










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.73 no.4 Johannesburg Mai. 2018
REVIEW
Comparing patient-based outcomes related to neutral zone and conventional mandibular dentures: A systematic review
Geerts GI; Khan SII
IBChD, PG Dip Implantology, MChD, PhD Prosthodontist/Associate Professor/Senior Lecturer, Department of Restorative Dentistry, University of the Western Cape, Tygerberg Campus, Fransie van Zyl Drive, Parow 7505
IIBChD, PDD, MSc, PhD Dentist / Senior Lecturer, Department of Restorative Dentistry, University of the Western Cape, Tygerberg Campus, Fransie van Zyl Drive, Parow 7505 +27 21 9373000 skhan@uwc.ac.za
SUMMARY
INTRODUCTION: neutral zone mandibular dentures are considered to be superior to conventional complete dentures.
AIM: To synthetize evidence regarding patient-based outcomes of treatment with complete mandibular dentures following static or dynamic methods of establishing denture shape.
OBJECTIVE: To answer the question: "In edentulous patients, what is the effect of neutral zone dentures on oral health-related quality of life and preference as compared with conventional dentures?"
METHODS: Medline, Wiley, Cochrane Central Register of Controlled Trials, Proquest, Elsevier, Trip and Science Direct databases were searched for clinical studies, using a specific search strategy.
RESULTS: From a total of 103 records, 9 studies (participants n=270) were included in the review, based on specific selection criteria. Reports on oral health-related quality of life and preference produced conflicting results. Most patients reported improvement in retention, stability, comfort, chewing, speech with fewer recall visits for neutral zone dentures. High level of heterogeneity in study design, patient-based outcomes, instruments and statistical analysis was encountered, preventing meta-analysis. Quality of most studies was low, with small sample sizes (range: n=5-128), short follow-up periods (5 days-2 months), and high level of selection, performance and detection bias.
CONCLUSION: Results should be interpreted within the context of little and low-level scientific evidence.
INTRODUCTION
Conventional complete dentures (CD) have been the most common and only treatment modality for rehabilitation of edentulousness until the introduction of dental implants. Implant-retained or Implant-supported prostheses have been proven to be superior to conventional CDs in terms of patient-based outcomes (PBOs).1 However, implant therapy may be out of reach of patients due to a variety of reasons. This group of patients is and will continue to be dependent on traditional CDs to restore form and function. It is assumed that these patients would benefit if dentures were made to be as stable and comfortable as possible.
The neutral zone (NZ) concept has been defined as "the potential space between lips and cheeks on the one side, and tongue on the other side; that area or position where forces between tongue and cheeks and lips are equal".2 As early as 1746, Fauchard advocated that the inside and outside form and shape of dentures should be considered carefully in order to avoid conflict with lips, cheeks and tongue (in: Lott and Levine, 1966).3 Today, there is a high level of International consensus that teeth should be arranged in a neutral position and that arch form should assist stability during function.4
While experts may agree, there appears limited scientific evidence based on patient feedback on the clinical benefits of CDs made according to a dynamic NZ method (NZD) over a biometric, static method of determining arch form and shapes of dentures. To date, no systematic review of clinical studies comparing PBOs of the mandibular NZD versus a conventional mandibular CD has been done. Therefore, the efficacy of NZDs compared with CDs has yet to be established.
The aim of this systematic review was to synthesize scientific data related to PBOs of mandibular CDs fabricated according to the NZ concept as compared with conventional methods.
The objectives of this systematic review were:
1. To identify clinical studies comparing PBOs of mandibular NZDs versus conventional CDs
2. To extract and compare data based on PBOs of both types of dentures from studies included in the review
3. To perform a meta-analysis should the nature of the data identified from the clinical studies allow this to be done.
Hence, the following research question was developed: In edentulous adult patients, what is the effect of NZD on oral health-related quality of life (OHRQoL), patient satisfaction, and preference as compared with that of conventional mandibular CDs?
METHODS
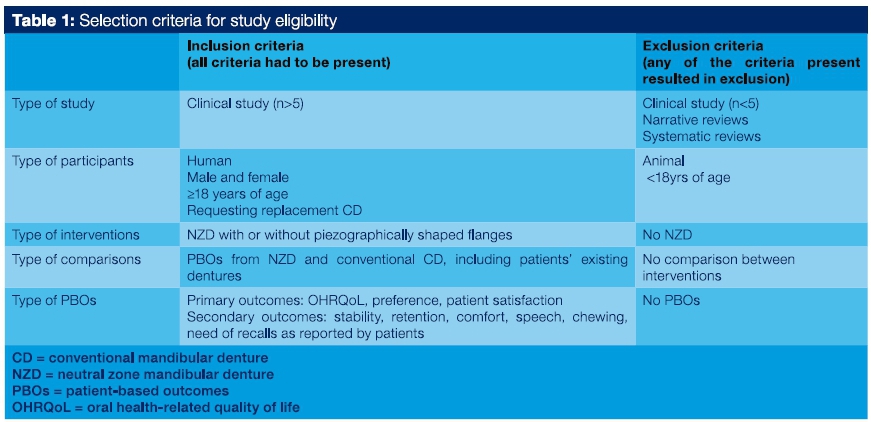
A protocol was developed to Include all aspects of a systematic review: a search strategy, selection criteria (Table 1), the use of customized study eligibility and data extraction forms, assessment of risk of bias (RoB) using the Cochrane tool,5, 6 and statistical analysis by calculating risk ratios for outcomes using 95% confidence intervals. The protocol was registered with the Biomedical Research Ethics Committee at the University of the Western Cape (BM/17/4/9).
Search and Selection Strategy
Online searches were conducted for primary and ongoing studies to Identify literature on the topic of NZ as a treatment strategy for edentulous adult patients. Two reviewers {GG and SK) Independently and systematically searched for studies using the databases Medline, Wiley, Cochrane Central Register of Controlled Trials, Proquest, Elsevier, Trip and Science Direct. Medical subject headings (MESH terms) were applied In databases which allowed this function. Key terms were combined using Boolean operators and search strategies were developed for each database using database specific functions. For Pubmed, the search terms were: Neutral zone AND complete dentures and the following article types were selected: Case Reports, Clinical Study, Clinical Trial, Clinical Trial Phase I, Clinical Trial Phase II, Clinical Trial Phase III, Clinical Trial Phase IV, Comparative Study, Controlled Clinical Trial, Multicenter Study, Observational Study, Pragmatic Clinical Trial, Randomized Controlled Trial. A similar search strategy was developed and modified according to the requirements of each database to ensure inclusion of all relevant studies. If databases allowed It, the following filters were applied: publication dates (1930-2017), species (human), ages (18+ years). No language filters were activated. Similar articles listed for each reference were also searched for possible inclusion. Based on titles and abstracts, a first selection of articles was done. Full texts of these selected articles were retrieved. Eligibility of these articles was determined using the customized eligibility tool. Reference lists of Included studies were searched for additional records. Where full texts were unavailable, authors were contacted. Efforts were also made to obtain English versions of studies reported In other languages either by requesting them from the authors or using language experts to translate key findings. At every level of selection, consensus was reached between the two reviewers, adopting a lenient approach towards Inclusion of records.
Data extraction
The two reviewers Independently reviewed all Included full-articles extracting the following data using the standardized data extraction sheet: authors, title, date, country, publication type, study method, estimate of bias, sample (number, age, sex), Interventions, outcomes, statistical analyses, results, conclusions, funding sources, ethics clearance, comments and correspondence required.5 Extraction sheets were compared. Differences were discussed until consensus was reached. Where more than one article reported different aspects of the same study, these were combined as a single study. Data from the Included and excluded studies were summarized in tables of included and excluded studies respectively.
Qualitative analysis
The two reviewers independently evaluated the included studies for RoB using the Cochrane's 'Risk-of-bias assessment tool'.5, 8 Risk of bias was assessed across the following components: Sequence generation and allocation concealment to prevent selection bias; Blinding of participants, personnel and outcomes assessors to reduce performance bias; Incomplete outcome data to eliminate attrition bias; Selective outcome reporting to reduce selective outcome reporting bias; and other sources of bias, such as those related to specific study designs, early stoppage, fraudulent or extreme baseline imbalances. Risk of bias for each component was scored as 'high', 'low' or 'unclear'. Bias was summarized in RoB graphs for each study in the Review Manager Software program.6
Data synthesis and management
Results from the included studies were reported separately according to the Interventions, controls, and reported outcomes. No imputation of missing data was carried out and as all outcomes were reported, authors were not contacted for these. Although a meta-analysis of outcomes across studies was anticipated, the included studies had different designs and reported outcomes differently. Hence, individual study results could not be pooled in a meta-analysis.
RESULTS
Results of the search are indicated in the PRISMA flow chart (Figure 1). One hundred and fifty nine records were generated: 157 records from online search engines and two records found later on reference lists from included full-texts. A total of 56 duplicate records were removed, leaving 103 records which were assessed for eligibility. After reading titles and abstracts, a further 79 records were excluded. Full texts of the remaining 24 records were retrieved. A total of 10 articles, reporting results of 9 studies, were used for this review. There were no deviations from the protocol during the search.
The nine studies were placed in three different groups according to NZ methodology. In Group 1, NZDs were made using a NZ Impression including piezographically shaping offlanges. In Group 2, NZDs were made without piezographically shaping of flanges. Group 3 included methods of Groups 1 and 2. Because of the different NZ techniques followed for these studies, it was decided not to combine results from studies in different groups.
There were seven studies in Group 1, reporting on a total of 137 patients.7-14 Their follow-up periods were 1,2,4,8 (x2) weeks. Two studies did not report a follow-up period. Two studies reported on OHRQoL using two different versions of the OHIP, with conflicting results.12, 14 Geerts (2017) (OHIP-20, n=37) reported no significant difference in OHIP-scores between NZD and CD, while Rehmann et al. (2016) (G-OHIP-14, n=21) found significant differences.12, 14 Three studies (total n=71) reported on patient preference.8, 13 A total of 49 preferred NZDs, eight preferred CDs and 14 had no preference. Only one study had results statistically analyzed and found no significant difference in preference.13 This study was also the largest with the longest follow-up period (at least eight weeks as compared with two weeks and unknown). One study reported on satisfaction (n=10) with a significantly higher satisfaction for NZDs.11 Of the studies that reported on stability (total n=66), 50 out of 56 patients reported improvement for NZDs,7,10,12 and one study (n=10) reported a significant improvement for NZDs.11 Only one study (n=10) reported a statistically improved patient-reported retention, chewing, satisfaction, comfort, speech for NZDs.11 Walsh (1976) (n=30) reported that nine patients needed recalls for NZDs, as compared with 21 for CDs.7
Group 2 had one study, reporting on 128 patients, with a follow-up period of 40 days.15 "Number of recalls" was used as a measurement for patient satisfaction. This study reported statistically less recalls for NZDs for patients who were edentulous for longer than two years.
Group 3 also had one study, reporting on five patients, followed-up over five days, who all preferred manually formed flanges as compared with piezographically shaped flanges.16
For Group 1, lengths of follow-up periods were 1,2,4,8 (x2) weeks. Two studies did not report a follow-up period. For Groups 2 and 3, follow-up periods were 51/έ weeks and five days respectively.
In Group 1, there were four prospective single-cohort studies where PBOs of existing dentures were compared with the new NZDs.7,11'10,12 One study was prospective with two cohorts, receiving either a new CD or NZD.9 There were two cross-over trials with all patients receiving both new CDs and NZDs.8, 13,14 Four of the seven studies did not report statistical analysis.7-10
There was one study in Group 2, with cohorts receiving either a NZDs or CD.15 These two cohorts were further divided into "period of edentulousness < or > than two yrs".
The study in Group 3 was a cross-over with all patients being tested with both the manually formed and physiologically formed flanges.16
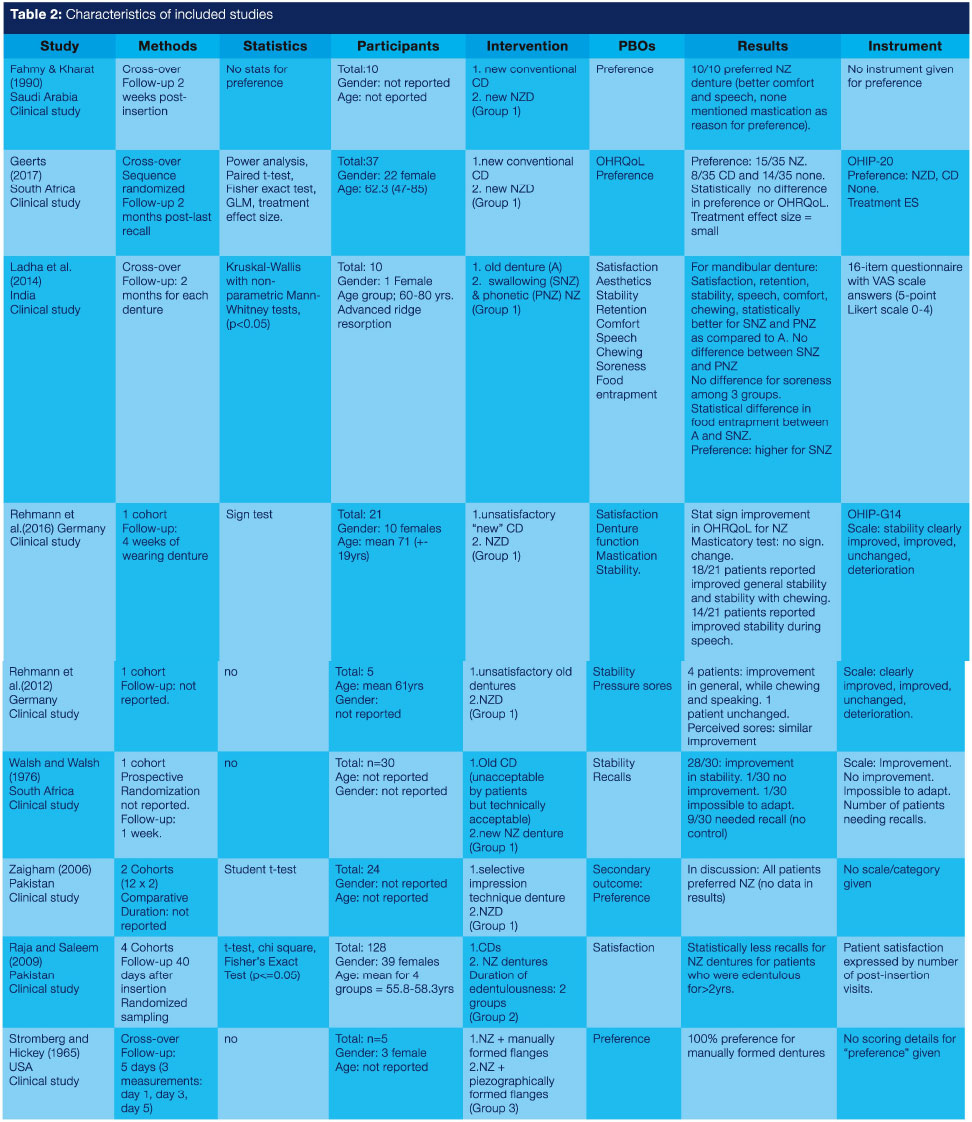
The study characteristics of all included studies are summarized in Table 2. It must be noted that, regarding outcomes, only PBOs were extracted. Some studies also reported on clinician-based outcomes, but these outcomes are not reported since they fell outside the scope of the review. Excluded studies are recorded in Table 3, together with reasons for exclusion.
For each included study, RoB was assessed as being 'low', 'high' or 'unclear' following Cochrane guidelines.5,6 Results are shown in a RoB graph and RoB summary (Figures 2 and 3). A detailed explanation of the results is as follows:
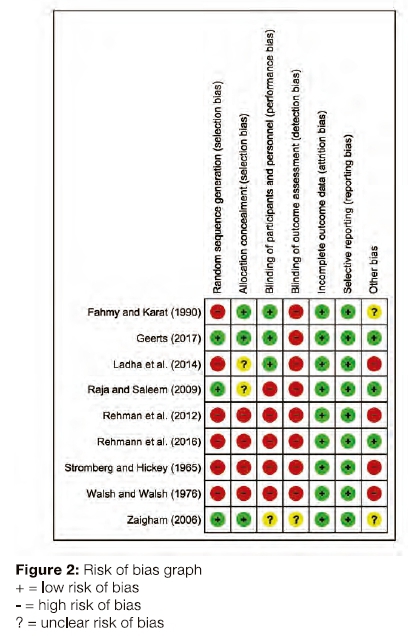

ALLOCATION (SELECTION BIAS)
Three of the nine studies were reported as randomized.7,13-15 For sequence generation: Three out of nine studies used some sequence to include patients into the study (Figures 2 and 3). One study drew lots, one used random tables and another used computer generated numbers. Where participants were asked to join the study or were included on the basis of their experiencing problems with old dentures, these were recorded as studies with a high risk of bias. Three of the studies used an allocation technique (directing the patient to a specific treatment group) eliminating selection bias. In two of the studies, allocation was unclear.9,11,16
BLINDING (PERFORMANCE BIAS AND DETECTION BIAS)
Blinding of either participants and/ or personnel was ensured in three of the nine studies (Figures 2, 3). Blinding of participants only may thus be considered as in a single-blinded cross-over clinical trial.8,11,13,14 But this process was unclear in one of the studies.9 For all the included studies, the outcomes assessors were not blinded and these were all judged as having a high risk of bias.
INCOMPLETE OUTCOME DATA (ATTRITION BIAS)
All studies did not report the analysis to be completed by the "intention-to-treat" principle, nor did any of the studies lose any patients, thus results were not negatively affected. Moreover, all pre-specified outcomes (even though these were not pre-specified as primary or secondary outcomes) were reported, thus all the studies were judged to have a low risk of bias as there was no missing data (Figures 2 and 3).
SELECTIVE REPORTING (REPORTING BIAS)
All included studies pre-specified and reported all outcomes; but only the Geerts (2017) study pre-specified these as primary and secondary outcomes.13,14 Most of the studies were not registered or approved by a review board, but because these studies reported all the outcomes as specified in the protocol, these were still judged as having a low risk of bias.
OTHER POTENTIAL SOURCES OF BIAS
Studies were judged as having a low risk of bias if there were no reason to suggest any other potential sources of bias.12-15 Four other studies were judged as having a high risk of bias due to the poor design, small sample sizes, no blinding and/or no randomization and because no ethical approval was obtained.
DISCUSSION
This SR was developed to answer the question: "In edentulous adult patients, what is the effect of NZDs on OHRQoL, patient satisfaction, and preference as compared with that of conventional mandibular CDs?" Following the search strategy, nine studies were included in an effort to answer the question. The nine studies showed high levels of heterogeneity in terms of study design, sample (size, gender), type of PBOs, instruments used to measure PBOs and RoB. Therefore, the answer to the question is: There exists no strong evidence on the beneficial effects of NZDs over conventional CDs when analyzing PBOs.
The nine selected studies were placed in one of three groups according to NZ technique used. In Group 1, four of the seven studies reported frequencies and/or ratios which were not statistically analyzed.7-10 Three studies did a statistical analysis of some PBOs but used different instruments to measure these.11-14 Only two studies used validated instruments for measuring OHRQol, but reached conflicting results, with Geerts (2017)14 reporting no difference in OHRQoL between NZDs and CDs, while Rehmann et al. (2016)12 did identify differences.12-14 The reason might be that the study design differed, with Geerts (2017)14 being a prospective cross-over study, while the Rehmann et al. (2016)12 study was a cohort study with the new NZD being compared with the patients' existing dentures, made outside trial conditions. In the Ladha et al. (2014)11 study, the main focus was comparing PBOs using a 16-item questionnaire using a 5-point Likert scale.11 This questionnaire was not provided. Hence, validity and reliability of the data could not be determined. Two different methods of making NZDs (swallowing and phonetics) performed statistically better than the CDS in satisfaction, retention, stability, comfort, speech and chewing hard food. However, they were compared with the patients existing dentures that were made outside the confines of the trial. Hence, for both the Ladha et al. (2014)11 and Rehmann et al. (2016)12 studies, the fact that existing dentures were used as control may have caused bias towards a positive outcome for the NZDs. It has been reported that simply making new dentures already improves OHRQoL, regardless of technique used.31 Another prospective single cohort study in Group 1 using the existing denture was by Walsh and Walsh (1976).7 The same argument can be used here to explain bias towards the positive results for NZDs as compared with CDs.
One study in Group 1 was prospective, using two cohorts, one receiving new CDs and one receiving new NZDs, but there was no other information on PBOs other than that all patients who received the NZDs preferred it (to the old dentures).9
Groups 2 and 3 each had one study. The study in Group 2 was a prospective cohort with all patients receiving both a CD and NZD. However, the only PBO reported on was the number of recalls as a measure for satisfaction.15 The study in Group 3 was a cross-over study, but compared functionally shaped with manually shaped flanges.16 No literature could be found confirming a positive cause-effect relationship between number of recalls and patient satisfaction. The authors did not have a conventional denture as control - both dentures were NZ dentures. However, It was decided to include this study in the review for the following reason: Piezographically contoured flanges is one of the variables of the other two groups. This study showed that piezographically developed flanges did not influence retention as compared with manually shaped flanges, while all patients preferred the manually shaped flanges. This could be clinically relevant and should be Investigated further because not having to dynamically shape flanges as part of the NZ procedures reduces clinical chair time.
Quality of the evidence of the research is dependent on several factors. By completing a RoB assessment, quality is evaluated and addressed. The quality of the evidence is an indication of the Integrity of the study. The ethics in conducting a clinical study encompasses several aspects too, but the details of design and conducting the study and obtaining the expected data is equally Important. It has been reported that developing a protocol and registering it with an Ethics review board or in trial registries and even publishing it, ensures rigor.5 The quality of the study is determined by the study design; and details must be such that results may be generalizable to larger populations. Randomized controlled trials and cross-over trials are of higher quality than cross-sectional and cohort studies. But if an RCT does not have all the steps such as 'sequence generation,' 'blinding' or 'allocation concealment' these maybe downgraded and considered of poorer quality. The results may not be considered reliable and valid. Most of the included studies followed some guidelines to protect against bias even though all the details were not reported. These were judged by using the Cochrane's RoB tool.5 For example, completing power calculation to estimate sample size will reduce RoB. Sample sizes of the included studies ranged from five to 128, but only one study reported a power calculation.13,14
The use of different study designs, methodologies, validated and unvalidated instruments and "results" not supported by data, prevented comparisons and the completion of meta-analysis among the studies. For example, Raja (2009) and Zaigham (2006) used subjective grading systems, also lacking calibration and reliability.9,15
CONCLUSION
The nine studies incorporated in this SR showed a high level of heterogeneity in terms of study design, types of PBOs and Instruments used to measure these PBOs.
The quality of the majority of clinical studies was low, with small sample sizes, short follow-up periods and presence of high level of selection, performance and detection bias.
Little high-level scientific evidence exists on the benefit of dynamic over static methods to determine mandibular CD form and shape.
Declaration
The authors received no funding for this research. The authors declare no conflict of interest.
ACRONYMS:
CD: complete dentures
NZ: neutral zone method
OHRQoL: oral health-related quality of life
PBOs: patient-based outcomes
RoBm: risk of bias
References
1. Emami E, Heydecke G, Rompré PH, de Grandmont Ρ, Feine JS. Impact of implant support for mandibular dentures on satisfaction, oral and general health-related quality of life: a meta-analysis of randomized-controlled trials. Clin Oral Implants Res 2009; 20: 533-44. [ Links ]
2. American College of Prosthodontists. Glossary of prosthodontic terms. J Prosthet Dent 2005; 94: 10-92. [ Links ]
3. Lott F, Levin B. Flange technique: an anatomic and physiologic approach to increased retention, function, comfort and appearance of dentures. J Prosthet Dent 1966; 16: 394-413. [ Links ]
4. Owen CP. Guidelines for a minimum acceptable protocol for the construction of complete dentures. Int J Prosthodont 2006; 19: 46774. [ Links ]
5. Higgins and Green. Cochrane Handbook for Systematic Reviews of Interventions. 2009. John Wiley & Sons Ltd. [ Links ]
6. Cochrane Community. Review manager. http://community.cochrane.org/editorial-and-publishing-policy-resource/information-technology/review-manager. [ Links ]
7. Walsh JF, Walsh T. Muscle-formed complete mandibular dentures. J Prosthet Dent 1976; 35: 254-8. [ Links ]
8. Fahmy FM, Kharat DU. A study of the importance of the neutral zone in complete dentures. J Prosthet Dent 1990; 64: 459-62. [ Links ]
9. Zaigham AM. A comparative study of selective pressure impression technique and neutral zone approach in atrophic mandibular ridges. Pakistan Oral & Dental Jnl. 2006; 26: 247-50. [ Links ]
10. Rehmann P, Zenginel M, Wöstmann Β. Alternative procedure to improve the stability of mandibular complete dentures: a modified neutral zone technique. Int J Prosthodont 2012; 25: 506-8. [ Links ]
11. Ladha K, Gupta R, Gill S, Verma M. Patient satisfaction with complete dentures fabricated using two neutral zone techniques: a within-subject cross-over pilot study. J Indian Prosthodont Soc 2014; 14: 161-8. [ Links ]
12. Rehmann P, Künkel AK, Weber D, Lotzmann U, Wöstmann Β. Using a modified neutral zone technique to improve the stability of mandibular complete dentures: a prospective clinical study. Int J Prosthodont. 2016; 29: 570-2. [ Links ]
13. Geerts GA. A randomized crossover trial comparing patient preference for mandibular complete dentures made with two different techniques: a short-term follow-up. Int J Prosthodont 2017; 30: 334-40. [ Links ]
14. Geerts GAVM. Neutral zone or conventional mandibular complete dentures: a randomised crossover trial comparing oral health-related quality of life. J Oral Rehabil 2017; 44: 702-8. [ Links ]
15. Raja HZ, Saleem MN. Neutral zone dentures versus conventional dentures in diverse edentulous periods. Biomedica 2009; 25: 136-45. [ Links ]
16. Stromberg WR, Hickey JC. Comparison of physiologically and manually formed denture bases. J Prosthet Dent 1965; 15: 213-30. [ Links ]
17. Pilon JF, Olthof A, van de Poel AC. Het vervaardigen van een onderprothese naar de vorm van de neutral ruimte in de edentate mond. Ned TIjdschrTandheelkd 1985; 92: 479-82. [ Links ]
18. Barrenas L, Odman P. Myodynamic and conventional construction of complete dentures: a comparative study of comfort and function. J Oral Rehabil 1989;16: 457-65. [ Links ]
19. Miller WP, Monteith B, Heath MR. The effect of variation of the lingual shape of mandibular complete dentures on lingual resistance to lifting forces. Gerodontology 1998; 15: 113-9. [ Links ]
20. Makzoumé JE. Morphologic comparison of two neutral zone impression techniques: a pilot study. J Prosthet Dent 2004; 92: 563-8. [ Links ]
21. Kursoglu P, Ari N, Calikkocaoglu S. Using tissue conditioner material In neutral zone technique. Ν Y State Dent J 2007; 73: 40-2. [ Links ]
22. Patil PG. Conventional complete denture for a left segmental mandibulectomy patient: a clinical report. J Prosthodont Res 2010; 54:192-7. [ Links ]
23. Afroz S, Rahman SA, Rajawat I, Verma AK. Neutral zone and oral submucous fibrosis. Indian J Dent Res 2012; 23: 407-10. [ Links ]
24. Astorga E, LeeX, Vergara C Reporte clínico: Registro piezográfico de la zona neutra, en un paciente con espasmos musculares involuntarios. Rev Clin Periodoncia Implantol Rehabil Oral 2013; 6: 134-7. [ Links ]
25. Tambe A, Patil SB, Bhat S, Badadare MM. Cross-arch arrangement ¡n complete denture prosthesis to manage an edentulous patient with oral submucous fibrosis and abnormal jaw relation. BMJ Case Reports 2014:bcr2013203065. doi:10.1136/bcr-2013-203065. [ Links ]
26. Comut AA, Somohano T. Surgical and prosthetic management of a complex edentulous patient for fabrication of complete dentures. Ν Y State Dent J 2015; 8: 29-33. [ Links ]
27. Mustafa AZ. Effect of the lingual ledge of neutral zone impression on the retention and stability of mandibular complete denture in elders with atrophied alveolar ridge. Tanta Dental Journal 2015; 12: 111-8. [ Links ]
28. Darwish M, Nassani MZ, Baroudi K. Effect of neutral zone technique on marginal bone loss around implant-supported overdentures. J Int Soc Prev Community Dent 2015; 5(Suppl 2): S57-62. [ Links ]
29. Porwal A, Satpathy A, Jain P, Ponnanna AA. Association of neutral zone position with age, gender, and period of edentulism. J Prosthodont 2016 Apr 6. doi: 10.1111/jopr.12485. [Epub ahead of print] PubMed PMID: 27060929. [ Links ]
30. Liu L, Ye XH, Li JY, Liao JK, Ye JT. The effect of reading aloud exercises for complete denture patients during the functional rehabilitation period. J Prosthodont 2017; 26: 201-5. [ Links ]
31. Adam RZ, Geerts GA, Lalloo R. The impact of new complete dentures on oral health-related quality of life. SADJ 2007; 62: 264-6, 268. [ Links ]
 Correspondence:
Correspondence:
Professor Greta Geerts
Tel +27 21 9373095
Email ggeerts@uwc.ac.za
Contributions
1. Greta Geerts. Conceptualization 100%, Researcher 50%, Writing 50%
2. Saadika Khan Researcher 50%, Writing 50%


{kind=link}
{kind=link}
{kind=link}