










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.73 n.10 Johannesburg Nov. 2018
http://dx.doi.org/10.17159/2519-0105/2018/v73no10a1
RESEARCH
The orthopantomograph as an indicator of vertical jaw relations
MF SulimanI; SM DawjeeII
IBChD Dip Odont (Ortho) MSc Dent (Ortho), Coordinator of the Undergraduate programme. Department of Orthodontics. University of Pretoria
IIBChD, BChD Hons, MSc Odont, M Dent (Ortho), PGD Dip IRE, PhD, Head, Department of Orthodontics. University of Pretoria
SUMMARY
INTRODUCTION: Lateral cephalometry is important in the orthodontic diagnosis of jaw relationships, in treatment planning, and prediction of growth but also in the evaluation of different facial forms. Little research has evaluated the orthopanto-mograph for these purposes
AIM: To compare the data taken from orthopantomographs and lateral cephalograms in the investigation of vertical jaw relationships and to assess correlation between measurements
MATERIALS AND METHODS: The gonial angle, ramus height and condyle angle were measured for each patient on the two radiographs and these data compared for the three different facial growth types, dolichofacial, mesofacial and brachyfacial.
RESULTS: In subjects with normal (meso-) or horizontal (brachy-) growth patterns, there were no significant differences between the mean and median values for the gonial and condyle angles, but the ramus heights showed significant differences
The data of the vertical (dolicho-) growth pattern patients recorded significant differences only between the data for the gonial angles and the ramus heights.
Significant correlations were found between the gonial angles and the condyle angles for all three growth patterns, but not for ramus heights.
CONCLUSION: in comparing the data from the two radiographs, the angular measurements showed high correlation and predictability whilst linear measurements showed inconsistency
Keywords: Orthopantomograph, lateral cephalogram, facial growth.
INTRODUCTION
The diagnosis of the vertical facial dimension is a complex problem. It may be simplified by studying a face and applying common sense diagnostic tools to ascertain whether the lower face is relatively long or relatively short.
Vertical Facial Dysplasias are to some extent the result of growth that was programmed in that direction, but their expression is influenced by the interactions of both form and function. The clinician must make a careful differential diagnosis for each patient who seeks his or her care. The diagnosis must analyze all three morphological components of malocclusion namely, facial, dental and skeletal.
Orthodontic treatment encompasses more than the correction of the dental malocclusion; but also includes the diagnosis and treatment of facial and skeletal problems, upper airway obstruction, temporomandibular dysfunction, and abnormal myofunctional habits. Each aspect must be carefully studied and understood to enable the correct diagnostic decisions to be made so as to effect a successful treatment plan. Faces are specific to the individual. Orthodontists have the ability to perceive exceedingly subtle differences in the shape, size, and proportions of both the hard and soft tissue components and also minute variations in the topographic contours amongst them. Three vertical forms exist for the shape of the face:
• the vertical, hyperdivergent - long and narrow, dolichofacial form
• the horizontal, hypodivergent - wide and short, brachyfacial form
• the normal - which is the mesofacial form
These facial patterns are also described as Leptoprosopic (thin), Mesoprosopic and Euryprosopic (broad).1 Each has characteristic, and varied, vertical facial relationships. Clinicians have long been interested in the multitude of differences in the diagnosis, treatment, and the treatment responses between these hyperdivergent or dolichofacial types and hypodivergent or brachyfacial types.2
Radiographs are important diagnostic tools in the assessment of these different facial types. Lateral cephalome-try serves as the gold standard in orthodontic diagnosis of the vertical jaw relationships, treatment planning, prediction of growth and the evaluation of facial forms.
However, cephalometric analysis has limitations, the major sources of error include image magnification, superimposition of the images of structures and errors in landmark identification, tracing and measuring.
Although the orthopantomograph is not itself free of possible errors, it is feasible that using that radiograph for the assessment of particular cranial features may effect some compensation for the limitations of lateral cephalograms.
AIM
This study aims to compare measurements taken from the orthopantomograph with those recorded from the lateral cephalogram for the investigation of the vertical jaw relationship patterns of individuals, and to assess the degree of correlation between these data.
MATERIAL AND METHODS
The sample comprised 90 patients, all adults over the age of 20 years. The sample size was determined on the Central Limit Thereom.3 There was no race or gender distinction. Patients who had received orthodontic treatment were excluded. Every patient had had a lateral cephalometric film and a panoramic film taken for routine examination. The identity of the subject was not revealed and patient anonymity was fully respected. The records were randomly numbered and documented.
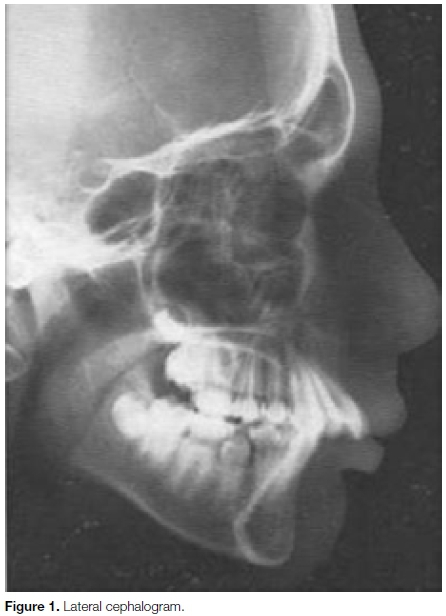
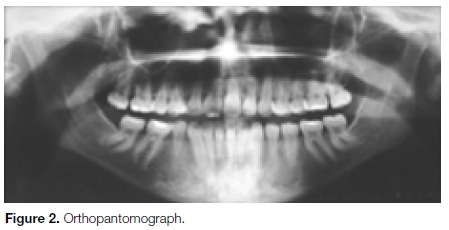
Printed pictures, having a ratio of 1:1, of the lateral cephalograms and the orthopantomographs were used for the measurements (Figures 1 and 2).
Three groups of 30 patients each represented the different growth patterns, namely dolichofacial, mesofacial and brachyfacial. The cephalogram was used as the gold standard for identification of the three categories. The cephalometric criteria on which the growth patterns were determined were:
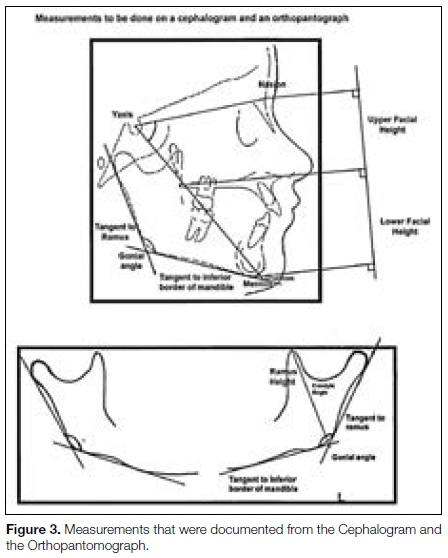
• Upper anterior facial heights were measured as the distance in mm from the nasion to the anterior nasal spine and lower facial heights were measured as the distance in mm from the anterior nasal spine to the menton on the cephalogram. The ratio was determined as that between the upper and lower measurements (mean 45% to 55%).4
• The Y-Axis was drawn from the midpoint of the sella to the gnathion point and the contained angle between the axis and the line SN was measured on the cephalogram (mean 59,4, SD 3,82).4
Measurements
Measurements of the gonial angle, condyle angle and ramus height were made on both the lateral cephalograms and orthopantomographs of these patients (Figure 3) and these data were documented and statistically compared.
Standardization was done on every fifth tracing and every third measurement was repeated by an independent investigator to ensure accuracy.
RESULTS
The data were analyzed using the SAS program, Release 92, running under Microsoft Windows for a personal computer. A total of 90 orthopantomographs and 90 cephalometric radiographs were obtained, 30 for each of the three different growth types. Mean values were compared by the two-sample t test. Median values were compared by the non-parametric Wilcoxon rank sum test. P values < 0.05 were considered significant.
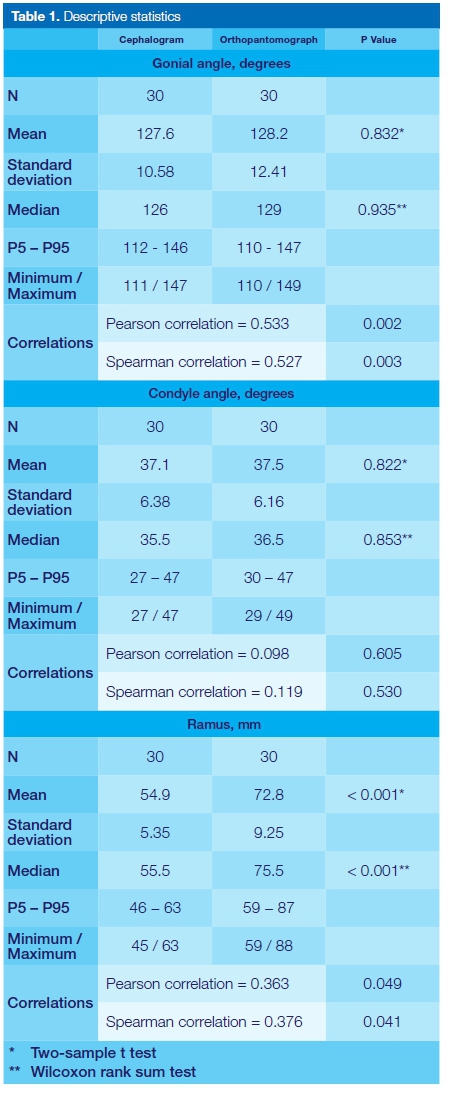
Comparisons were made of the means, standard deviations and the median values of the gonial angle, the ramus height and the condyle angle, measured in the three different growth types, namely mesofacial, brachyfacial and dolichofacial. The measurements of the cephalogram were identified as "C" and those of the orthopantomograph as "O".
Data from the three facial types were subjected to the statistical tests and the elements and findings are presented in Tables and Graphs below. P5 = percentile 5 of the distribution of values for the variable concerned, and...
P95 = percentile 95 of the distribution of values for the variable concerned.
Therefore 90% of the values occurred in the interval P5 - P95.
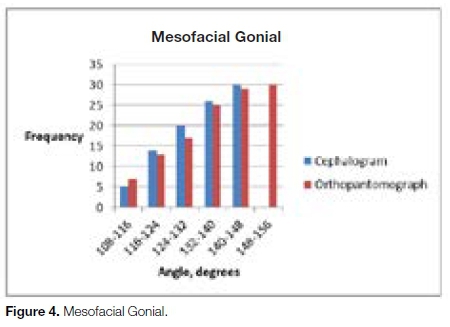
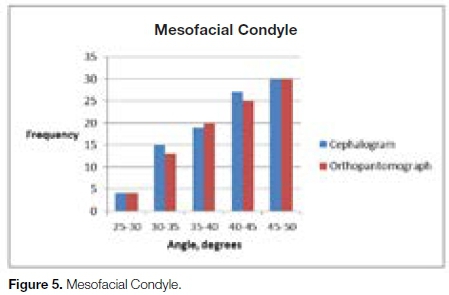
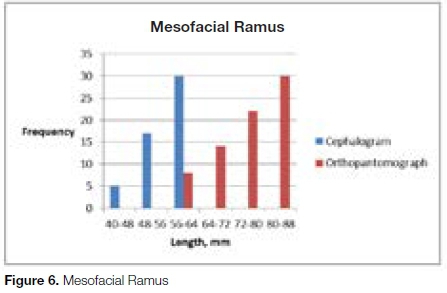
Mesofacial growth pattern
Mesofacial growth
• The mean as well as the median values of the gonial angles from the lateral cephalograms and orthopantomographs do not differ significantly.
• The mean as well as the median values of the condyle angles from the lateral cephalogram and orthopantomograph do not differ significantly.
• The mean as well as the median values of the ramus height from the lateral cephalogram and orthopantomograph differ significantly
• The P5 - P95 intervals vary noticeably for C Ramus and O Ramus, in contrast to the overlap between the lateral cephalogram and orthopantomograph bars for the gonial and condyle angles. This indicates a significant and positive correlation for the measurements of the condyle and gonial angles between the two radiographs. However, there is no correlation between the data from two radiographs in respect of the ramus height. The strong correlation is for angular measurements, while linear measurements do not show a correlation.
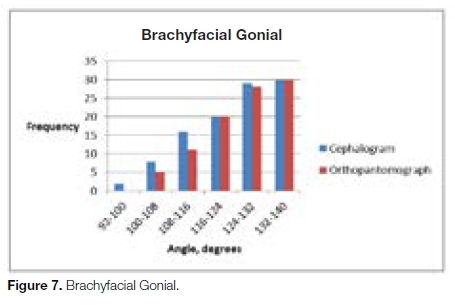
Brachyfacial growth pattern
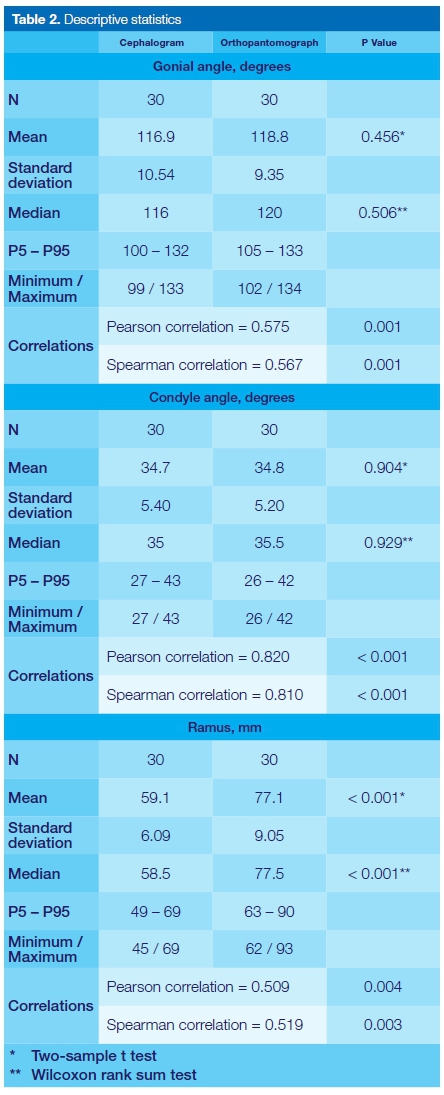
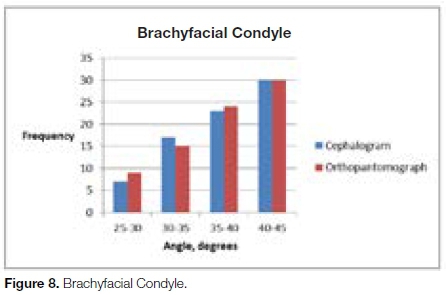
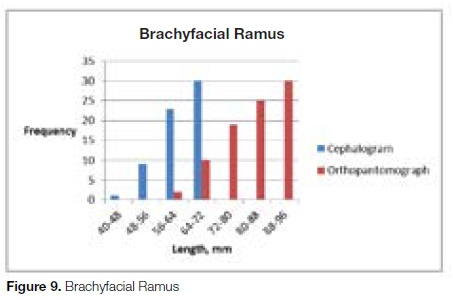
Brachyfacial growth
• The mean as well as the median values of the gonial angles from the lateral cephalogram and orthopantomograph do not differ significantly.
• The mean as well as the median values of the condyle angles from the lateral cephalogram and orthopantomograph do not differ significantly
• The mean as well as the median values of the ramus heights from the lateral cephalogram and orthopantomograph differ significantly.
• The P5 - P95 intervals do not match closely for C Ramus and O Ramus, in contrast to the overlap between the lateral cephalogram and orthopantomograph bars for the gonial and condyle angles. Thus, significant and positive correlations between the data from the two radiographs were found for the gonial angles and the condyle angles. With regards the ramus measurements, no correlation was found.
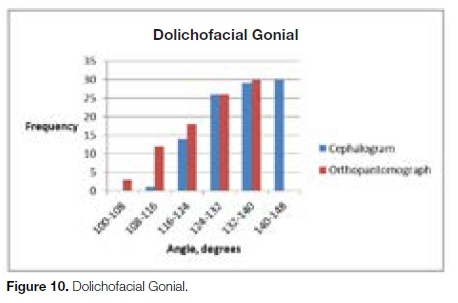
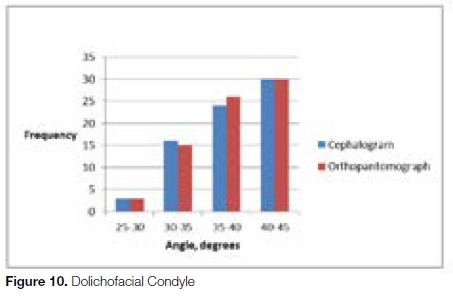
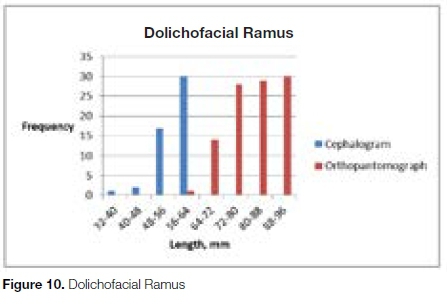
Dolichofacial growth pattern
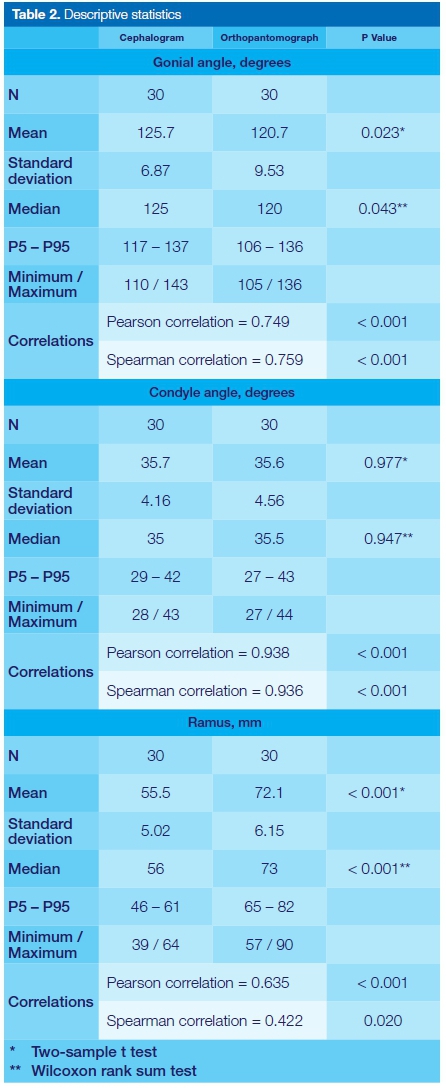
Dolichofacial growth
• The mean as well as the median values of the gonial angles from the lateral cephalogram and orthopantomograph differ significantly
• The mean as well as the median values of the ramus height from the lateral cephalogram and orthopantomograph differ significantly
• The mean as well as the median values of the condyle angles from the lateral cephalogram and orthopantomograph do not differ significantly
• The P5 - P95 intervals for C Ramus and O Ramus are noticeably different, in contrast to the overlap between the lateral cephalogram and orthopantomograph bars for the gonial and condyle angles. Again, significant and positive correlations between the data from two radiographs were found for the gonial angles and the condyle angles. For the ramus measurements, no correlation was found.
RESULTS
The orthopantomograph is a panoramic view, demonstrating the right and left landmarks for bilateral structures. In addition, it displays many anatomic landmarks with enough detail to indicate the possibility of mandibular asymmetries. Therefore, the panoramic radiograph is a valuable orthodontic screening tool and is useful in the formulation of a treatment plan. However, the ortho-pantomograph has some limitations such as image magnification, geometric distortion and superimposed images. This limits accuracy.5
Studies have been undertaken to evaluate the use of orthopantomographs for dentoskeletal measurements.6,7 Some studies have shown that vertical and horizontal linear measurements in orthopantomographs are unreliable. Van Elslande et al., (2008), claimed that although vertical linear measurements were more accurate than horizontal linear or angular measurements, they were not true representations of the real objects to which they corresponded, and therefore caution is advised when using conventional or digital panoramic images to assess linear markers of mandibular asymmetry.8 Larheim and Svanaes (1986), found acceptable reproducibility for vertical linear and angular variables on panoramic radiographs that did not exceed 1% of the total variance, however, horizontal linear variables were less reliable.7 For this reason, many studies have focused only on angular measurements.5
In 1993, Levandoski was one of the first to introduce a method of orthopantomograph analysis for evaluating facial asymmetry.9 In these cases of asymmetry, it was especially challenging to achieve reliable skeletal measurements owing to interferences presented by superimposition of images on the lateral cephalogram.9,10 Since then, few studies have been conducted which have investigated the possibility of enhancing the application of orthopantomographs in the evaluation of changes in craniofacial morphology in comparison with the data gleaned from lateral cephalograms.11
With regards to orthodontics, dimensional measurements made on an orthopantomograph can involve considerable methodological error. One major limiting factor in the clinical use of orthopantomography is its inability to confirm whether the dimensions of structures shown on radiographs correspond to the real dimensions of the structures. The orthopantomographic image is affected by both magnification errors and displacement.
Horizontal distances are particularly unreliable as a result of non-linear variation in the magnification at different object depths, whereas vertical distances are relatively reliable. Distortion, displacement and in a special way, magnification, can cause changes in the dimensions of the images of structures on radiographic films in comparison with those of the actual structures.12,13
Cephalometric radiography is an essential tool in the diagnosis and treatment planning of dental malocclusions and underlying skeletal discrepancies. The use of serial cephalograms makes it possible to study and predict growth, orthodontic treatment progress and the outcome of dentofacial deformity surgical treatment.14
However, the inconsistency in landmark identification is still an important source of random errors in both computer-aided digital cephalometry and in manual cephalometric analysis. Last, but not least, both methods are time-consuming, although to a different extent.15
For these reasons there have been efforts to automate cephalometric analysis with the aim of reducing the time required to obtain an analysis, improving the identification and reducing the errors due to clinician subjectivity.
The main source of errors includes technical measurements, radiographic acquisition and identifying landmarks. The lateral cephalometric radiograph has become a standard tool in orthodontic assessment and treatment planning. The need for lateral cephalometric radiographs in certain patients has always been controversial.
Many authors are of the opinion that study models alone provide adequate information for treatment planning, and the incremental addition of other diagnostic records make minimal difference.16 More recently, studies have noted that, for most patients, the clinical examination, supplemented with study models and photographs, provided adequate information for orthodontic treatment planning. It should be stressed that individually based selection criteria should be used for radiographic examination. Pae et al., (2001) stated that the lateral cephalometric radiograph might influence treatment planning in patients with bimaxillary protrusion and Class II division 2 malocclusion, however cephalometrics does not appear to influence orthodontic treatment planning for Class II division 1 adolescents.17
The popularity of the orthopantomograph stems from the simplicity of the operation, its low radiation dosage when compared with a conventional lateral cephalogram and full mouth periapical radiographs, and the wide field of visible projected structures with reduced superimposition of the investing tissue.18,19
Orthopantomography is a very popular and widely accepted technique of panoramic radiography of the oral region, producing a single image of the facial structures that include both maxillary and mandibular arches with the temporomandibular joints and their supporting structures. It has a wide variety of uses, including the screening of patients before prosthetic treatment for evidence of roots, cysts, foreign bodies, and neoplasms.
Furthermore, it helps in the evaluation of the resorptive and the osteopenic processes of the jaws. In addition, orthopantomography plays an important role in implantology, in as much as it offers information about the vertical dimension of the bone and the locations of certain anatomic structures in the orofacial region.
Therefore, it seems that an orthopantomograph, a simple, inexpensive and a potentially comprehensive diagnostic tool, can be investigated and studied more extensively for determination of angular as well as linear measurements as an indicator of vertical jaw relations.
Based on the findings of our study it can be seen that angular measurements from the two radiographs can be correlated between for all three growth patterns.
There was no significant difference between the angles measured in the groups. The findings also showed that there were no statistically significant differences between the angular measurements of the two radiographs in the normal and horizontal growth patterns. This however this did not apply to the vertical growth pattern. Larger samples may possibly show a different result. The angular distortion in both the images is within the acceptable range and if the images are prepared perfectly and without technical errors, they could be used for clinical measurements.
However, the linear measurements taken from an orthopantomograph and that of a lateral cephalogram radiograph showed little consistency.
CONCLUSION
Angular measurements of both the gonial angle and the condyle angle from the orthopantomograph can be used to assess the dentoskeletal pattern of the patient.
Although a correlation was observed for the angular measurements, further investigations should be undertaken to establish a formula to create norm values to determine the vertical dimension from the orthopantomograph.
Limitation
The study conducted was not race or gender specific. Future studies could be undertaken to investigate these variables.
References
1. Franco! FCM, de AraujolI TM, VogellII CJ, QuintäoiV CCA. Brachycephalic, dolichocephalic and mesocephalic: is it appropriate to describe the face using skull patterns? Dental Press J. Orthod. vol.18 no.3 Maringá May/June 2013. Link: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S2176-94512013000300025. [ Links ]
2. Isaacson JR, lsaacson RJ, Speidel TM and Worms FW. Extreme variation in vertical facial growth and. associated variation in skeletal and dental relations. The Angle Orthodontist, 1971;41:219-29. [ Links ]
4. Rumsey DJ. Statistics for Dummies. 2nd Edition, Wiley. 2011; ISBN 9780470911082. [ Links ]
5. Downs WB. Analysis of the dento-facial profile. The Angle Orthodontist 1956; 26:191-212. [ Links ]
6. Burnstone CJ, James RB, Legan H, Murphy GA, Norton LA Cephalometrics for orthognathic surgery. Journal of Oral Surgery 1979; 36:269-77. [ Links ]
7. Akcam MO, Altiok T, Ozdiler E. Panoramic radiographs: a tool for investigating skeletal pattern. American Journal of Orthodontics and Dentofacial Orthopedics 2003;123(2): 175-81. [ Links ]
8. Larheim TA, Svanaes DB. Reproducibility of rotational panoramic radiography: mandibular linear. dimensions and angles. American Journal of Orthodontics and Dentofacial Orthopedics 1986;90(1): 45-51. [ Links ]
10. Van Elslande DC, Russett SJ, Major PW, Flores-Mir C. Mandibular asymmetry diagnosis with. panoramic imaging. American Journal of Orthodontics and Dentofacial Orthopedics 2008;134(2):183-92. [ Links ]
12. Levandoski RR. Mandibular whiplash. Part I: An extension flexion injury of the temporomandibular joints. The Functional Orthodontist 1993;10(1): 26-9. [ Links ]
13. Piedra I. The Levandoski panoramic analysis in the diagnosis of facial and dental asymmetries. The Journal of Clinical Paediatric Dentistry 1995;20(1):15-21. [ Links ]
14. Ongkosuwito EM, Dieleman MM, Kuijpers-Jagtman AM, Mulder PG, van Neck JW.Linear mandibular measurements: comparison between orthopantomograms and lateral cephalograms.The Cleft Palate-Craniofacial Journal 2009;46(2):147-53. [ Links ]
15. Brooks SL. Guidelines for radiologic examinations: do we have all the answers yet? Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology 1997;83(5): 523-4. [ Links ]
16. Tronje G, Eliasson S, Julin P, Welander U. Image distortion in rotational panoramic radiography. II. Vertical distances. Acta Radiologica. Diagnosis (Stockholm) 1981;22(4): 449-55. [ Links ]
17. Vig KW. Nasal obstruction and facial growth: the strength of evidence for clinical assumptions. American Journal of Orthodontics and Dentofacial Orthopedics 1998;113(6): 603-11. [ Links ]
18. Celik E, Polat-Ozsoy O, Toygar Memikoglu TU. Comparison of cephalometric measurements with digital versus conventional cephalometric analysis. European Journal of Orthodontics 2009;31(3): 241-6. [ Links ]
19. Brown WA, Harkness EM, Cousins AJ, Isotupa K. Treatment planning from study models: an examiner variability study. The Angle Orthodontist 1977;47(2):118-22. [ Links ]
20. Pae EK, McKenna GA, Sheehan TJ, Garcia R, Kuhlberg A, Nanda R. Role of lateral cephalograms in assessing severity and difficulty of orthodontic cases. American Journal of Orthodontics and Dentofacial Orthopedics 2001;120(3): 254-62. [ Links ]
21. Shahabi M, Ramazanzadeh BA, Mokhber N. Comparison between the external gonial angle in panoramic radiographs and lateral cephalograms of adult patients with Class I malocclusion. Journal of Oral Science 2009;51(3): 425-9. [ Links ]
 Correspondence:
Correspondence:
Salahuddien M. Dawjee
Head, Department of Orthodontics. University of Pretoria
Email: s.dawjee@up.ac.za

