










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.73 n.4 Johannesburg May. 2018
DENTAL EDUCATION
Dental clinical teachers' perceptions of their teaching role.
Maart RI; Gordon NII
IBChD, PDD (Comm Dent), MPhil (Higher Education) Stomatologist /Senior Lecturer Department of Prosthetic Dentistry University of the Western Cape
IIDip OH, BA, MPH, Adv DiplAdult Education, Department of Oral Hygiene, University of the Western Cape. ngordon@uwc.ac.za
SUMMARY
INTRODUCTION: Clinicians often occupy a clinical teaching role without being adequately prepared for or orientated to the associated demands.
AIM: Explore perceptions of clinical teachers at the Faculty of Dentistry (UWC).
Method
RESULTS: A cross-sectional research design was used. Full and part-time clinical teachers (n=66) employed in 2014 were included. Data was gathered using a questionnaire administered via the online Survey Monkey® system. : The response rate was 47% (n=31). The top five qualities of a clinical teacher were -understanding students, patience, subject knowledge, passion/commitment and communication. The top five competencies were: clinical skills and experience, subject knowledge, good communication, good teacher, role model. All respondents selected "availability throughout a clinical session, punctuality at a clinical session and identifying gaps in procedural/clinical aspects in the patient care" as important roles of a good clinical teacher. Differences in perceptions of clinical roles were seen between full and part-time clinical teachers
CONCLUSION: Clinical teachers' perceptions of their teaching role was to a great extent in line with best practice as indicated in the literature. Faculty teaching and learning initiatives should highlight the clinical teacher role, harness the unique perspectives of full and part-time clinical teachers and address barriers that may hinder this process.
INTRODUCTION
A core dimension of the lecturer role at dental schools is that of a clinical teacher, also referred to as a clinical supervisor. Clinical supervision is defined as 'monitoring, guidance and feedback on matters of personal, professional and educational development in the context of patient care'.1 The largely clinical nature of dental education makes the use of best practice in clinical teaching essential. Yet literature shows that clinicians often occupy a clinical teaching role without being adequately prepared for the special demands of the post.24
Best practice in clinical teaching has been identified within the domains of positive role modelling; competent and compassionate health care provision; effective supervision and mentoring; use of varied teaching approaches and being supportive.5 Considering that a role model demonstrates a standard of excellence which should be imitated,6 it is vital for trainees and trainers to be aware of positive and negative role modelling so that trainers demonstrate and trainees imitate the appropriate professional behaviour.5 Dental student opinons of 'inconsistent and sometimes insensitive feedback' highlights that students could identify negative teaching and personal qualities modelled to them.7,8
The clinical environment is an authentic learning platform for students as they treat patients under supervision of qualified dental professionals. This one-to-one interaction is a key element in student learning.9 To support learning, clinical teachers should provide specific feedback on student performance, show an interest in teaching, motivate students, be able to translate didactic information into patient care situations, show compassion and approach patient treatment in a proactive manner.17 Feedback should facilitate learning,4 include appropriate cognitive feedback to the student,10 be contextual,11 be part of any assessment to improve the students' clinical skills and reinforce good practice.12 Students reportedly valued supervisor feedback, regarding immediate and constructive feedback as most helpful.7-8-13 The one-minute Preceptor model as a framework for clinical teaching, identifies five micro-skills to guide the teacher.14 These are securing a commitment from the student on actions they intend taking, probing for supporting evidence to explore the 'mindmap' of the student, teaching general rules, reinforcing what is done correctly and correcting mistakes. An additional factor in the teaching and learning process is that dental educators may be at different stages of didactic competence, ranging from a novice that is new to teaching to the expert where teaching has become instinctive and intuitive.15
The background and professional status of staff6,17 and concerns regarding curriculum and students18 appear to influence clinical teaching. Sweet et al.16 reported that practitioners viewed their role as supervision rather than teaching; that senior academics tended to be resistant to change particularly when such change challenged the authority of their discipline; that intuitive teachers tend to emphasise practical learning; and that trained academics focussed on education theory and critical thinking.16 Furthermore, supervisors reported a lack of clear objectives and expectations, considered that teaching was pitched at the wrong level and that there was a lack of active participation with a focus on recall rather than problem solving by learners.
AIMS AND OBJECTIVES
The purpose of this descriptive study was to explore the perceptions of clinical teachers at Faculty of Dentistry (UWC) regarding their roles in the clinical environment in order to inform faculty teaching and learning initiatives. The objectives were to determine their demographics, perceptions of their role as clinical teachers, barriers experienced in fulfilling their role as clinical teachers and suggestions to promote excellence in clinical teaching at the faculty.
METHOD
The Faculty of Dentistry (UWC) routinely offers teaching and learning initiatives for part-time and full-time staff. One such Initiative includes a monthly Faculty Journal club on Teaching and Learning, with a strong emphasis on clinical teaching. A core group of 10-15 staff attend these discussions although the topic and logistics are contributing factors to attendance.
Clinical teachers at the Faculty are generally drawn from full-time academic staff across clinical departments and part-time staff from private practice. Part-time staff is a feature of dental education for the clinical expertise they provide and the fact that dental student numbers are increasing without a concomitant Increase in full-time staff. Full and part-time clinical teachers were Included in this study as they may have different perceptions on their role within the clinical environment, which could influence their actions as clinical teachers.
This was a quantitative, cross sectional study of all clinical teachers (n=66) employed in the Faculty of Dentistry in 2014.
Data was collected by means of a questionnaire using open-ended and closed questions.
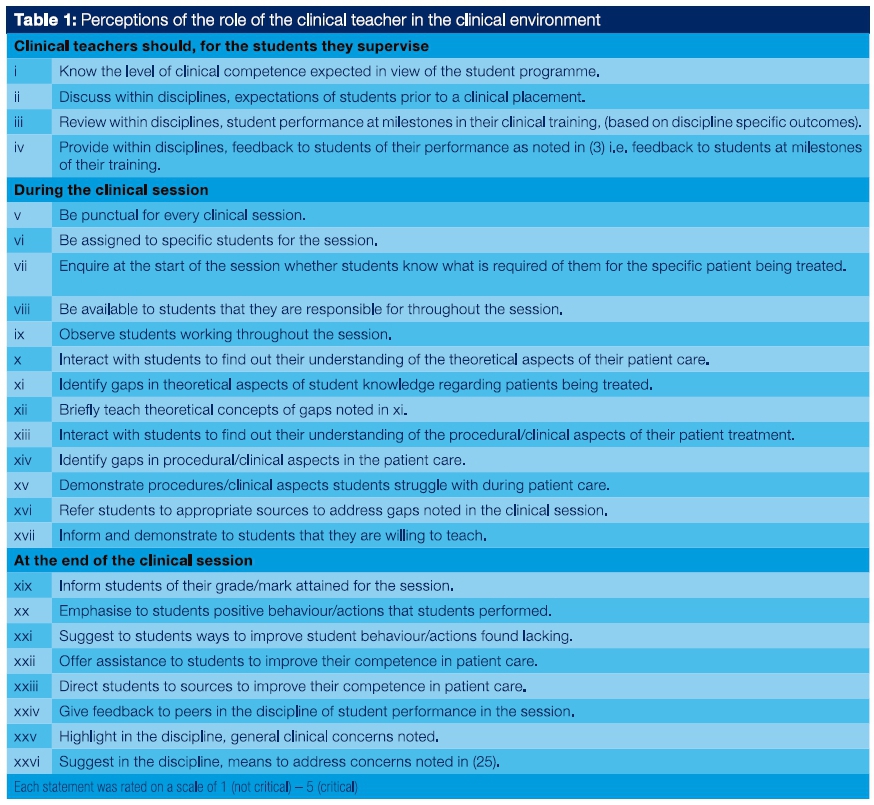
The questionnaire focused on the perceptions of clinical teachers on their role in teaching within the clinical environment and the barriers they experienced in executing this role. Included were: 1) teacher demographics, 2) open-ended questions about perceptions of qualities and competencies of the clinical teacher, 3) details of barriers to fulfilling the role of a clinical teacher and 4) suggestions to promote excellence in clinical teaching. A set of 26 statements were prepared, structured around the role of the clinical teacher before, during and after a clinical session, to enquire about perceptions on the process of clinical teaching (Table I). Respondents were asked to react to these statements on a five-point scale namely 'critical (5), 'important' (4), 'useful' (3), 'not important' (2) and 'not critical' (1). The questionnaire was administered using the online SurveyMonkey system (Palo Alto, CA, USA).
Face and content validity of the questionnaire were addressed by the critical scrutiny of colleagues in the Dental Faculty who have done research in the field of clinical teaching. A pilot study was conducted and format changes were made for more user friendly online application.
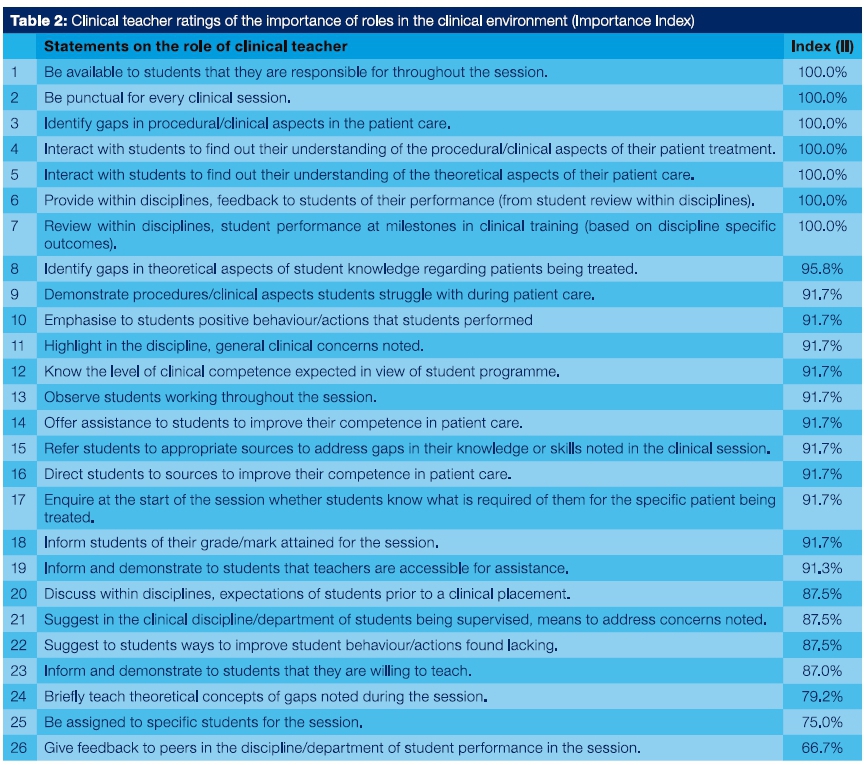
Open-ended data were summarised using descriptive frequency tables. The Chi-square test was used to test for significant relationships between categorical demographic information. Where the assumptions of the Chi square test were not met the alternative output of likelihood ratio was used. The non-parametric Independent Samples Kruskal-Wallis test was used to compare the distribution of responses for the different demographic features of the clinical teacher. An importance index (II) was calculated for each question on the importance of the role of the clinical teacher by subtracting the total number of responses in the 'critical' and 'important' categories from the total of responses for the 'not important' and 'not critical' (Table II).
Data were entered into the Statistical Products and Solution Services (SPSS) version 22. Quantitative data were analysed using frequencies and percentages. Chi square test statistics was used to test for associations (p>0.05) between the profile of clinical teachers and their perceptions.
Ethical clearance was obtained by the University of the Western Cape Ethics Committee. Participants were invited to participate in the study using staff email addresses with a link to SurveyMonkey if they chose to partake. The research purpose was explained in the online survey and anonymity was assured by the online system.
RESULTS
The response rate was 47% (n=31). The 21 full-time and 10 part-time staff who responded were mostly female (75%) with the majority reporting a Bachelor of Dental Sciences (BDS) as one of their qualifications. The professional status of full-time staff was almost evenly spread in terms of lecturer (38.1%), senior lecturer (33.3%) and professor (28.6%), whereas part-time staff were primarily lecturers (85.7%) and professors (14.3%). Full-time teachers had overall higher professional status (p = .036) and significantly more years of experience in clinical teaching (p = .015). Sixty percent (60%) of part-time and 23% of full-time clinical teachers had less than 11 years of experience,
QUALITIES OF CLINICAL TEACHERS
The top five qualities identified were understanding students (n=13), patience (n=10), subject knowledge (n=8), passion/commitment (n=7) and communication (n=7). Part-time teachers perceived 'understandingstudents', 'communication'and'subjectknowledge' less important as a teacher quality than did the full-time teachers (p = .029, ρ = .027, ρ = .05 respectively).
Competencies of clinical teachers
The top five identified competencies of a clinical teacher were : clinical skills and experience (n=18), subject knowledge (n=16), good communication (n=7), good teacher (n=6) and role model (n=4). Part-time clinical teachers perceived clinical skills and experience more important as a competency than the did the full-time teachers (p=.05; ρ = .038 respectively).
Perceptions on the role of the clinical teacher The median values for all 26 items (Table 2) on the clinical teacher roles were between 4 and 5 for the combined responses of full and part-time clinical teachers, indicating that respondents regarded all roles as important. However, full-time clinical teachers perceived observing students working throughout the session as less important than did the part-time clinical teachers (p=038).
Females perceived the following statements as more important than males (p<0.05):
-
'Suggest to students ways to improve student behaviour/ actions found lacking',
-
'Give feedback to peers in the discipline of student performance in the session',
-
'Highlight in the discipline, general clinical concerns noted'.
-
Perceived barriers for clinical teachers
-
Barriers reported to fulfilling their roles as clinical teachers were categorised as:
-
'The teacher': too many students per teacher, too much administrative work, unmotivated staff, publication pressure, clinical load.
-
'The student': unprepared/unmotivated students, poor student ethics towards patients, punctuality.
-
'Curriculum issues': lack of curriculum review, poorly planned assessments, lack of tutorial sessions, contradictory teaching in relation to evidence-base.
-
'The clinical environment': limited space, logistics around materials and patient files, and outdated technology.
Suggestions to promote excellence in clinical teaching
Suggestions for the Faculty to promote excellence in clinical teaching were categorised as:
-
'The teacher': acknowledge valuable input of all clinical teaching staff, collegiality among staff around professionalism/ rules/discipline, smaller student groups, employ young energetic hard working teachers, comparable salaries with other universities,
-
'The curriculum': compulsory student evaluation before they enter clinics, standardise concepts across disciplines, Improve assessment tools, establish clear evidence base, cross department seminars/discussions,
-
'The clinical environment': sufficient and available consumables/working equipment and support staff, clinical protocols in place, more comfortable working environment such as air conditioning, improve logistics around files, Introduce information technology systems,
-
'Other': collaborate with other dental faculties nationally.
DISCUSSION
The stronger academic status of full-time teachers is possibly a result of a more enabling environment that would allow them to pursue an educational trajectory to use resources such as journal club attendance to equip them for clinical teaching. If part-time clinical teachers are seen as integral to the teaching and learning project, higher education institutions must create opportunities for them to develop the necessary competencies, while recognising the skills they bring to this project. Training programmes should emphasise that being a dental educator is an ongoing journey where educators are expected to maintain and improve teaching practice throughout their careers.15
Excellence in clinical teaching requires 'clinical knowledge of medicine, of specific patients, and of context plus an educational knowledge of learners, general principles of teaching, and case-based teaching scripts'.5 Effective supervisors need to have good Interpersonal skills, good teaching skills, be clinically competent and knowledgeable in addition to supervisory skills.1,4-6,8-22 The manner in which these terms are defined integrates the traditional supervisory and teaching roles and supports their interchangeable use in the literature. However, the results of this study show that the perceptions of part-time staff do not fully encompass their teaching role in the clinical environment; these differences are in line with Sweet et al.,16 that the background of dental staff is also reflected in their understanding of teaching development needs.
Broad themes of teacher qualities identified in this study are also reported in the literature.3,7,20 Perceptions of ideal clinical teachers agreed between students and faculty were, "stimulating, encouraging, competent, communicates, and well-read",21 suggesting that students can identify the teacher from whom they can learn. The notion of respect and role-modelling is inherent in the teacher qualities identified. Respect of students contributes to their professional development and shows them the correct attitude towards patients and colleagues.6,20 At the same time standards of excellence are modelled to students.6
Clinical competence, reported as among the most important attributes of an effective clinical teacher,22 was also noted in this study with reference to clinical skills, experience and subject knowledge. The fact that part-time clinical teachers perceived clinical skills and experience more important as a competency than did the full-time teachers further reflects differentials in practice background and highlights the contribution of part-time teachers to professional education and training. Full-time staff engage with students in a classroom and clinical environment, creating an opportunity for daily interaction17 which may broaden their understanding of the dimensions of the learning process within the clinical environment as noted in this study.
Participant response (Table 2) shows that clinical teachers are for the most part aware of the dimensions of positive feedback in terms of the need to observe students, offer assistance, emphasise positive behaviours, inform them of grade marks and direct them to appropriate learning resources. Positive feedback can reinforce effective behaviours, suggest new behaviours that may be helpful in the future and correct mistakes.14 The actions noted are in line with the One-Minute preceptor model,14 an indication of consistent feedback, and shows participant understanding that feedback facilitates learning4 There was an apparent contradiction in the lower rating of the importance of engaging departments/disciplines before and after clinical sessions around student expectations and performance (Table 2) and suggestions to improve excellence in clinical teaching. This dissonance may require clarification of the roles and responsibilities of clinical teachers within the broader faculty structures.
Part-time clinical teachers rated 'observing students working throughout the session' higher than full-time clinical teachers. This may indicate an implicit understanding of their role in guiding the student to perform the correct procedure at the correct time and reflects their practice experience. Part-time practitioners saw their role as supervisors rather than teachers, indicating that they may have 'interesting techniques' to share.16 Conversely, full-time clinical teachers rated this activity less important and may still be rooted in a traditional clinical supervisory role where they see themselves as assessing the outcome of the procedure rather than guiding the process thereof.
Barriers identified were similar to challenges in clinical teaching reported in the literature,4,7,18,23 highlighting the fact that these barriers may need to be addressed at different levels within the Faculty. Medical teachers reported similar concerns with additional problems such as pressure from commitment to the multiple roles of the academic,18,24 having relationships with several agencies such as the University and the National Health System and a lack of incentives and rewards for teaching and patient related factors.24 Recommendations made by respondents appear to address the barriers identified, indicating that staff know how their challenges in the clinical environment can be addressed. Of Interest is that the notion of rewards and incentives24 to promote excellence in clinical teaching was not reported by any staff.
Teacher competence and the learner-educator relationship are significant contributors to the academic success of students and to the way in which future clinicians work as members of a team and as caring professionals.25 Forums where clinical teachers can explore issues of teaching and learning have the potential to create vibrant learning communities.26 The suggestions of respondents on ways to promote excellence in clinical teaching lends to the creation of a community of practice in clinical teaching which has been shown to contribute to a more collegial and positive work environment amongst dental hygiene educators.27 Journal club discussions at the Dental Faculty, as part of the broader Faculty processes to develop excellence in clinical teaching and learning, may be a niche for such a community of practice. Therefore, understanding the perceptions of clinical teachers may guide appropriate interventions that would promote best practice and excellence in clinical teaching.
The results of this study should be interpreted against the response rate as individuals who chose not to participate may have different perceptions. The small number of respondents in each of the professional status categories may explain the lack of significance between staff background and teaching perceptions as noted in the literature.
CONCLUSION
This study found that the perceptions of respondents regarding clinical teaching were to a great extent in line with best practice according to the literature. Faculty teaching and learning initiatives should highlight the clinical teacher role for all staff, harness the unique perspectives that full and part-time clinical teachers bring to the teaching platform to maximise clinical teaching and learning while simultaneously addressing barriers that may hinder this process.
Acknowledgement
We, the authors, owe a debt of gratitude to the late Professor Wendy McMillan for her inspiration and to pursue excellence in clinical teaching. Also acknowledgement for funding received from Deputy Vice-Chancellor for Teaching and Learning towards statistical support.
References
1. KilminsterSM, Cottrell D, Grant J, Jolly B.AM EE Guide No. 27: Effective educational and clinical supervision. Med Teach. 2007; 29:2-19. [ Links ]
2. Ramani S, Leinster S. AMEE Guide no 34: Teaching in the clinical environment. Med Teach. 2008;30:347-64. [ Links ]
3. Singh S, Pai DP, Sinhal NK, Kaur A, Kyaw Soe HH, Barua A. Qualities of an effective teacher: what do medical teachers think? BMC Medical Education 2013; 13:128 Available at: http://www.biomedcentral.com/1472-6920/13/128. Accessed 2/17/2016. [ Links ]
4. Polyzois I, McLoughlin J, Kelly A, Claffey N. Clinical teaching in restorative dentistry and the variation between students' and supervisors' perceptions of its effectiveness. Eur J of Dent Educ. 2010;14:92-8. [ Links ]
5. Irby DM. What clinical teachers in medicine need to know? Acad Med. 1994; 69(5):333-42. [ Links ]
6. Jochemsen-van der Leeuw R, van Dijk Ν., van Etten-Jamaludin F, Wieringa-de Waard Μ. The attributes of the clinical trainer as a role model: A systematic review. Acad Med 2013; 88(1):26-34. [ Links ]
7. Henzi D, Davis E, Jasinevicius R, Hendrickson W. North American dental students' perspectives about their clinical education. J of Dent Educ. 2006; 70(4):361-77. [ Links ]
8. Gordon NA. Learning experiences of oral hygiene students in the clinical environment. Int J Dent Hygiene 2013; DOI:10.111/idh.12039. [ Links ]
9. Fugill M. 2005. Teaching and learning in dental student clinical practice. Eur J of Dent Educ 2005; 9:131-6. [ Links ]
10. Bowen J. Educational strategies to promote clinical diagnostic reasoning. New EngL J Med 2006; 355:2217-25. [ Links ]
11. Hattie J, Timperley H. The power of feedback. Review of Educational Research 2007; 77 (1):81-112; DOI:10.3102/003465430298487 [ Links ]
12. Harden R. Assess clinical competence- an overview. Med Teach. 1979; 1(6):289-96. [ Links ]
13. Winning T, Lim Ε, Townsend G. Student experiences of assessment in two problem-based dental curricula: Adelaide and Dublin. Assessment and Evaluation in Higher Education 2005; 30(5):489-505. [ Links ]
14. O'Neher, J, Stevens N. The One-minute Preceptor: shaping the teaching conversation. Family Med. 2003; 35(6):391-3. [ Links ]
15. Chuenjitwonga S, Oliver RG, Bullock AD. Competence, competency based education and undergraduate dental education: a discussion paper. European Journal of Dental Education 2016; 22(2018) 1-8. [ Links ]
16. Sweet J, Wilson J, Pugsley L. Chairside teaching and the perceptions of dental students in the UK. Β Dent J. 2008; 205(10): 565-9. [ Links ]
17. Allison-Jones L, Hirt J. Comparing the teaching effectiveness of full time and part time clinical nurse faculty. Nursing Educ Perspective 2004; 25(5): 238-43. [ Links ]
18. Spencer J. Learning and teaching in the clinical environment. BMJ. 2003; 326:591. [ Links ]
19. Reeves J. Why teachers adopt a controlling motivating style towards students and how they can become more autonomy supportive. Educational Psychologist 2009; 44(3):159-75. [ Links ]
20. Duvivier RJ, Van Dalen J, van der Vleuten CP, Scherpbier AJ. Teacher perceptions of desired qualities, competencies and strategies for clinical skills teachers. Med Teach. 2009; 31:634-41. [ Links ]
21. Morrison EH, Hitchcock MA, Harthill Μ, Boker JR, Masunaga H. The on-line clinical teaching perception inventory: A 'snapshot' of medical teachers. Fam Med. 2005; 37(1):48-53. [ Links ]
22. Büchel TL, Edwards FD. Characteristics of effective clinical teachers. Fam Med. 2005; 37(1):30-5. [ Links ]
23. Alhaqwi AI, van der Molen HT, Schmidt HG, Magzoub E. Determinants of effective clinical learning: a student and teacher perspective in Saudi Arabia. Education for Health 10 (online) 201; 369. Available at :http://www.educationforhealth.net. Accessed 10/29/2008. [ Links ]
24. Stark P. Teaching and learning in the clinical setting: a qualitative study of the perceptions of students. Med Educ. 2003; 37:975-82. [ Links ]
25. McMillan W. 'Then you get a teacher'-Guidelines for excellence in teaching. Med Teach.29: e209-e2007: 218. [ Links ]
26. Irby DM. Excellence in clinical teaching: knowledge transformation and development required. Med Educ. 2014; .48:776-84. [ Links ]
27. Cara LT, Doucette Η, Neish NR, Mailet P. A model for cultivating dental hygiene development within a community of practice. J of Dent Educ 2012; 76 (3):311-21. [ Links ]
 Correspondence:
Correspondence:
RD Maart
Stomatologist /Senior Lecturer, Department of Prosthetic Dentistry
University of the Western Cape,
Private Bag X1 Tygerberg 7505
Tel. +27 21 9373181
Fax. +27 21 931 2287
Email rmaart@uwc.ac.za


{kind=link}
{kind=link}