










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Dental Journal
versión On-line ISSN 0375-1562
versión impresa ISSN 0011-8516
S. Afr. dent. j. vol.73 no.4 Johannesburg may. 2018
CASE REPORT
Oral medicine case book: Oral angiomyoma
Temilola D.I; Holmes H.II; Mulder-van Staden S.III; Stephen LIV; Afrogheh A.V
IBChD, MSc. Division of Oral Medicine and Periodontics, Faculty of Dentistry, (UWC)
IIBChD, MSc, MChD. Division of Oral Medicine and Periodontics, Faculty of Dentistry, (UWC)
IIIBChD, MChD. Division of Oral Medicine and Periodontics, Faculty of Dentistry, (UWC)
IVBChD, PhD. Division of Oral Medicine and Periodontics, Faculty of Dentistry, (UWC)
VBChD, MSc, MChD, IFCAP. Division of Oral and Maxillofacial Pathology, Faculty of Dentistry, (UWC) Cape, National Health Laboratory Service, Tygerberg Hospital
Keywords: Oral Squamous Cell Carcinoma, Oral Cancer, OSCC, Epidemiology
CASE REPORT
A 50-year-old female was referred to the Oral Medicine Clinic at the University of the Western Cape, Oral Health Centre, Tygerberg campus, by her general practitioner. She presented with a three year history of a painless swelling on the inner aspect of her lower lip. The patient recalled episodes of trauma to her lower lip from a protruding upper incisor tooth. The patient had diabetes and hypertension, which were both well controlled with medications.
Intra-oral examination revealed a 2 χ 1cm non-tender, firm, dome shaped bluish swelling on the lower labial mucosa, which did not blanch on palpation (Figure 1).

A clinical diagnosis of mucocele was suspected, however, since mucoceles are seldom encountered in middle-aged patients, the differential diagnosis also included vascular (hemangioma and lymphangioma) and fluid-filled mucocele-like salivary gland tumours, such as mucoepidermoid carcinoma. An excisional biopsy was performed under local anaethesia, and the patient was prescribed 0.2% Chlorhexidine digluconate oral rinse and 500mg Paracetamol four times daily postoperatively.
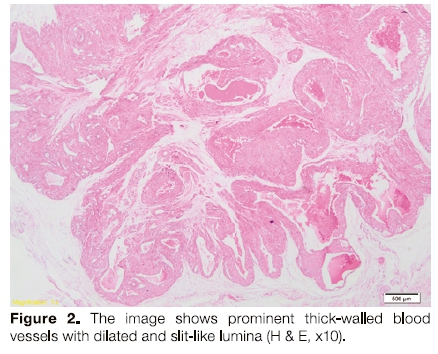
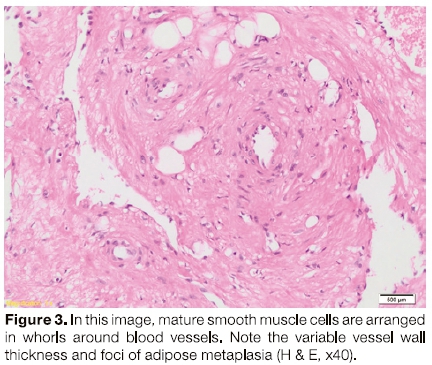
Histological examination disclosed an angiomyoma (vascular leiomyoma). The lesion consisted of prominent thick-walled blood vessels with dilated and slit-like lumina (Figure 2). Mature smooth muscle cells were arranged in bundles and whorls around blood vessels. There were also aggregates of mature adipocytes, which appeared to represent a form of degenerative metaplasia (Figure 3).
DISCUSSION
Leiomyoma is a benign smooth muscle neoplasm composed of cells displaying smooth muscle differentiation. In general, leiomyomas can be classified into cutaneous and non-cutaneous types. Cutaneous leiomyomas arise within the superficial dermis, and originate from the arrector pili muscle and are therefore termed pilar leiomyomas. Noncutaneous leiomyomas with a prominent vascular component are referred to as vascular leiomyomas or angiomyomas.1-3 Since there is little smooth muscle in the head and neck region (seen only in cervical oesophagus, circumvallate papillae and ductus lingualis of the tongue), leiomyomas are rarely reported in the head and neck region, accounting for only 0.4% of all soft tissue neoplasms and 0.06% of all leiomyomas.4,5
Angiomyoma is the most common variant of leiomyoma found in the oral cavity, nasal cavity and paranasal sinuses, representing 0.016% to 0.065% of all leiomyomas.57 These tumours may arise from the tunica media of small blood vessels.8,9
Oral angiomyomas are common in male patients,10-11 with only a few cases reported in females. The exact aetiopathogenesis is unknown, though local infection, chronic trauma, arteriovenous malformations and hormonal influences have been proposed as possible factors.12
Oral angiomyomas are well circumscribed, benign tumours which present as slow growing, dome shaped masses, commonly affecting the lower lip, tongue, cheeks, and palate.6 They are asymptomatic and may be present for months to years.
Because oral angiomyomas are highly vascular, they appear clinically as blue, fluid-filled lesions, closely resembling mucoceles. However, in an adult patient one should also consider vascular [lymphangioma, hemangioma, and pyogenic granuloma) and other salivary gland lesions (mucoepidermoid carcinoma and myxoid pleomorphic adenoma). The histologic differential diagnosis of an angiomyoma is not usually problematic but may include fibroma or schwannoma.
Imaging systems such as ultrasound and colour flow imaging have been used to determine the nature and extent of lesions.7 Histological examination of oral angiomyomas usually confirms a well circumscribed lesion, with vascular spaces of different sizes and shapes. Smooth muscle cells are arranged in disorganized bundles and whorls around the vascular spaces. In rare cases, tumours may exhibit cellularity, nuclear pleomorphism, and nuclear hyperchromasia coupled with any mitotic activity and should be considered potentially malignant.13
The treatment of choice for oral angiomyoma is conservative surgical excision. Despite the vascular origin of these lesions, excessive bleeding during surgical excision is very rare.4 Local recurrences occur in only 5% of leiomyomas, irrespective of the type.12,14 The prognosis of oral angiomyoma is excellent. Recurrence is rare and non-destructive. Any recurrences must be considered as possible "smooth muscle tumour of uncertain malignant potential.' "15Therefore, long-term follow-up after treatment is required.
CONCLUSION
Oral angioleiomyomas are rare, benign smooth muscle neoplasms. As oral angiomyomas are highly vascular, they appear clinically as blue, fluid-filled lesions, closely resembling mucoceles. However, in an adult patient, dentists should also consider vascular (lymphangioma, hemangioma, and pyogenic granuloma) and other salivary gland lesions (mucoepidermoid carcinoma and myxoid pleomorphic adenoma). The prognosis of oral angiomyoma is excellent. Recurrence is rare, but when evident the clinician should be encouraged to reconsider the lesion as a possible "smooth muscle tumour of uncertain malignant potential." Therefore long-term follow up after treatment is required.
ACRONYMS
MD: moderately differentiated
OSSC: Oral squamous cell carcinoma
PD: poorly differentiated
WD: well differentiated
References
1. Veeresh M, Sudhakara M, Girish G, Naik C. Leiomyoma: A rare tumor in the head and neck and oral cavity: Report of 3 cases with review. Journal of Oral and Maxillofacial Pathology 2013;17(2):281 [ Links ]
2. Ramesh P, Annapureddy SR, Khan F, Sutaria PD. Angioleiomyoma: a clinical, pathological and radiological review. International Journal of Clinical Practice 2004; 58(6):587-91. [ Links ]
3. Rawal SY, Rawal YB. Angioleiomyoma (Vascular Leiomyoma) of the oral cavity. Head and Neck Pathology 2017; 6:1-4. [ Links ]
4. Menditti D, Laino L, Nastri L, Caruso U, Fiore P, Baldi A. Oral angioleiomyoma: a rare pathological entity, IN VWO. 2012; 26(1):161-3. [ Links ]
5. González Sánchez MA, Colorado Bonnin M, Berini Aytés L, Gay Escoda C. Leiomyoma of the hard palate: a case report. Medicina Oral, Patología Oral y Cirugía Bucal (Internet) 2007;12(3):221-4. [ Links ]
6. Barboza CA, Ginani F, Leite-Segundo AV, Silva UH. Oral angioleiomyoma: a case report and considerations on differential diagnosis. Jornal Brasileiro de Patología e Medicina Laboratorial 2013;49(6):429-32. [ Links ]
7. Ranjan, S. and Singh, K.T., 2014. Gingival angiolelomyoma-infrequent lesion of oral cavity at a rare site. Journal of Oral and Maxillofacial Pathology 2014;18(1) :107-11. [ Links ]
8. ArpaHOF, Damlar I, Kilç S, Altan A, TaHZA, Özgür T. Angioleiomyoma of the gingiva: a report of two cases. Journal of the Korean Association of Oral and Maxillofacial Surgeons 2016; 42(2):115-9. [ Links ]
9. Mahlma VG, Patil K, Srlkanth HS. Recurrent oral angioleiomyoma. Contemporary Clinical Dentistry 2011:2(2):102-5. [ Links ]
10. Tsuji T, Satoh K, Nakano H, Kogo M. Clinical characteristics of angioleiomyoma of the hard palate: report of a case and an analysis of the reported cases. Journal of Oral and Maxillofacial Surgery 2014 ;72(5):920-6. [ Links ]
11. Bey KA, Alroyayamina S, Golding SJ, Tiam RN, Watt-Smith SR. Angioleiomyoma of the hard palate: report of a case and review of the literature and magnetic resonance imaging findings of this rare entity. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology. 2012;114(2):e45-9. [ Links ]
12. Hung KF, Yan AH, Kao SY, Chang CS. Angioleiomyoma in right lingual gingiva. Chin J Oral Maxillofac Surg. 2005 ;16:179-87. [ Links ]
13. Brooks JK, Nikitakis NG, Goodman NJ, Levy BA. Clinicopathologic characterization of oral angioleiomyomas. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics 2002;94(2):221 -7. [ Links ]
14. Inaba H, Ohnishi Y, Inaba M, Niki H, Yamasaki Y, Morita S, Kakudo K. Painless mass of the cheek. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics. 2003;95(1):3-6. [ Links ]
15. Ishikawa S, Fuyama S, Kobayashi T, Taira Y, Sugano A, lino M. Angioleiomyoma of the tongue: a case report and review of the literature. Odontology 2016;104(1):119-22. [ Links ]
 Correspondence:
Correspondence:
Dr. Haly Holmes
Division of Oral Medicine and Periodontology, (UWC) Dental Faculty
Francie Van Zyl Drive, Tygerberg Campus
Tel: 27 21 937 3102
Email: hholmes@uwc.ac.za

