










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.73 n.4 Johannesburg May. 2018
RESEARCH
A comparison of the dental age estimation methods of Phillips and Proffit in a sample of South African children
Elgamri AI; Mohamed NII; Hudson AIII
IBDS (Univ of Khartoum); MFD (Royal College of Surgeons, Ireland); MSfcPaed Dent (UWC)
IISCftOfUS); BScHons(Paed Dent) (US); MSc (Paed Dent) (US); /W(Comm Health) (US)
IIIBChD(US); BScHons(US); MSt(UWC)
ABSTRACT
INTRODUCTION: Dental age is an indicator of the physiological maturity of growing children. Different methods for estimating the dental age in contrast to the chronological age have been proposed.
Aims and objectives.
The aim of this retrospective study was to compare the accuracy of the Phillips and the Proffit methods in estimating the dental age in a mixed sample of South African children.
METHODS: A random selection was completed of 100 panoramic radiographs of patients with known chronological ages, ranging between 6 and 11 years. Dental age for each radiograph was estimated using both the Phillips and the Proffit methods.
RESULTS: The Phillips method underestimated the age of combined sample by four months (statistically significant ρ =0.03), whilst the age of the boys sample was underestimated by six months (statistically significant ρ <0.0001). For the girls' sample, the Proffit method underestimated the age by only two days (not statistically significant ρ =0.97). Proffit's method underestimated the age of the boys by two months (not statistically significant (p= 0.15).
CONCLUSION: Even though it has not previously been validated, Proffit's description of dental development has been shown to be accurate in estimating the dental age.
Keywords: Dental age, Physiological age, Chronological age, Estimation, Comparison, Proffit, Phillips tables, Panoramic radiograph
INTRODUCTION AND LITERATURE REVIEW
Dental age (DA) is defined as "the morphological state of an individual's dentition without reference to their actual age".1 When compared with somatic, skeletal and sexual ages, DA was found to be less variable in assessing the chronological age.2
The most common DA estimation methods are the Moorrees, Fanning and Hunt method, the Demirjian, Goldstein and Tanner method and the Gustafson and Koch chart.3-6 These methods were based on specific populations i.e. the reference population which has its own ethnic complexity and background.6 Therefore, using these methods in other populations will always carry the risk of inaccuracy. To overcome the risk, population-specific tables were suggested to match the diversity of each population.8-10
Examples include the specific tables which were generated for each population in the following countries: Southern Finland, India, Korea, Saudi Arabia, Pakistan and South Africa.8,10-16 These specific tables were tested in their own reference populations and found to be more accurate than standard methods.
The Phillips tables are population-specific tables which were designed to match the diversity of the South African population. Phillips' tables were published in 2009 and consisted of three tables (Tygerberg, Indian and Nguni) derived from 1476 panoramic radiographs of South African children from different ethnic groups (White, Coloured, Indian and Black). These tables were tested in a sample of South African children and adolescents and were found to be the most accurate method for DA estimation if the ethnic origin is known.16
Proffit's DA description has been used in dental faculties throughout the world as a teaching tool to explain the concept of DA to dental students. It has been used extensively as a clinical tool in interceptive orthodontics and in paediatric dentistry. The description consists of eight stages from DA six to DA fifteen.16 The description uses tooth eruption but also evaluates tooth formation and mineralization on a radiograph in order to determine the DA.16
The Proffit description for DA has been widely accepted in academia because it is simple and straightforward. It has however never been tested scientifically against any of the other DA estimation methods.
The South African population is ethnically diverse and includes a significant section of the population that is of mixed ethnic origin (Census, 2011). Previous work has taken ethnic issues into account and an influence has been demonstrated.8-16 The aim of this study was to compare the accuracies of the Phillips and Proffit methods of estimating the DA from panoramic radiographs In a random sample of South African children of all races. Any ethnic influence would therefore be equal for either method, and the comparisons would be valid. An objective of this study was to assess the accuracy of the Proffit method, which is widely taught, when applied to a multi-ethnic group of South African children.
MATERIALS AND METHOD
Permission to carry out the study was obtained from the Senate Research Ethics Committee of the University of the Western Cape.
A retrospective cross-sectional study was carried out. The study population was selected from amongst the available panoramic radiographs taken from the records database of the Department of Paediatric Dentistry (University of the Western Cape).
Inclusion criteria
-
Good quality panoramic radiographs.
-
Patients with a chronological age between 6 and 11 years.
-
The date on which the panoramic radiographs were taken had to be recorded.
-
There also needed to be information regarding the gender and the date of birth.
Exclusion criteria
-
Radiographs of poor quality.
-
Radiographs demonstrating gross pathology.
-
Bilateral congenitally missing permanent teeth. (If a tooth was only absent on one side, the contralateral tooth was assessed.)
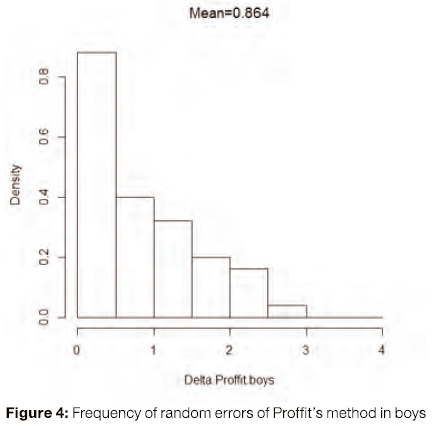
The sample finally comprised 100 panoramic radiographs which were sorted according to chronological age and sex by someone other than the author. The radiographs were then divided into five groups according to the age of the patient at the time of the radiograph being taken.
Privacy of the participant data found in the folders was respected and confidentiality was strictly maintained. Informed consent had been obtained during the initial clinical evaluation.
The panoramic radiographs were saved as JPEG image files and were viewed using the Photo gallery programme.
Data collection was done using two forms i.e. one for each DA estimation method. Each panoramic radiograph was assessed using both the Phillips and Proffit criteria as described in the literature.15,16
The sample was examined by the author only who was blinded as to the chronological age and the gender of the child when estimating the DA.
The calculation of actual chronological age was done by subtracting the date of birth from the date on which the radiograph was taken. The calculation gave the age in fractions of years which was approximated to two decimal points.
The accuracy of the tested methods in this study was defined by how closely the estimated DA was to the chronological age. A positive number was considered to be an overestimation while a negative number was considered an underestimation.
RESULTS
Intra-observer reliability
Twenty percent of the sample was re-examined after two weeks. The mean differences between the data recorded for the initial and the repeated assessments for both the Phillips and Proffit methods were not statistically significant, p-values = 0.5575 and 0.6453 respectively. The results show that the readings for both methods are reliable and unbiased.
Phillips' method
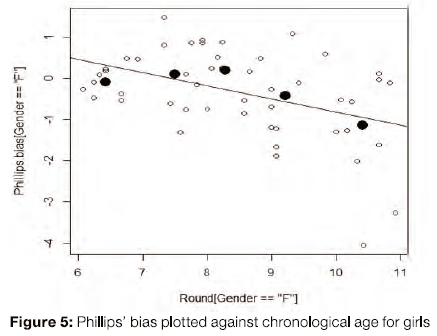
The present study shows that Phillips' method predominantly underestimated the age in this sample of South African girls and boys by 4 and 6 months respectively (p-value = 0.03 and <0.0001 respectively). The overall bias was statistically significant. Furthermore, for girls sample the underestimation appears to be age dependent (Figure 5 shows linear regression line with intercept= 2.354, slope= -0.318 and p-value= 0.002 which is statistically significant). The bias is positive at the smaller age groups i.e. from 6 to 8.9 years and negative at the larger age groups i.e. from 9 to 11 years. So, the older the girl, the more likely the Phillips method is to underestimate the age. However, for the boys' sample the underestimation is not age dependent (linear regression line with intercept -0.121, slope= 0.043 and p-value = 0.58 which is not statistically significant). This means that Phillips' method was generally biased when applied to the study sample.

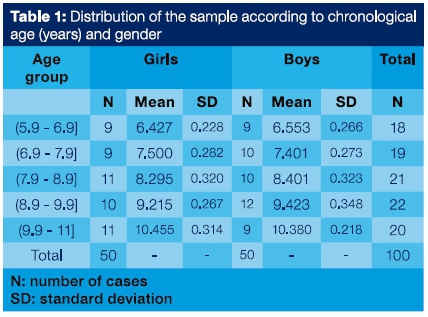
Figures 1 and 2 indicate that for girls the mean error according to Phillips is greater than the mean error according to Proffit.
Proffit's Method
The results of age estimation in girls and boys show that Proffit's method underestimates the DA of girls and boys by two days and two months respectively (p-value = 0.97 and 0.15 respectively). The underestimation is not statistically significant. Furthermore, unlike the Phillips method, there is no age dependent bias (p-values for the linear regressions are 0.11 and 0.78 respectively) which are not statistically significant.
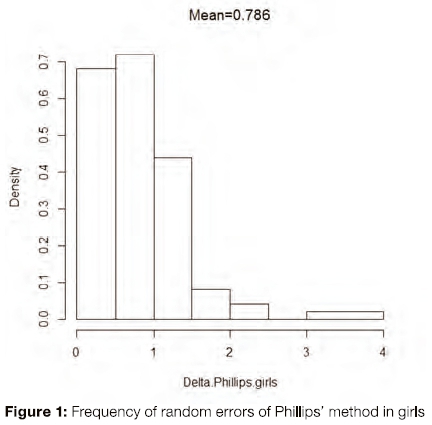
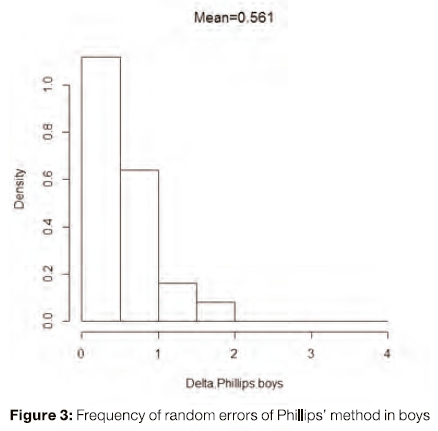
Figures 3 and 4 indicate that the mean error for boys according to Phillips is smaller than that of Proffit's mean error (p-value of 0.002).
DISCUSSION
The bias demonstrated in the current study of the Phillips method is contrary to the report by Hag-Mahmoud17 who investigated the accuracy of the method in a sample of Sudanese children. That author found that Phillips' method overestimated the age of girls by two and half months and underestimated the age of boys by only one month (unpublished data).17 This overall bias was not statistically significant. However, the difference between the present study and Hag-Mahmoud's study17 could be explained by differences in age groups, age distribution across the groups, ethnic origin and statistical analysis between the two studies.
The inaccuracy of Phillips' method found in the current study was not an expected outcome as the method was derived originally from a sample of South Africa children. However, this could be due to several reasons. The Phillips' method is a scoring system which depends on multiple readings of the developmental stages for eight permanent teeth. Although the intra-observer reliability score showed unbiased results, subjectivity of the readings cannot be completely excluded.18 Furthermore, distinguishing between the different developmental stages could be very challenging especially when the tooth presented as a borderline stage. It is difficult to judge whether a half or a third of the root has formed if you don't know the final root length.19 The absence of the intermediate stage (i.e. one third of the root completed) may contribute to the biased estimation.15
Phillips' method also Included the mandibular third molar which Is known for its variability and unpredictability.20 According to Miles,21 DA estimation using the third molar can produce an error of two years. This may have affected the scoring system and led to bias in the overall results.
Proffit's method
No age dependent bias was demonstrated for Proffit's method, the p-values for the linear regressions being not statistically significant. This means that the method was unbiased when applied to the study sample.
There are no other reports in the literature to allow for comparison with the present study. Proffit published his description of DA in 1986. It has however not been compared with the other DA estimation methods in the literature. Despite the value of Proffit's description, it has not been considered as a bona fide DA estimation method.
Random errors
The accuracy of age estimation does not depend only on the overall bias of the estimating procedure. The random errors associated with the overall bias are extremely important. The frequency distribution of the random errors for Phillips and Proffit are represented in figures 1 to 4.
The histograms indicate that there is no significant difference in the mean errors for the girls' sample. However, for the boys' sample, the p-value is 0.002 which is statistically significant.
This means that Phillips' method will have fewer random errors compared with Proffit when DA estimation is done on boys. The results of this study support the argument that population specific tables may not be very accurate within the reference population because of the intrinsic variation - which is difficult to explain.
CONCLUSION
It can be concluded that if one had to choose between the two DA estimation methods for girls, Proffit's method would be more appropriate because it underestimates the age by only two days and has the same frequency of random errors as does Phillips' method. However, if one had to choose between the two methods for boys, the situation should be evaluated carefully. For boys, the Phillips method has fewer random errors but a larger overall bias (six months) whereas Proffit's method has more random errors but less overall bias (two months).
The choice between the two methods should therefore depend on the purpose of the estimation. If the method is used for estimating the age in a single individual with an unknown chronological age e.g. for forensic and immigration purposes, the method with less random error would be more preferable (i.e. Phillips). However, if the age estimation method is used for age estimation in populations with a known mean chronological age e.g. epidemiological studies, the method with less overall bias is preferred (i.e. Proffit).
The accuracy of the Profitt method used in a multi-ethnic group reflects the validity of this research. This technique of dental age prediction may be used with confidence as a reliable teaching tool.
Conflict of interest
The authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest, or non-financial interest in the subject matter or materials discussed in this manuscript.
ACRONYMS
DA: Dental age
References
1. Grover S, Marya CM, Avinash J, Pruthi N. Estimation of dental age and its comparison with chronological age: accuracy of two radiographic methods. Med Sei Law 2012; 52(1): 32-5. [ Links ]
2. Demirjian A, Buschang P, Tanguay R, Patterson, DK. Interrelationships among measures of somatic, skeletal, dental, and sexual maturity. Am JOrthod1985; 88(5): 433-8. [ Links ]
3. Moorrees CF, Fanning EA, Hunt Jr EE. Age variation of formation stages for ten permanent teeth. J Dent Res 1963; 42(6): 1490-1502. [ Links ]
4. Demirjian A, Goldstein H, Tanner JM. A new system of dental age assessment. Human Biology 1973; 45(2): 211-27. [ Links ]
5. Gustafson G, Koch G. Age estimation up to 16 years of age based on dental development. Odontol Revy 1974; 25(3) 297-306. [ Links ]
6. Phillips VM, Van Wyk Kotze TJ. Testing standard methods of dental age estimation by Moorrees, Fanning and Hunt and Demirjian, Goldstein and Tanner on three South African children samples. J Forensic Odontostomatol 2009; 27(2): 20-8. [ Links ]
7. Olze A, Bilang D, Schmidt S, Wernecke K, Geserick G, Schmeling A. Validation of common classification systems for assessing the mineralization of third molars. Int J Legal Med 2005; 119(1): 22-6. [ Links ]
8. Baghdadi ZD. Dental maturity in Saudi children using the Demirjian method: a comparative study and new prediction models. ISRN Dentistry 2013; 1-9. [ Links ]
9. Almeida MSC, Pontual AdA, Belträo RT, Belträo RV, Pontual MLD. The chronology of second molar development in Brazilians and its application to forensic age estimation. Imaging Sei Dent 2013; 41(1 ):1-6. [ Links ]
10. Sukhia RH, Fida M, Azam SI. Dental age table for a sample of Pakistani children. Eur J Orthod 2012; 34(1): 77-82. [ Links ]
11. Kataja M, Nyström M, Aine L. Dental maturity standards in southern Finland. Proceedings of the Finnish Dental Society 1989; 85(3):187-97. [ Links ]
12. Koshy S, Tandon S. Dental age assessment: the applicability of Demirjian's method in South Indian children. Forensic Sei Int 1998; 94(1): 73-85. [ Links ]
13. Sarkar S, Kailasam S, Kumar PM. Accuracy of estimation of dental age in comparison with chronological age in Indian population-A comparative analysis of two formulas. J Forensic Leg Med 2013; 20(4): 230-3. [ Links ]
14. Lee SS, Kim D, Lee S, Lee U.Y, Seo JS, Ahn YW, Han SH. Validity of Demirjian's and modified Demirjian's methods in age estimation for Korean juveniles and adolescents. Forensic Sei Int 2011; 211 (1 -3) 41 -6. [ Links ]
15. Phillips VM, Van Wyk Kotze TJ. Dental age related tables for children of various ethnic groups in South Africa. J Forensic Odontostomatol 2009; 27(2): 29-44. [ Links ]
16. Proffit WR, Fields HW, Sarver DM. Contemporary Orthodontics. 4th ed, St. Louis: Mosby Elsevier, 2007. [ Links ]
17. Hag-Mahmoud NE. Testing the standard method of dental age estimation by Demirjian and Phillips age related tables on a Sudanese Arab children sample. Unpublished. A mini-thesis submitted in partial fulfilment of the requirements for the degree of MSc in Forensic Dentistry, 2012; University of the Western-Cape. [ Links ]
18. Li G, Ren J, Zhao S, Liu Y, Li N, Wu W, Yuan S, Wang H. Dental age estimation from the developmental stage of the third molars in western Chinese population. Forensic Sei Int 2012; 219(1-3):158-64. [ Links ]
19. Leurs IH, Wattel E, Aartman I HA, Etty E, Prahl-Andersen B. Dental age in Dutch children. Eur J Orthod 2005; 27(3): 309-14. [ Links ]
20. Garn SM, Lewis AB, Bonné Β. Third molar formation and its development course. Angle Orthod 1962; 32(4): 270-9. [ Links ]
21. Miles A. The dentition In the assessment of individual age in skeletal material. Dental Anthropology. Symposia of the Society for the Study of Human Biology (1963); 191. [ Links ]
 Correspondence:
Correspondence:
Nadia Mohamed
Paediatric Dentistry, Faculty of Dentistry, UWC.
Email address: namohamed@uwc.ac.za

