










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Dental Journal
versión On-line ISSN 0375-1562
versión impresa ISSN 0011-8516
S. Afr. dent. j. vol.73 no.9 Johannesburg oct. 2018
http://dx.doi.org/10.17159/2519-0105/2018/v73no9a7
CASE REPORT
Hamartomas in the opercula of four unerupted primary molars
N PotgieterI; L RobinsonII; I MiddletonIII
IBChD (UP), PG Dip Dent: Endodontics (UP), PG Dip Paedodontics (UWC), MSc Dent (UP)
IIBChD (UWC), PDD: Maxillofacial Radiology (UWC), PDD: Forensic Odontology (UWC), Registrar: Oral and Maxillofacial Pathology, University of Pretoria
IIIBChD (UP), PG Dip Dent: Endodontics (UP)
ABSTRACT
Odontogenic lesions in the opercula may result in delayed eruption of primary molars.
CASE REPORT: This case presents a rare occurrence of delayed eruption of four primary molars causing interference with normal function. The lesions were surgically excised to expose the underlying first deciduous molars. Histopathological analysis of the excised tissue revealed hamartomatous lesions. These lesions appeared histologically identical to those of an odontogenic giant cell fibroma, consisting of odontogenic epithelial islands with scattered giant cells and histiocytes in a surrounding dense fibrous connective tissue stroma. Occasional dyskeratotic cells were also noted with an intermixed mild, chronic inflammatory cell infiltrate
CONCLUSION: Eruption cysts are traditionally left untreated to resolve spontaneously with the eruption of the underlying teeth. However, lesions that stay unresolved or interfere with function should be surgically excised and sent for histological analysis. The presence of hamartomas in the oper-culum should be considered as a differential diagnosis in persistent unerupted deciduous and permanent teeth
Keywords: Eruption cyst, hamartoma, delayed eruption, odontogenic giant cell fibromatosis
INTRODUCTION
A dome shaped swelling in the mucosa overlying an unerupted tooth is commonly diagnosed as an eruption cyst (EC).1 An EC is a dentigerous cyst that develops when
the dental follicle separates from the crown of an erupting tooth that is still enfolded in the soft tissue overlying alveolar bone.1, 2
The lesions are usually associated with unerupted deciduous mandibular central incisors and permanent first molars, but rarely with deciduous molars.3
Eruption cysts are usually asymptomatic and are conservatively left to rupture spontaneously when the underlying tooth erupts.1, 4, 5 However, surgical intervention should be considered if the EC's cause pain or discomfort, infection or interfere with normal function (i.e. breastfeeding/mastication).4, 6
Persistent multiple EC's on all four first deciduous molars of one patient is a rare occurrence. This paper describes the surgical management and final diagnosis of such a case.
CASE REPORT
A healthy, 19-month-old boy presented with his mother. The main complaint was that swellings in the boy's mouth were interfering with breastfeeding. According to the history, the swellings had been present and had increased gradually in size for approximately eight months. Initially, the referring dentist explained to the mother that the swellings would self-correct on eruption of the primary molars. After a year had lapsed without self-correction and the boy started experiencing functional problems, the dentist referred the patient for further investigation.
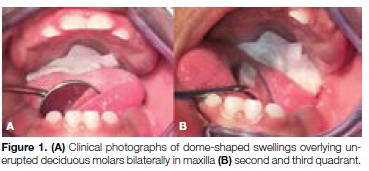
Upon clinical examination, dome-shaped lesions were noted in all four quadrants in the areas where the first deciduous molars were expected to erupt. The swellings were the same colour as surrounding mucosa with a slight bluish tint and were soft and tender on palpation (Figures 1A and B). The patient could not close the mouth completely due to the size and location of the lesions. No other clinical pathological findings were noted. Due to the patient's age and cooperation it was decided not to expose the child to radiation for radiographic examination. A clinical diagnosis of multiple eruption cysts was made.
The child was examined by the anaesthesiologist and cleared for general anaesthesia. All four cysts were surgically removed through elliptical incisions made with a surgical blade (Figure 2A).

Clear fluid was drained once the mucosa was cut. The incisions were made larger than normal to prevent tissue contact and reattachment. The excised tissues were sent for histopathological analysis. Bleeding was easily controlled without any sutures or haemostatic agents (Figure 2B). Post-operative instructions were given to the mother and follow-up visits were scheduled.
At the one-week clinical follow-up (Figure 3A), the tissues surrounding all four teeth were sound with slightly rolled borders and marginal inflammation. All four deciduous first molars were clearly visible. The mother reported an improvement in feeding and did not report pain or discomfort experienced by the boy. At the three-week follow-up (Figure 3B), all signs of gin-gival inflammation had cleared and the infant functioned and fed well.

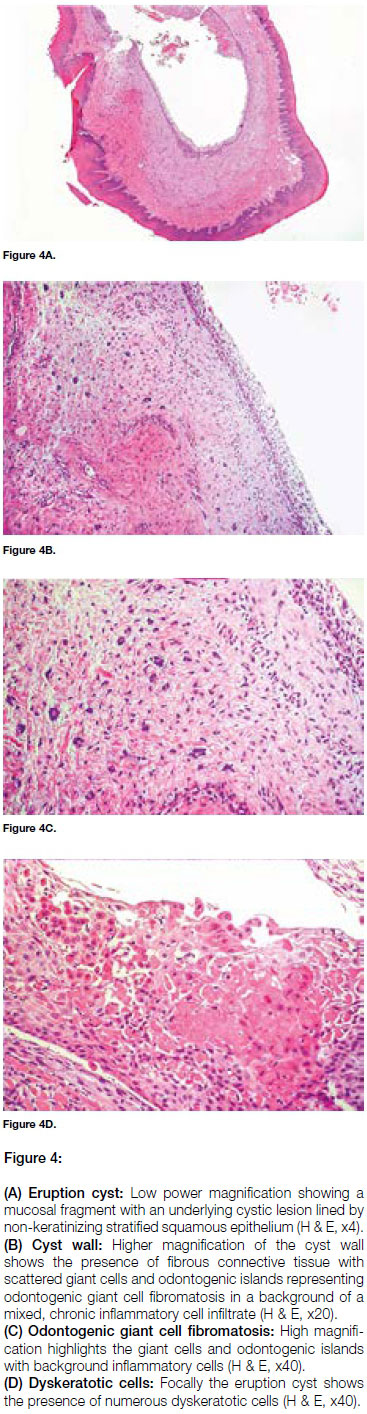
Histological analysis confirmed the diagnosis of multiple eruption cysts with the presence of odontogenic giant cell fibromatosis in the overlying mucosa. The lesions showed the presence of odontogenic epithelial islands with scattered giant cells and histiocytes in a surrounding dense fibrous connective tissue stroma. Occasional dyskeratotic cells were seen, which were more abundant in one fragment, and a mild, chronic inflammatory cell infiltrate was present within the surrounding fibrous connective tissue (Figures 4A to D).
DISCUSSION
Biopsies from the opercula overlying the impacted first deciduous molars showed increased odontogenic epithelial rests that varied in size and shape. These epithelial rests may obstruct normal tooth eruption.7
These lesions have been described using terms such as 'odontogenic giant cell fibromatosis (OGCF)' and 'peri-coronal hamartomatous lesions'.8 The term hamartoma can be defined as a "non-neoplastic, unifocal/ multifocal developmental malformation".9 While the pathogenesis of hamartomas remain speculative, it is known that these tissues are most commonly derived from the mesoderm.10
The hamartomas in our patient corresponded to OGCF, a term first coined by Philipsen et al.,7 to describe an odontogenic hamartomatous lesion present within the opercula of permanent first and second molars with delayed eruption. Histologically, OGCF presents as a non-encapsulated lesion consisting of dense fibrous connective tissue containing a large number of spindleshaped or stellate cells and large multinucleated cells, proliferating strands and islands of odontogenic epithelium with occasional squamous cell metaplasia and no calcifications present.8
These multinucleated giant cells and stellate cells, found in great number in these lesions, are histologically identical to those described in giant cell fibromas.7 The patient in question presented with a focal area of dyskeratotic cells in the wall of the cyst which is a rare phenomenon, but is well documented in odontogenic cysts. The strong association between OGCF and mandibular impacted molars suggests that the biology of these hamartomatous lesions differs from that of "classic" odontogenic tumors.7
Both Philipsen et al.7 and Yonemochi et al.11 concluded that the presence of hamartomatous lesions in the pericoronal areas of teeth may cause delayed eruption which can interfere with the pathway of an erupting tooth, causing tissue derangement and remodelling. 7, 8, 11
The odontogenic hamartomas presenting in this case were successfully resolved following conservative surgical incision. Odontogenic hamartomas are non-neoplastic and once they have been resolved, there is little chance of recurrence.12
CONCLUSION
In this case report, the delayed eruption of primary molars, which is uncommon, is described and is attributed to eruption cysts, characterised by OGCF hamartomatous lesions in the opercula. Failure to spontaneously resolve and a reduced ability to breastfeed resulted in a decision to treat the cysts surgically.
Conservative surgical intervention resulted in the successful eruption of all four primary molars, improved function and overall quality of life.
Disclosure
The authors declare no conflicts of interest related to the case reports depicted in this article.
ACRONYM
EC: Eruption Cyst
OGCF: Odontogenic Giant Cell Fibromatosis
References
1. Neville BW, Damm DD, Chi AC, Allen CM. Oral and Maxillofacial Pathology: Elsevier Health Sciences, 2015. [ Links ]
2. Kramer IR, Pindborg JJ, Shear M. Histological Typing of Odon-togenic Tumours: Springer Science & Business Media, 1992. [ Links ]
3. Bodner L, Goldstein J, Sarnat H. Eruption cysts: a clinical report of 24 new cases. J Clin Pediatr Dent. 2005; 28 (2):183-6. [ Links ]
4. Shaul H, Chatra L, Shenai P, Rao P, Veena K, Prabhu R. Eruption cyst: a case report. Pac J Med Sci. 2013; 11(1):34-8. [ Links ]
5. Boj J, Poirier C, Espasa E, Hernandez M, Jacobson B. Eruption cyst treated with a laser powered hydrokinetic system. J Clin Pediatr Dent. 2006; 30 (3):199-202. [ Links ]
6. Bernardes Gonçalves Weber P, Cezar Ilha M, Silvana Borges T, Castilhos Ruschel H, Floriani Kramer P, Ferreira SH. Eruption cyst associated with tooth rotation on deciduous dentition: A case report. Stomatos, 2015; 21 (40):21-6. [ Links ]
7. Philipsen HP, Thosaporn W, Reichart P, Grundt G. Odontogenic lesions in opercula of permanent molars delayed in eruption. J Oral Pathol Med. 1992; 21(1): 38-41. [ Links ]
8. Nikitakis NG, Parashar P, Terezides A, Sarlani E. Dental follicular hamartomas in the opercula of teeth delayed in eruption: A case report and review of the literature. Oral Oncol Extra. 2006; 42 (3): 129-32. [ Links ]
9. Patil S, Rao RS, Majumdar B. Hamartomas of the oral cavity. J Int Soc Prev Com Dent. 2015; 5(5): 347. [ Links ]
10. Berman JJ. Neoplasms: Principles of Development and Diversity: Jones & Bartlett Learning, 2009. [ Links ]
11. Yonemochi H, Noda T, Saku T. Pericoronal hamartomatous lesions in the opercula of teeth delayed in eruption: an immuno-histochemical study of the extracellular matrix. J Oral Pathol Med. 1998; 27 (9): 441-52. [ Links ]
12. Barnes L. Surgical Pathology of the Head and Neck: CRC Press, 2000. [ Links ]
 Correspondence:
Correspondence:
N Potgieter
Tel +27 (0)12 319 2932
Email: nicoline.potgieter@up.ac.za

