higher than the need for preventative care in both groups.
Treatment needed in the permanent dentition of the total group of children (intervention and control group combined)
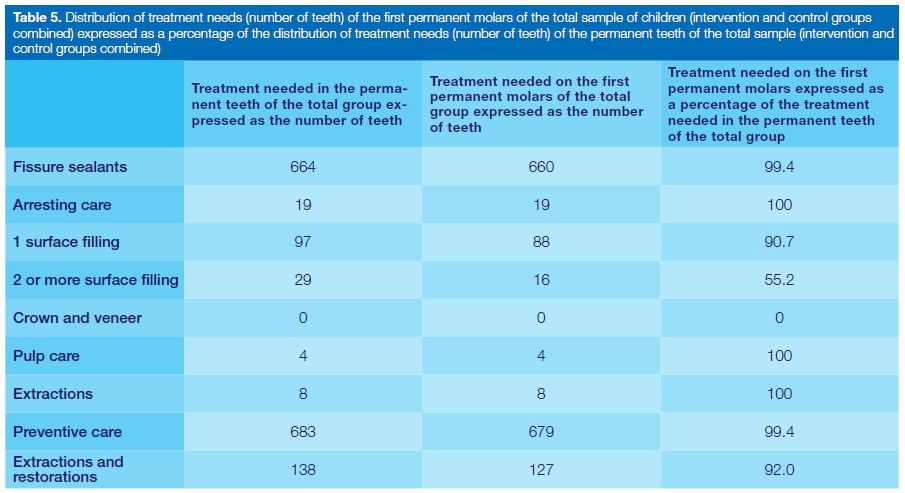
The distribution of treatment needs (number of teeth) on the first permanent molars of the total group of children (intervention and control groups combined) expressed as a percentage of the distribution of treatment needs (number of teeth) in the permanent teeth of the total group (intervention and control group combined) is shown in Table 5.
The results presented in Table 5 show that although the four first permanent molars constitute only 33.3% of the permanent teeth present in the mouth in this age group (four mandibular incisors, four maxillary incisors and four first permanent molars) they require more than 92% of the curative treatment and more than 99% of the preventive services needed on permanent teeth.
In contrast to the total treatment need (Table 4) where two or more surface fillings constitute 66.5% and 58.8% of the restorative treatment needed in the intervention and the control groups respectively, the results of Table 5 show that one surface fillings constitute 76.9% of the restorative care needed for the permanent teeth.
In addition to the large percentage of one surface fillings needed in the permanent dentition, 660 first permanent molars (33% of the total number of first permanent molars) were also identified as teeth needing fissure sealants.
DISCUSSION
Oral health habits, attitudes, and behaviour are best established during childhood. The Colgate Bright Smile Bright Future tooth brushing programme was introduced in low socio-economic areas in the Ehlanzeni district of Mpumalanga for children in grades R to 3, in June 2012. This programme provided an ideal opportunity to evaluate the effectiveness of a supervised tooth brushing programme in primary schools (community trial) in a rural area in the South African public school set-up.
Several studies indicate that daily tooth brushing using fluoride toothpaste reduces tooth decay if the practice is commenced early and becomes a routine.11,21-,23 All the analyses (Tables 1-4) demonstrated the effectiveness of the of the intervention programme. Children who brushed once daily at school during the school term, had significantly less caries and odontogenic infections than
children in the control group for whom there was no such intervention. Treatment needs in the intervention group was also lower than treatment needs in the control group (Table 4). Ideally, tooth brushing should begin at home, under parental supervision, with the eruption of the first tooth. However, children from socially deprived backgrounds are more likely to commence tooth brushing later in life and to brush less frequently than children from more affluent backgrounds.22
An alarmingly large amount of caries goes untreated as indicated by the Unmet Treatment Need Index (UTN). The UTN percentages for primary and permanent teeth of both groups ranged from 86.7% in permanent teeth of the intervention group and from 93.6% in primary teeth of the control group. This high percentage of untreated dental caries is consistent with other studies conducted in South Africa.3,6,28 This might be due to the inadequacy of resources including dental facilities and oral health professionals and/or the lack of awareness about oral health and available dental services amongst the majority of the population.3
In contrast to the total treatment need (Table 4) where two or more surface Allings constituted 66.5% and 58.8% of the restorative treatment needed in the intervention and the control groups respectively, the data of Table 5 show that one surface Allings constituted 76.9% of the restorative care needed for the permanent teeth.
This observation, combined with the finding that 33% of the total number of first permanent molars present also need fissure sealants, indicates that the placement of fissure sealants should be part of any caries preventive programme.
A significant finding of the study was that the need for extractions (26.8%, mean 0.56) in the control group was higher than the need for pulp care (18%, mean 0.26) while in the intervention group the need for pulp care (13.6%, mean 0.22) was more than that for extractions (10.4%, mean 0.2). This could possibly indicate that teeth in the intervention group were not that extensively decayed and could still be restored by performing some form of endodontic treatment.
Due to persistent oral health inequalities in access to care, the South African public health sector is under pressure to deliver effective primary oral health preventive services. Oral health promotion programmes are not implemented and distributed uniformly and appear to be fragmented with lack of evaluation. Facilities conducting primary oral health care are focusing mainly on emergency relief of pain and sepsis.29,30 This was confirmed in this study when analyzing statistics of the extremely low number of children receiving dental treatment. This indicates that by far the majority of dental carious lesions are untreated and that extractions were the treatment of choice if provided.
Studies indicated that the treatment of dental caries is expensive for governments31,32 and that the approach to eradicate disease still remains largely curative and delivered at an individual level. Oral health care service delivery is depending on expensive and sophisticated technology resulting in many South Africans being denied access to oral health services.
As discussed previously the lack of oral health personnel and dental facilities and limited knowledge of available dental services amongst the general population are contributing factors to the situation that many South Africans are denied access to care.6 Researchers found that an unrealistic high number of personnel and a substantial amount of time to perform treatment is required, if the current backlog of dental caries for children under the age of 15 is to be addressed.
Such a programme will be financially astronomical and is clearly unaffordable.6 Preventing dental diseases will be financially more beneficial. This study confirmed the suggestions of other researchers that caries in South African children is not adequately addressed through current policies and service provision.14
The brushing programme for this project was implemented and monitored by dentists due to a lack of other oral health professionals employed at primary health care facilities such as Community Health Centres in Mpumalanga, together with a severe shortage of oral hygienists and dental therapists in the Province. This type of intervention ideally should be introduced and monitored by district based oral hygienists and also funded at district level.
The National Human Resource Audit recognized oral hygienists and dental therapists as important members of the oral health team. They advised an urgent need for additional training of oral hygienists and dental therapists.33
The White Paper for Transformation of the Health System in South Africa also suggested that oral health services should be transformed through the primary health care approach. It advised focusing on equitable preventive services integrated with primary care services. It also suggested a minimum package of services which could be delivered by oral hygienists and dental therapists.34
As the oral health professional cannot be at the school full time, the importance of school principals and teachers should not be underestimated in ensuring that a preventive programme be successful. Great care should especially be taken in selecting the correct teacher to be the oral health school coordinator as he/she will play a pivotal role in the execution of the programme at ground level. Oral health school coordinators should be a responsible and motivated individual who is respected by other teachers and has the well-being of learners at heart. Such a person should be identified after consultation with the school principal who can advise the correct candidate, who in most cases for this study, was the head of the foundation phase.
The researchers observed that constant motivation of all parties involved (principals, coordinators, teachers and children) is crucial for the programme to succeed over an extended period of time.
Random checks by requesting classes to demonstrate how they conduct the brushing activities were found to be very effective as teachers do not want to be exposed as uncooperative. In general, learners found the daily brushing a fun event in which to participate and did not need as much motivation as did the teachers.
Modern dentistry had become very isolated from other elements of the health service.35 Many oral health programmes are developed and implemented in isolation from other oral health programmes, leading to duplication of efforts. Oral health programmes tend to concentrate on individual behaviour change and largely ignore the influence of socio-political factors as key determinants of health.36
A holistic approach should be considered to improve oral health of school children by developing healthy lifestyles and creating healthy environments. To achieve sustainable lifestyles oral health education should involve the active participation of children, parents and "significant others" such as school teachers.37 Policies at national level should be encouraged to provide a framework for environmental change as is the case with water fluoridation.38
CONCLUSIONS AND RECOMMENDATIONS
This study showed that teacher supervised tooth brushing programmes implemented and closely monitored by oral health professionals may be effective in the South African public school set-up, if combined with oral health education in socially deprived communities.
This targeted population approach resulted in significantly reduced caries in the intervention group compared with the control group. A substantial reduction in dental treatment needs in children could be achieved if the findings in this study could be translated to the population at risk in South Africa.
This study provide additional evidence, as previously observed by other researchers, that caries as a disease in South African children is not adequately addressed through current policies and service provision.14 It is suggested that policies and strategies should focus on reducing the burden of oral diseases through prevention and need to be integrated with other health programmes to be successful.1
As the White Paper for Transformation of the Health System in South Africa suggested, oral health services should be transformed through a primary health care approach with equitable preventive services integrated with the primary health care services.34
With dental inequality, and access to care still a huge obstacle, the focus should move away from relief of pain and sepsis and limited curative services to the provision of preventative services through an integrated primary oral health care approach, together with improving the living standards of the population with an emphasis on the most disadvantaged groups.
ACRONYMS
PUFA/pufa: P/p: Visible Pulp Involvement
U/u: Ulceration Caused by Dislocated Tooth Fragments
F/f: Fistula
A/a: Abscess
PUFA: Permanent Teeth
pufa: Primary Teeth
UTN: Unmet Treatment Need Index
REFERENCES
1. Petersen PE. The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century - the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. 2003; 31 (S1): 3-24. [ Links ]
2. Peterson PE. Challenges to improvement of oral health in the 21st century - the approach of the WHO Global Oral Health Programme. Int Dent J. 2004; 54(6): 329-43. [ Links ]
3. Van Wyk PJ, van Wyk C. Oral health in South Africa. Int Dent J. 2004; 54(6): 373-77. [ Links ]
4. Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye, C. The global burden of oral diseases and risks to oral health. Geneva: World Health Organisation; 2005. [ Links ]
5. Van Wyk PJ, van Wyk C. Trends in dental caries prevalence, severity and unmet treatment need levels in South Africa between 1983 and 2002. SADJ. 2010; 65(7): 310, 312-4. [ Links ]
6. Van Wyk PJ, Louw AJ, du Plessis JB. Caries status and treatment needs in South Africa: report of the 1999-2002 National Children's Oral Health Survey. SADJ. 2004; 59(6): 238, 240-2. [ Links ]
7. World Health Organization Expert Committee on Oral Health Status and Fluoride Use. Fluorides and oral health. WHO Technical Report Series No. 846. Geneva: World Health Organization; 1994. [ Links ]
8. Centres of Disease Control and Prevention. Populations receiving optimally fluoridated public drinking water: United States, 1992-2006. MMWR Morb Mortal Wkly Rep. 2008; 57(27): 737-41. [ Links ]
9. Kroon J, Van Wyk PJ. A retrospective view on the viability of water fluoridation in South Africa to prevent dental caries. Community Dent Oral Epidemiol. 2012; 40: 441-50. [ Links ]
10. Bratthall D, Hansel-Petersson G, Sundberg H. Reasons for the caries decline: What do the experts believe? Eur J Oral Sci. 1996; 104: 416-22. Discussion 23-5,30-2. [ Links ]
11. Curnow MM, Pine CM, Burnside G, Nicholson JA, Chesters RK, Huntington E. A randomised controlled trial of the efficacy of supervised toothbrushing in high-caries-risk children. Caries Res. 2002; 36: 294-300. [ Links ]
12. de Almeida CM, Petersen PE, Andre SJ, Toscano A. Changing oral health status of 6- and 12-year-old schoolchildren in Portugal. Community Dent Health. 2003; 20: 211-6. [ Links ]
13. Van Rensburg HCH. Profile of health and disease in South Africa. Academia 1982; 1-22. [ Links ]
14. Singh S. Dental caries rates in South Africa: implications for oral health planning. South Afr J Epidemiol Infect. 2011; 26(4): 259-61. [ Links ]
15. Singh S, Myburgh NG, Lalloo R. Policy analysis of oral health promotion in South Africa. Glob Health Promot. 2010: 17(1); 16-24. [ Links ]
16. Peterson PE, Phantumvanit P. Perspectives in the effective use of fluoride in Asia. J Dent Res. 2012; 91(2): 119-21. [ Links ]
17. Featherstone JD. The science and practice of caries prevention. J Am Dent Assoc. 200; 131:887-99. [ Links ]
18. Yazdani R, Vehkalahti MM, Nouri M, Murtomaa H. School-based education to improve oral cleanliness and gingival health in adolescents in Tehran, Iran. Int J Paediatr Dent. 2009; 19(4): 274-81. [ Links ]
19. Gill P, Chestnutt IG, Channing D. (2009). Opportunities and challenges to promoting oral health in primary schools. Community Dent Health. 2009; 26(3): 188-92. [ Links ]
20. World Health Organisation. Oral Health through Schools. Geneva: WHO document 11, 2003. [ Links ]
21. Al-Jundi SH, Hammad M, Alwaeli H. The efficacy of a school-based caries preventive programme: a 4-year study. Int J Dent Hyg. 2006; 4(1): 30-4. [ Links ]
22. Jackson RJ, Newman HN, Smart GJ, Stokes E, Hogan JI, Brown C, Seres J. The effects of a supervised tooth brushing programme on the caries increment of primary school children, initially aged 5-6 years. Caries Res. 2005; 39(2): 108-15. [ Links ]
23. Peterson PE, Hunsrisakhun J, Thearmontree S, Pitchpornchaiyakul S, Hintao J, Jurgensen N, Ellwood RP. School-based intervention for improving the oral health of children in southern Thailand. Community Dent Health. 2014; 26 (31): 1-7. [ Links ]
24. De Vos AS, Delport CSL, Fouche CB, Strydom H. Research at grass roots: a primer for the social science and human professions. Pretoria: Van Schaik Publishers; 2011. [ Links ]
25. World Health Organisation. Oral Health Surveys, Basic Methods. 4th ed. Geneva: World Health Organisation; 1997. p.39. [ Links ]
26. Monse B, Heinrich-Weltzien R, Benzian H, Holmgren C, van Palenstein Helderman W. PUFA - An index of clinical consequences of untreated dental caries. Community Dent Oral Epidemiol. 2010; 38: 77-82. [ Links ]
27. Department of Education. National Norms and Standards for school funding. 1998. Pretoria. Government Printer. [ Links ]
28. Department of Health. National Oral Health Survey: South Africa 1988/89. Pretoria: Government Printer; 1994. [ Links ]
29. Lalloo R, Solanki GS. An evaluation of a school-based comprehensive oral health programme. Community Dent Health 1994; 11(3): 152-5. [ Links ]
30. Locker D. Deprivation and oral health: a review. Community Dent Oral Epidemiol. 2000; 28:161-9. [ Links ]
31. Sheiham A. Dietary effects on dental diseases, Public Health Nutr. 2001; 4: 569-91. [ Links ]
32. Moyniham P, Petersen PE. Diet, nutrition and the prevention of dental diseases. Public Health Nutr 2004; 7(1A): 201-6. [ Links ]
33. Directorate of Human Resources Development. The Human Resource Audit for Health Care Personnel in South Africa. Department of Health, Pretoria, 1996. [ Links ]
34. Department of Health. White Paper for the Transformation of the Health System in South Africa. Government Gazette Vol 382 No 17910, Notice 667 of 1997, Pretoria 16 April 1997. [ Links ]
35. Daly B, Watt RG, Batchelor P, Treasure ET. Determinants of Oral Health. In: Daly B, Watt RG, Batchelor P, Treasure ET, editors. Essential Dental Public Health. Oxford: Oxford University Press; 2002. p. 28-30. [ Links ]
36. Sheiham A, Watt R. The common risk factor approach: a rotational basis for promoting oral health. Community Dent Oral Epidemiol. 2000; 28(6): 399-406. [ Links ]
37. Peterson PE, Hadi R, Al-Zaabi FS, Hussein JM, Behbehani JM, Skougaard MR, Vigild M. Dental knowledge, attitudes and behavior among Kuwait mothers and school teachers. J Pedod. 1990; 14(3): 158-64. [ Links ]
38. Marthaler TM, O'Mullane DM, Vrbic V. The prevalence of dental caries in Europe,1990-1995. Caries Res. 1996; 30: 237-55. [ Links ]
 Correspondence:
Correspondence:
P.J. van Wyk
Department of Community Dentistry, University of Pretoria.
P.O. Box 70068, Die Wilgers 0041.
Email: flipsibyl@gmail.com


{kind=link}