










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Dental Journal
versión On-line ISSN 0375-1562
versión impresa ISSN 0011-8516
S. Afr. dent. j. vol.73 no.4 Johannesburg may. 2018
RESEARCH
An in-vitro comparative micro-computed tomographic evaluation of three obturation systems
Kabini SNI; Moodley DSII; Parker MEIII; Patel NIV
IDepartment of Prosthodontics Faculty of Dentistry, Sefeko Makgatho Health Science University, South Africa
IIPhD, Department of Restorative Dentistry, Faculty of Dentistry, University of the Western Cape, Cape Town, South Africa
IIIMChD, Department of Restorative Dentistry, Faculty of Dentistry, University of the Western Cape, Cape Town, South Africa
IVMChD, Department of Restorative Dentistry, Faculty of Dentistry, University of the Western Cape, Cape Town, South Africa
ABSTRACT
Adaptation of obturation material to dentine walls is essential for the success of root canal treatment.
AIM: To evaluate and compare the adaptation of gutta-percha of three obturation systems, using micro-computed tomography.
METHODS: The roots of 90 central incisors were shaped with ProTaper Universal (Dentsply) files, irrigated with 1ml 5.25% sodium hypochlorite and flushed with 5ml 17% EDTA. The roots were randomly divided into: Group 1: GuttaCore obturation, Group 2: ProTaper single-cone obturation, Group 3: Thermafil obturation. All canals were sealed with AH Plus (Dentsply). A v|tome|x 240D micro-CT scanner was used to scan each root at 15μιτι resolution. The size of voids and gaps observed at 1mm, 3mm and 6mm axial sections from the apex were compared, as was the volume of cement around the gutta-percha.
RESULTS: Group 2 (Protaper) had statistically significantly greater incidence of voids and of surrounding cement than either Thermafil or GuttaCore carrier based systems (Kruskal-Wallis p<0.001).
CONCLUSION: Both carrier-based techniques allowed for better sealing ability in root canals compared with single-cone gutta-percha obturation although none of the materials were gap free, especially at 1mm from apex.
CLINICAL SIGNIFICANCE: Both carrier-based techniques show good sealing ability and are appropriate for daily endodontic practice.
Keywords: Endodontics, Obturation, Gutta-percha, Cold condensation, Carrier-based obturation, Thermafil, ProTaper, GuttaCore
INTRODUCTION
Endodontic materials are developing at a rapid rate with each manufacturer claiming their products are superior. The ultimate aim of a root filling is to fill the entire prepared and cleaned root canal.1 The success of root canal obturation does not only depend on the root canal sealer, but also on proper compression of the gutta-percha against the walls of the root canal. A hermitic seal can be obtained by good root canal obturation and sealing of lateral and accessory canals as well. Therefore, close conformation of the root canal filling material to the dentinal walls is essential for the success of root canal therapy as this prevents the formation of gaps or voids between the root filling material and the root canal walls. This will ensure the sealing of all the lateral and accessory canals that are frequently found on the root canal walls. Furthermore, dissolution of root canal sealer at the apex of the tooth may be counteracted by properly filled and well compressed gutta-percha to prevent microbial infection due to leakages.
The formation of a gap between root canal walls and the root canal filling material may allow re-infection of the root canal system, leading to treatment failures. Efficient sealing of the canals is essential in the prevention of colonization by micro-organisms within the root canal system.2
The techniques commonly employed for endodontic root canal obturation include cold lateral compaction, warm vertical compaction and core-carrier techniques. These core-carrier systems are claimed by the manufacturers to enhance intimate compression of the gutta-percha against the canal wall, and the flow of the filling material into the lateral canals. The original carrier was made of metal. Due to the difficulties encountered in retreatment and in the preparation of post spaces, the original metal carriers were subsequently replaced by plastic obturators.3 Recently, a new core-carrier system, GuttaCore (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA) was introduced in which the Vectra (a liquid crystal polymer) or polysulphone plastic carriers in Thermafil Plus (Dentsply Tulsa Dental Specialties), were replaced by cross-linked thermoset gutta-percha, which enables the carrier (obturator) to be removed more easily during retreatment.3 The GuttaCore does not melt when placed in an obturator oven but softens.4 The core-carrier obturation technique has been regarded by some as the only genuine warm gutta-percha technique for complete filling of the apical third of the canal space. However, the quality of root canal obturation achieved by the new core-carrier system that incorporates cross-linked thermoset gutta-percha carriers has not been reported.3
Thus, the objective of the present in-vitro study was to use micro-computed tomography (micro-CT) to examine the quality of obturation in single-rooted canals obturated with the GuttaCore core-carrier system and to compare the results between similar canals obturated with the ProTaper single-cone obturation technique and with another core-carrier technique, Thermafil. The null hypothesis stated that there are no differences in the percentage of interfacial voids amongst the three obturation techniques.
MATERIALS AND METHODS
A total of ninety extracted permanent human central incisor teeth were used in this study. Roots with a curvature of less than 10 degrees were selected. Previously root canal treated teeth, teeth with root caries or root fractures, teeth with immature apices or root resorption were excluded from the study. Those teeth with canal sizes larger than the size F3 file were also excluded from the study.
Tooth preparation
To standardize root canal dimensions, the teeth were decoronated with a Diamond Cut-off wheel (Struers, Denmark) to achieve a length of 15mm. Access into the canal was created and a size 10 hand file (K-file, Dentsply, Tulsa Dental, Tulsa, USA) was used to establish patency. The working length was calculated and set at 1mm short of the apex. A glide path was established by initially filing with number 10 and number 15 files (K-file, Dentsply, Tulsa Dental, Tulsa, USA) for all the roots.59 The ProTaper (Dentsply Tulsa Dental, USA) files were used to clean and shape the root canal up to the master file.10 Rotary files (ProTaper Universal) were used with a hand-piece attached to a speed and torque controlled motor (X-Smart, Dentsply-Maillefer) set at 300 rpm. The sequence used was ProTaper S1, S2, F1, F2, and F3 as per manufacturer's Instructions. During preparation and between each file, 1ml of 5.25% sodium hypochlorite was used as an irrigant to debride the canal.11 After completion of instrumentation, all specimens were flushed with 5ml of 17% ethylene-diamine-tetra-acetic acid (EDTA) and a final drench with sodium hypochlorite to rinse off the EDTA from the root canal walls and remove the smear layer.12 All the canals were dried with paper points and were readied for obturation. The roots in all the three groups were treated by a single operator and all files were replaced after five uses.
Root canal obturation
The roots were randomly divided into three groups of thirty each and each group was obturated with a different obturation technique (n=30). The roots in Group 1 were obturated with GuttaCore, Group 2 with ProTaper single-cone and Group 3 with Thermafil. AH Plus root canal sealer (Dentsply Tulsa Dental, Tulsa, USA) was used for sealing all canals. All roots were stored at a temperature of 37°C and at 100% relative humidity in an incubator for a period of 24 hours to allow complete setting of root canal sealers.
Micro-CT Imaging
A high-resolution micro-CT scanner model A v|tome|x 240D (General Electric, MA, USA) was used to scan the teeth. Each root was positioned on the specimen stage and scanned with a very high Isotropic resolution of 15μιτι, rotational step of 0.6° and a rotational angle of 360°. With a fully automated CT scan reconstruction and analysis process (datos|x 2.0 software) with high precision and reproducible 3D metrology, images obtained from the scan were reconstructed to show two-dimensional slices of the inner structure of the roots. Accelerated 3D CT reconstruction technique by velo| CT software was invoked for volume visualization in 3D rendered mode analysis, for measurements of the volume of the root canal filling material and calculation of the percentage of gaps and voids present in the material. Axial sections at 1mm, 3mm, and 6mm from apex were made and two different parameters were derived: The ratio between the total area of voids/gaps in square micrometers and the total canal area in the section were calculated. In 3D surface-rendered reconstructions, the ratio between the volume of voids/gaps in cubic micrometers, and the total canal volume were calculated.
Statistical Analysis
Since the datasets from the parameters were not normally distributed even after data transformation, each dataset was analysed using the non-parametric test: Kruskal-Wallis analysis of variance. Statistical significance was pre-set at alpha = 0.05 for all analyses to explore for any significant differences between GuttaCore, ProTaper and Thermafil. The following outcome measures were assessed:
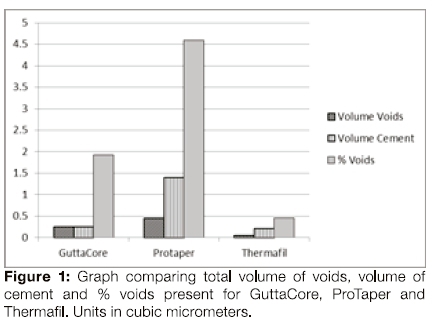
1. Total volume of voids between gutta-percha and the root canal walls
2. Total volume of cement within the canal space
3. Percentage of volume of voids to the total volume of canal space on 3D surface rendered reconstructions within the entire root canal space following obturation
4. The presence or absence of voids/gaps between the gutta-percha/cement and dentine interface on axial sections at 1mm, 3mm, and 6mm from the apex coronally.
RESULTS
The mean volume of voids for ProTaper single cone obturation (Figure 1) was found to be greater than that of Thermafil and GuttaCore, the statistical significance of the differences being confirmed by a Kruskal-Wallis test, p-value <0.001. The mean and median of Protaper were greater than those of Thermafil and GuttaCore, the differences again confirmed as statistically significant (p-value <0.001).
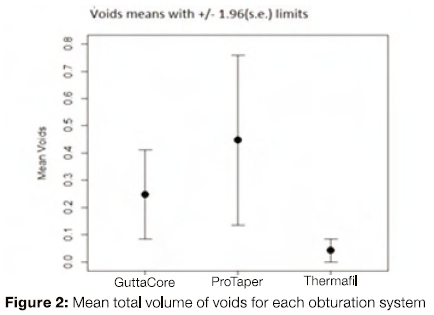
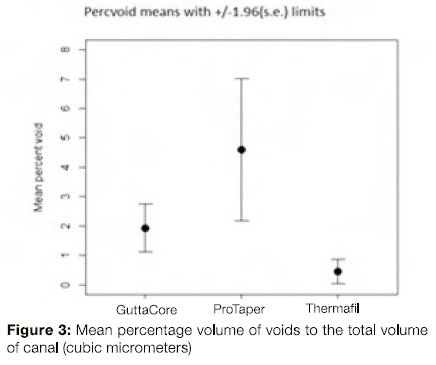
The mean and median of the Protaper data were greater than those of Thermafil and GuttaCore (Figures 2 and 3); the statistical significance of the differences confirmed by a Kruskal=Wallis test. ( Kruskal-Wallis chi-squared = 32.551, df = 2, p-value <0.001.)
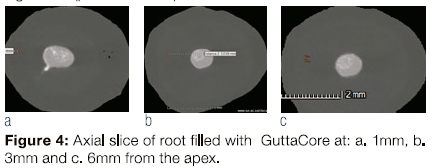
GuttaCore demonstrated good sealing of the root canal and there was also sealing of the lateral canals at 1mm from the apex (Figure 4). There was also little root canal sealer between the wall and GuttaCore at 1mm, 3mm and 6mm from the apex indicating good compression of GuttaCore against the inner walls of the root canal.
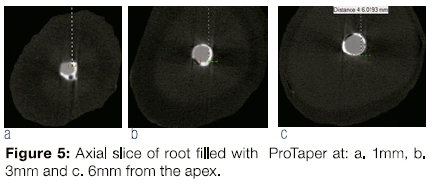
Voids (translucent areas seen in micro-CT images) were present in ProTaper single cone obturation at 1mm, 3mm and 6mm from the apex of the tooth (Figure 5). There was also a higher volume of cement in all the three sections of the slices (white areas in micro-CT images). The large cement volume and the abundance of voids with ProTaper single-cone obturation demonstrated poor sealing of the root canal.
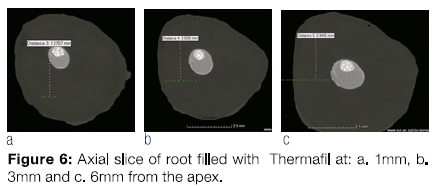
Thermafil achieved good sealing of the ovoid root canals (Figure 6). There was also little root canal sealer on the section of Thermafil at 1mm, 3mm and 6mm from the apex indicating good compression of Thermafil against the inner walls of the root canal.
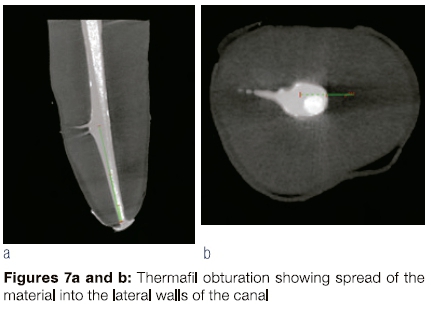
Thermafil not only showed good adaptability to the walls of the canal but was able to fill the lateral walls (Figures 7a and 7b).
DISCUSSION
The quality of obturation can be assessed through laboratory studies. Several in vitro techniques were developed to determine the sealing ability of root fillings: dye penetration, fluid transport, and scanning electron microscopy analyses. All have limitations of measuring voids by analysis of sectioned roots. In the past various types of dyes like eosin, methylene blue; black Indian ink and Procion brilliant blue were used to evaluate adaptation and micro-leakage of the gutta-percha.13 Microscopy can be used at various magnifications to determine adaptation of gutta-percha to the walls of the root canal. It is one of the oldest methods used to evaluate gutta-percha leakage and adaptation but sample preparations are technique sensitive and may be damaged during the process.14
Micro-computed tomography (micro-CT) has been described as a new and promising tool in endodontics to assess the geometry of the root canal.1,15,16 High resolution micro-CT is an emerging technology with several promising application in different fields of dentistry. It is highly accurate and non-destructive method for in-vitro evaluation of root canal fillings.2 However, micro-CT sections lack the resolution when compared with scanning electron microscopy (SEM), for the use of studying inter-facial gaps and Intra-canal voids. SEM however, is a more destructive method of Investigation and is labour intensive.3
Micro-CTprovidesathree dimensional view of the root canal system by providing an undistorted image of the tooth. It has the highest resolution at a very low exposure compared to a conventional CT scan. The micro-CT can be a useful tool to check for gap formation between the root canal filling and the dentine walls because it is a less complicated technique compared to conventional methods, specimens are not damaged and images can be viewed in three dimensions. Micro-CT imaging tool overcomes the limitations of the previously used model like dye penetration, fluid transport, and cross-sectional analyses, which are valuable techniques, but the results do not always corroborate with each other.2 Therefore In this study, micro-CT was used as an imaging tool of choice based on its advantages that are demonstrated by the literature. In clinical situations, radiographs are frequently used to analyse root canal treatment. Intra-oral radiographs are widely used to evaluate adaptation of obturation materials but have the disadvantage of showing a two dimensional view of the image.
Under the conditions of the present study, all three obturation systems exhibited void formation when observed using the micro-CT scanned images set at 15μιτι resolution. As there were significant differences in the percentages of void formation between the systems tested when obturated with the GuttaCore carrier technique, ProTaper single-cone technique and Thermafil carrier technique, the null hypothesis had to be rejected.
Thermafil produced superior obturation when compared with ProTaper single-cone gutta-percha and GuttaCore, and one demonstrated the best compression when compared with GuttaCore and ProTaper gutta-percha. When the volumes of voids were evaluated, Thermafil data were significantly lower than GuttaCore and ProTaper (Kruskal-Wallis analysis of variance p<0.001). This indicated good material adaptation for specimens obturated with Thermafil. When the percentages of the volumes of voids to the canal volumes were compared, ProTaper guttapercha recorded a higher percentage when compared with Thermafil and GuttaCore (p<0.001). The review of the literature has shown superior obturation with thermal obturation compared with lateral condensation both in the presence or absence of smear layer.17 The current study was conducted in the absence of smear layer, removed from all the root canal walls using EDTA.
Apical leakage is one of the more common complications encountered in endodontic failures. AH Plus root canal sealer was used to apically seal off all the roots in the three groups. It Is classified as a resin bonded sealer and uses methamine for polymerization. The presence of large amount of root canal sealer usually leads to root canal failure due to the dissolution of the root canal sealer by cellular fluids. The sealer coverage is influenced by the closeness of the adaptation of the gutta-percha to the walls of the root canal.18
In the current study the quantity of sealer coverage was found to be reduced apically with Thermafil and GuttaCore obturations, Indicating a good fit of the two carrier systems to the walls of the root canal. There was more sealer material apically with ProTaper single-cone gutta-percha, and indeed a significantly higher volume of cement in teeth obturated with this material, (Kruskal-Wallis, p<0.001) indicating poor sealing of the root canal. This may also account for the presence of a greater number and volume of voids found with single-cone ProTaper obturation. When there is poor adaptation of the gutta-percha to the root canal walls, the resulting gap is usually occupied by a large amount of root canal sealer;
This study assessed the critical area of the root canal, the apical third. Proper obturation of this area is crucial as most canal aberrations like apical deltas and lateral canals are located there, making proper obturation difficult.
Thermafil produced the best adaptation, followed by GuttaCore and then ProTaper gutta-percha as indicated by the reduced amount of cement around the gutta-percha in all three axial sections namely at 1mm, 3mm and 6mm. Carrier-based root fillings, in particular, have a mean sealer thickness of 2μιτι, considerably less than the 7μιτι resolution capability of the micro-CT scanner.2 This may explain why in the majority of Thermafil obturators, fillings sealer was indistinguishable from gutta-percha.
GuttaCore was introduced into the market as cross-linked gutta-percha which has the advantage of easier removal in the root canals for post placement and during retreatment.19 Since GuttaCore is a fairly new product in the market, only a few studies have evaluated its adaptation to the root canal wall and its ability to seal all canal abberations. GuttaCore produced superior obturation when compared with ProTaper single-cone gutta-percha but its performance was not superior to Thermafil obturations. Although the mean volume of cement for GuttaCore and Thermafil showed better results, canals obturated with GuttaCore exhibited more voids when compared with those filled with Thermafil. The disadvantage of presently available carrier-based obturation systems is that the volume of gutta-percha is not consistently distributed around the carrier. This might allow shedding of the gutta-percha from the carrier material when the obturator is inserted into the root canal space, possibly leading to voids.21 Frictional forces may generate an extrusion effect, whereby the filling material is retained at the orifice of the canal.22 This might possibly account for the presence of voids in GuttaCore obturation when compared with Thermafil obturation, but more studies are needed to verify this.
According to the literature, gutta-percha for dental use exists mostly in Η-phase crystalline form even though some companies claim to manufacture Η-phase gutta-percha.20 When gutta-percha Is heated, between the temperatures of 42°C and 49°C, the crystalline B-phase gutta-percha is converted to the crystalline B-phase gutta-percha.20 Both Thermafil and GuttaCore materials are covered with alpha-phase gutta-percha. This B-phase guttapercha becomes "gluey", adhesive and highly flowable when heated (low viscosity) accounting for its enhanced adaptation to the root canal walls compared with beta-phase gutta-percha which has a higher viscosity. This lack of flow ability may account for the poor adaptability of single cone cold condensation technique as seen in this study. The alpha-phase gutta-percha present in both Thermafil and GuttaCore when heated increases its viscosity and thus its plasticity thereby allowing for better compaction against the canals walls.
The results of this study show a high variation in the data especially for the cold condensation ProTaper single-cone obturation technique. This is an indirect indicator of the unpredictability of commonly used obturation techniques in perfectly adapting to the canal walls and root filling materials.3 A similar conclusion was reached in a stereomicroscopy study undertaken to examine voids present in central incisors that were obturated with cold lateral compaction.23
The warm obturation system produced better results in the sealing of lateral and accessory canals in this and in previous studies.24 The literature has also demonstrated that Thermafil produced good adaptation to the walls of the canals when compared with lateral compaction and single-cone obturation.25
CONCLUSION
Within the limitations of the present study, both carrier based techniques showed good sealing ability in root canals compared with the single cold gutta percha obturation technique although none of the materials was gap-free especially at 1mm from apex. This study shows the efficiency of carrier-based obturation systems in filling root canals hermetically compared with the cold condensation technique of ProTaper obturation. Thermafil produced good adaptation to canal walls with least amount of voids/gap formation, followed by GuttaCore and the ProTaper cold gutta-percha condensation.
Clinical Significance
This study showed the efficiency of carrier-based obturation systems in filling root canals hermetically when compared with the traditional standard cold gutta-percha obturation technique with lateral condensation. The results show good sealing ability of both carrier- based techniques making them appropriate for use in daily endodontic practice.
References
1. Hammad M, Qualtrough A, Silikas N. Evaluation of root canal obturation: A throe-dimensional in vitro study. Journal of Endodontics. 2009;35(4):541-4. [ Links ]
2. Zogheib C, Naaman A, Sigurdsson A, Medioni E, Bourbouze G, Arbab-Chirani R. Comparative micro-computed tomographic evaluation of two carrier-based obturation systems. Clinical Oral Investigations. 2013:17(8):1879-83. [ Links ]
3. Li G-h, Niu L-n, Selem LC, Eid AA, Bergeron BE, Chen J-h, et al. Quality of obturation achieved by an endodontic core-carrier system with crosslinked gutta-percha carrier in single-rooted canals. Journal of Dentistry. 2014;42(9):1124-34. [ Links ]
4. Gutmann JL. The future of root canal obturation. Dentistry Today. 2011;30:130-1. [ Links ]
5. Van der Vyver P, Paleker F, Jonker C. Comparison of preparation times of three different rotary glide path instrument systems. South African Dental Journal. 2015;70(4):144-7. [ Links ]
6. Gambarini G, Plotino G, Sannino G, Grande NM, Giansiracusa A, Piasecki L, et al. Cyclic fatigue of instruments for endodontic glide path. Odontology. 2015;103(1):56-60. [ Links ]
7. Cassim I, Van der Vyver PJ. The importance of glide path preparation in endodontics: A consideration of instruments and literature: South African Dental Journal. 2013;68(7):322-7. [ Links ]
8. Berutti E, Cantatore G, Castellucci A, Chiandussi G, Pera F, Migliaretti G, et al. Use of nickel-titanium rotary pathfile to create the glide path: Comparison with manual preflaring in simulated root canals. Journal of Endodontics. 2009;35(3):408-12. [ Links ]
9. Berutti E, Negro AR, Lendini Μ, Pasqualini D. Influence of manual preflaring and torque on the failure rate of protaper rotary instruments. Journal of Endodontics. 2004;30(4):228-30. [ Links ]
10. Ruddle CJ. The protaper technique. Endodontic Topics. 2005;10(1):187-90. [ Links ]
11. Palazzi F, Morra M, Mohammad! Ζ, Grandini S, Giardino L. Comparison of the surface tension of 5.25% sodium hypochlorite solution with three new sodium hypochlorite-based endodontic irrigants. International endodontic journal. 2012;45(2):129-35. [ Links ]
12. Asientas EE, Buzoglu HD, Altundasar E, Serper A. Effect of edta, sodium hypochlorite, and Chlorhexidine gluconate with or without surface modifiers on dentin microhardness. Journal of Endodontics. 2014;40(6):876-9. [ Links ]
13. Verfssimo DM, do Vale MS. Methodologies for assessment of apical and coronal leakage of endodontic filling materials: A critical review. Journal of Oral Science. 2006;48(3):93-8. [ Links ]
14. Tripi TR, Bonaccorso A, Tripi V, Condorelli GG, Rapisarda E. Defects in rotary instruments after use: An SEM study. Journal of Endodontics. 2001 ;27(12):782-5. [ Links ]
15. Peters OA, Schonenberger Κ, Laib Α. Effects of four ni-ti preparation techniques on root canal geometry assessed by micro computed tomography. International Endodontic Journal. 2001:34(3):221-30. [ Links ]
16. Peters OA, Barbakow F. Effects of irrigation on debris and smear layer on canal walls prepared by two rotary techniques: A scanning electron microscopic study. Journal of Endodontics. 2000:26(1):6-10. [ Links ]
17. Gengoglu N, Samani S, Günday Μ. Dentinal wall adaptation of thermoplastlcized gutta-percha in the absence or presence of smear layer: A scanning electron microscopic study. Journal of Endodontics. 1993:19(11):558-62. [ Links ]
18. Wu MK, Ozok A, Wesselink P. Sealer distribution in root canals obturated by three techniques. International Endodontic Journal. 2000:33(4):340-5. [ Links ]
19. Tomson R, Polycarpou N, Tomson P. Contemporary obturation of the root canal system. British Dental Journal. 2014;216(6):315. [ Links ]
20. Combe EC, Cohen BD, Cummings K. Alpha-and beta-forms of guttapercha In products for root canal filling. International Endodontic Journal. 2001 Sep 1:34(6):447-51. [ Links ]
21. Alhashlmi RA, Foxton R, Romeed S, Deb S. An in vitro assessment of gutta-percha coating of new carrier-based root canal fillings. The Scientific World Journal. 2014;2014. [ Links ]
22. Bertacci A, Baroni C, Breschi L, Venturi M, Pratl C. The influence of smear layer in lateral channels filling. Clinical Oral Investigations. 2007 :11(4):353-9. [ Links ]
23. Kececi A, Celik Ünal G, §en B. Comparison of cold lateral compaction and continuous wave of obturation techniques following manual or rotary instrumentation. International Endodontic Journal. 2005:38(6):381-8. [ Links ]
24. Robberecht L, Colard T, Claisse-Crinquette A. Qualitative evaluation of two endodontic obturation techniques: Tapered single-cone method versus warm vertical condensation and Injection system an In vitro study. Journal of Oral Science. 2012:54(1):99-104. [ Links ]
25. Lea CS, Apicella MJ, Mines P, Yancich PP, Parker MH. Comparison of the obturation density of cold lateral compaction versus warm vertical compaction using the continuous wave of condensation technique. Journal of Endodontics. 2005:31(1):37-9 [ Links ]
 Correspondence:
Correspondence:
Dr. DS Moodloy
Department of Restorative Dentistry, Faculty of Dentistry
University of the Western Cape
Private Bag X1, Tygerberg, 7505
Cape Town, South Africa.
Telephone: +27 21 9373090
Email: dmoodley@uwc.ac.za

