










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.73 no.4 Johannesburg Mai. 2018
RESEARCH
Evaluation of dentine damage after root canal preparation with rotary NiTi instruments
Ahmed SI; Saayman CMII
IBChD, PDD, MSc, Lecturer, Restorative Dentistry, Faculty of Dentistry, University of the Western Cape. Email address: suahmed@uwc.ac.za. Tel no.: (021) 937 3091
IIBChD, MSc, Principal Stomatologist, Head Clinical Unit, Restorative Dentistry, Faculty of Dentistry, University of the Western Cape. Email address: cmsaayman@uwc.ac.za. Tel no.: (021) 937 3097
ABSTRACT
AIM: The aim of this in-vitro study was to investigate the possible damage to root canal dentine during instrumentation with four different nickel-titanium rotary instruments and stainless steel hand files.
MATERIALS AND METHODS: 90 permanent human mandibular molars, each having two mesial canals, were selected for the study. The mesial roots were randomly divided into six groups (n=30), with one group remaining unprepared as the control. The remaining five groups were randomly assigned to one of the nickel-titanium rotary instrumentation systems (Wave One ™, ProTaper NEXT™, iRaCe™, BT-Ftace™), and to a stainless steel hand file group. Roots were prepared and segmented at 3mm, 6mm and 9mm. Each segment was studied under stereomicroscope to detect any dentine damage.
RESULTS: Data for the different groups were collected and summarised as percentages. Pairwise comparisons between the groups were done using Fisher's exact test. There were no significant differences between the four NiTi groups. However, there was a significant difference between the four groups and the stainless steel group (p<0.0001).
CONCLUSION: Under the conditions of this in vitro study the use of all NiTi rotary instrumentation systems resulted in dentine damage whereas stainless steel hand instrumentation did not cause dentine damage.
INTRODUCTION
The objective of root canal shaping is to create a continuous taper in the canal with a small diameter at the apical foramen and enlarging to be greatest at the coronal orifice. The original canal shape and curvature are maintained to allow for adequate irrigation and completion of obturation.1, 2
Debridement is followed by placement of an effective root canal filling material during obturation and a well sealed, functional coronal restoration to prevent further entry of bacteria. Debridement on its own will not effect significant clinical reduction in bacterial growth and therefore antibacterial irrigation is an important adjunct to mechanical preparation of the root canal systems.3'4 The advent of the first nickel-titanium rotary instruments marked a revolution in endodontics, resulting in a shift from hand instrumentation to rotary instrumentation.4 Although the use of nickel-titanium instruments allows for reduction of preparation time, centred canals and standardised canals, research has shown that an adverse consequence of rotary nickel-titanium instrumentation may be damage to dentine and the creation of defects in root canal walls,5'6 as a consequence of rotational forces being applied to the root canal walls. These defects can vary from craze lines and microcracks to incomplete and complete fractures in the root canal dentine.711
Damage to dentine can be classified as follows:
-
No defect- no lines/cracks present in dentine.
-
Incomplete crack-presence of a line from canal wall into the dentine but not extending to the outer surface of root.
-
Complete crack- presence of a line extending from root canal wall to outer surface of the root.
-
Craze lines- presence of lines that do not reach any surface of the root/ outer surface of dentine and do not reach the canal wall.12
During hand instrumentation, less aggressive movement is evident compared with engine operated instruments.13 Greater friction is observed between nickel titanium rotary files and root canal walls when compared with hand instrumentation, and thus the greater the amount of dentine removed, the greater the risk of causing dentine damage during instrumentation.14 The total volume of dentine removed is greater with rotary instrumentation when compared with hand instrumentation. The use of rotary instrumentation results in a greater incidence of craze lines compared with hand operation.9,15-17
Rotary instrumentation is associated with increased numbers of rotations and the application of a rotational force to the root canal walls, which may contribute to dentinal damage and dentine microcrack formation.17,18 Transitory stress concentrations, caused where the rotary instruments and the root canal dentine make contact, may result in dentinal defects. These stress concentrations may be transmitted through the root to the outer surface where dentinal bonds may be destroyed.11,19-21
Specific features of rotary instrumentation and shaping procedures may influence the occurrence of dentine damage and defects. These factors include, amongst others, tip design, design of cutting blade, cross-sectional geometry, tip configuration, taper (constant vs progressive), pitch (constant vs variable) and flute form.8,9,13,17,22-23 The incidence of dentinal defects may also be associated with the techniques followed in nickel-titanium rotary preparation (reciprocating motion, single instruments, multiple instruments and combination of different techniques).12 Other factors that may influence dentine damage is the effect of sodium hypochlorite and ethylenediaminetetra-acetic acid (EDTA) on root canal dentine during canal debridement and shaping. Sodium hypochlorite may have an effect on dentine mineral content, micro-hardness and flexural strength.23-27 Irrigants can thus alter surface characteristics of dentine. EDTA is used in endodontics as a chelator, for smear layer removal and increased dentine permeability.27 The chelating action of EDTA results in the softening of calcified components of dentine and subsequent decrease in micro-hardness of dentine.28
Recently single file systems as well as NiTi instruments manufactured from M-wire were introduced. ProTaper NEXT and WaveOne are manufactured with M-wire. WaveOne is a single file system, used in reciprocating motion. ProTaper NEXT is used in rotational motion and has an off-centre rectangular cross-section, which allows for a swaggering motion in the canal. iRaCe and BT-Race systems are NiTi instruments used in rotational motion. IRaCe has a triangular cross section with a rounded safety tip. BT-Race features a booster tip which is designed to allow files to follow curvature in the root without undue stress on instruments and root canal walls, while keeping files centred in the root canal.
This study investigated the effect of ProTaper NEXT(PTN), WaveOne (WO), ¡RaCe(iR) and BT-Race on root canal dentine, when used with 5,25% sodium hypochlorite and 17% EDTA.
MATERIALS AND METHODS
Mandibular molars were obtained from the Oral Surgery and service rendering clinics of the Faculty of Dentistry, University of the Western Cape. The teeth collected for the purposes of this study were extracted for reasons unrelated to the objectives of this study. Prior to commencement of this study, ethical clearance was obtained from the Research Committee of the Faculty of Dentistry, University of the Western Cape (Project number: 13/10/72). Every aspect of this study was conducted in accordance with the ethical and safety guidelines for handling human tissues and conducting laboratory studies, as prescribed by South African law: The Health Professions Act 56 of 1974 (Health Professions Council of South Africa, 2008).
Teeth with severely curved mesial roots were excluded from the study. The external root surfaces of all available teeth were was Inspected under a stereomicroscope (Nikon SMZ 10) at 12X magnification to identify any external defects or cracks. Teeth with defective roots were rejected. 90 mandibular first molars (180 mesial root canals) were finally selected and stored in distilled water. The crowns of these teeth were removed at the cemento-enamel junction (CEJ) using a diamond disk cutter (Struers Minitom, 350 μm blade thickness), under water cooling. The distal roots of the teeth were removed. The remaining mesial roots had an approximate length of 11mm. A polyvinyl silicone impression material (President Putty Coltene/Whaledent) was used to coat the cemental surface of the roots to simulate the periodontal ligament space and to reasonably mimic the mechanism of stress distribution during debridement.
The total sample was randomly divided into six groups (n=30), with one group receiving no instrumentation and serving as the control group. The remaining five groups were randomly assigned to a NiTi rotary instrumentation system as well to a stainless steel group.
Root segment preparation
The detailed debridement procedure for each system was as follows:
For all groups: canal patency was established with a no. 10 stainless steel K-file (FKG DENTAIRE™). The working length was set 1mm short ofthat length. The glide path was established with hand files: numbers 8, 10 and 15 stainless steel Κ files (FKG DENTAIRE™). The canals were irrigated with 5.25% sodium hypochlorite (Protea Chemicals) during glide path establishment. 17% EDTA (Glyde File Prep™, Dentsply Maillefer) was used as a lubricant during glide path establishment. After the glide path was established for each sample group, the allocated rotary nickel-titanium system was used for canal debridement. 5.25% sodium hypochlorite and 17% EDTA (Glyde File Prep™, Dentsply Maillefer) was used as an irrigant and chelator during debridement. Approximately 12ml sodium hypochlorite solution was used per canal. Canals were irrigated with sodium hypochlorite after each file change, and instrument flutes were cleaned on cotton gauze after insertion In canal. The EDTA solution was used after sodium hypochlorite rinse in the canals, usually twice). Patency was confirmed between each file. Sodium hypochlorite was used as the final rinse. The Wave One endo motor and handpiece (Dentsply Maillefer) was used for all canal preparation. All the NiTi rotary sample groups were prepared in rotational motion, except for the Wave One group which was prepared in reciprocal motion. One set of rotary Instruments was used for two canals (mesial roots). The speed and torque was programmed for each NiTi rotary system according to the manufacturers' recommendations to standardise the study. All procedures were carried out by a single operator.
GROUP 1: ProTaper NEXT™ (Dentsply Maillefer) (n=30) The ProTaper NEXT™ X1 Dentsply Maillefer (017/04) was used for Initial debridement until working length was achieved. Files were brushed with EDTA and manouvered down the glide path. This was followed by ProTaper NEXT™ X2 (025/06) to the working length. After each ProTaper NEXT™ instrument, recapitulation with a no 15 Κ file was effected. 5.25% sodium hypochlorite and 17% EDTA were used during debridement. Recommended speed: 300 rpm Torque: 2 Ncm
GROUP 2: Wave One™ (Dentsply Maillefer) (n=30) The single file for Wave One™ (Dentsply Maillefer) was selected accordingly and used to debride until working length was achieved. If a no. 10 K-file moved to length easily, was loose or very loose, a WaveOne™ Primary file (25/08) was used. The files were used In up and down movement no more than three to four times, with little force. 5.25% sodium hypochlorite and 17%EDTA was used during debridement. Recapitulation was done with a no 15 K-file. Recommended speed: 300 rpm Torque : 2Ncm
GROUP 3: BT Race FKG Dentaire (n=30)
BT1 (10/06) was used forfinalisation of glide path and conservative enlargement of the coronal third.
BT2 (35) was used for preparation of the apical third to full working length.
BT3 (35/04) was used for final shaping of canals until full working length was reached. 5.25% sodium hypochlorite and 17% EDTA was used during debridement. Instruments were used with a long and gentle pecking motion (3-4 back and forth strokes). Recapitulation was done with a no 15 K-file. Recommended speed: 800 rpm Torque: 1.5 Ncm
GROUP 4: iRaCe™ (FKG Dentaire) (n=30) R1 file (15/06) was used to working length. Thereafter an R2 file (25/04) was used to working length to continue shaping. 5.25% sodium hypochlorite and 17% EDTA were used during debridement. Long back-and-forth strokes with the instrument were applied, with a light touch. Recapitulation was done with a no 15 K-file.
Recommended Speed: 600 rpm Torque: 1.5 Ncm
GROUP 5: Stainless steel hand instruments (Dentsply Maillefer) (n=30)
All canals were prepared using stainless steel instruments to working length, and recapitulation was effected between each file. Canals were prepared to a no. 25 stainless steel K-file (Dentsply Maillefer). Once the instrument went to working length, recapitulation was done, followed by the consecutive instrument. 5.25% sodium hypochlorite and 17% EDTA were used during debridement.
GROUP 6: Control group (n=30)
No preparation was carried out in this sample group.
ROOT SECTIONING
The roots in all six groups were sectioned under water cooling at 3, 6, 9mm from the apex, using a diamond disc cutter (350 μιτι blade thickness) attached to Stueres Minitom. Root segments were then observed under stereomicroscope (Nikon SMZ 10) under 12X magnification and images of each section were captured at 40X using a digital camera (Leica DFC 290). The root segments were kept wet at all times and the stereo microscope examination was done immediately after sectioning of roots.
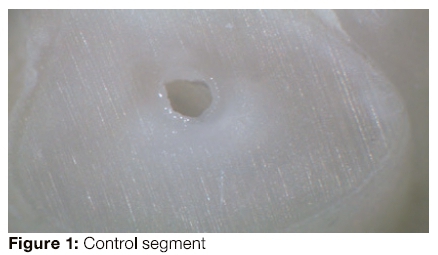
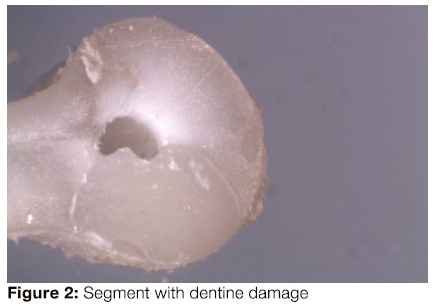
The root segments were evaluated for any defect in the dentine at any level in the segment slice. Defects were categorised as: 'no defect' and 'all other defects'. 'No defect' is defined as dentine devoid of any lines or cracks where both the external root surface and the internal root canal wall had no defects. Other defects included all lines that were observed from the root canal wall to the outer root surface (fractures); as well as any lines that did not reach either the canal lumen or the outer root surface.30
The author and an impartial second observer observed the images.
RESULTS
Statistical analysis
The results were expressed as the number and percentage of dentine damage in each group.
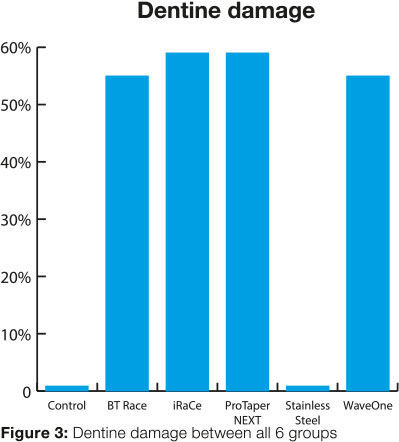
The study had a total sample size of 180, which was divided into six groups, each having 30 samples. Each sample was investigated at three segments; namely 3mm, 6mm and 9mm from the apex. Table 1 shows the incidence, as percentages of each sample of 30, of damage/defect observed in each group.
The control group (n=30) had zero (0) events and the stainless steel group (n=30) also recorded zero (0) events. The BT-Race group (n=30) had 17 events out of the sample, giving a 56,67% incidence of dentine damage/defects. The iRaCe group and the ProTaper NEXT group both had 18 events out of the total sample, giving a 60% incidence of dentine damage/defects. The WaveOne group (n=30) had 17 events out of the total sample, giving a 56,67% incidence of dentine damage/defects. There were no statistically significant differences between the groups: WaveOne, ProTaper NEXT, iRaCe and BT-Race. However, there is a significant difference between the four groups and the stainless steel group (p<0.0001).
DISCUSSION
The purpose of this in vitro study was to investigate the effect of nickel titanium rotary instrumentation on root dentine, by recording the appearance of dentine damage, whether it be a defect, microcrack, crack, craze line or fracture.
The dentine damage observed in this study may be caused by the interaction of four actions on root canal dentine; namely, the mechanical preparation and shaping of canals by the different NiTi rotary systems (each with their own specific features and differences), the chemical attack of the irrigants and chelating agents on the root dentine (5,25% sodium hypochlorite and 17% EDTA), the sectioning method of the root segments and the inherent anatomy of the extracted roots.
These aspects are discussed as follows: In this study, dentine damage was observed in all the teeth which had received nickel titanium rotary instrumentation (Groups WaveOne™, ProTaper NEXT™, iRaCe™, BT-Race™) and not in the stainless steel and control groups, which was not instrumented. This would imply that the sectioning method did not induce dentine damage, so it may be concluded that the dentine damage was likely as a result of the different rotary preparation procedures alone.
The effectiveness of nickel titanium rotary instruments during debridement is influenced by the number of rotations of the instrument in the canal. More rotations are necessary to complete preparation with nickel titanium rotary files as compared with hand instruments.30 The greater the number of rotations in the canals, the greater the chance of dentinal defects.14,20 This may explain the lack of dentine damage seen in the stainless steel hand instrument sample group in the present study, which is in agreement with the findings of Bier et al.14 Shemesh et al.29 and Priya et al.21 Hand Instrumentation is of a less aggressive nature as compared with nickel titanium rotary instrumentation. The lack of dentine damage in the stainless steel hand file group could be attributed to both the lack of the continuous rotational motion as well as to the 0.02 taper of hand files, when compared with the taper of the NiTi rotary instruments used in the present study. This plausible explanation is in agreement with additional previous studies, which also reported no defects with hand instrumentation.6'16 As all NiTi rotary instrument groups in this study presented with dentine damage, rotational force during preparation conceivably contributed to dentine damage.
In the present study, both rotary and reciprocal motion nickel titanium instruments resulted in significantly more dentine damage compared with hand instrumentation (p<0.0001). This result could be related to the contact areas between the rotary instrument and the root dentine. These contacts result in momentary stress concentrations which could cause dentine damage on the root dentine surface. Greater contact stress levels are present in the root canal during NiTi instrumentation, which is influenced by the mechanical behaviour of files. According to Cicek et al.9 and Priya et al.21 a greater volume of dentine is removed during canal preparation with nickel titanium rotary instruments due to rotational forces, and this may have an effect on the incidence of dentine damage. The resulting thinner dentine may weaken the root structure, and there will subsequently be an increased risk of fracture of roots.31 The results of the present study maintained the conclusion as determined by Shemesh et al. that nickel titanium rotary instrumentation damages the root dentine.29
The incidence of dentine damage could possibly be connected with nickel titanium rotary preparation techniques (reciprocating motion, single instruments, multiple instruments and combination of different techniques).12 Reciprocating motion allows for a more centred preparation compared with rational motion.32 Berutti et al.32 reported that the reciprocating motion of WaveOne aids with stress release as the file progresses down the canal. NiTi systems with both reciprocal and rotational motion were investigated in this study; and both motions resulted in dentine damage, although no statistical significance was noted between the reciprocal and rotational systems when looking at the total number of roots with dentine damage.
With increased rotational speed, greater cutting efficiency is achieved. Studies by Capar et al.33 showed that increased revolutions per minute (rpm), 500rpm being compared with 250 rpm, less dentine damage was found with the increased speed (rpm). In the current study, no statistical difference was noted in the amount of associated dentine damage between the rotary Instrumentation using higher rpm (BT-Race™ and iRaCe™ at 800 and 600 rpm respectively) compared with the lower rpm (both WaveOne™ and ProTaper NEXT™ at 300rpm).
The extent of dentine damage may be influenced by the tip design, cross-section geometry, constant or progressive taper type, constant or variable pitch, and flute form.6 The properties and behaviour of various Nickel-titanium instruments differ according to torsional and bending characteristics, cyclic fatigue and flexibility.6 As nickel-titanium rotary instruments have various design and functional features, different manufacturer's systems may influence the effect that these features could have on dentine.34 Topguoglu et al.35 stated that nickel titanium rotary files with greater tapers can thus cause increased friction and stresses within the canals, compared with hand instrumentation with a 0.02 taper.12 Consequently, the design and taper of the instruments and the motion of instrumentation were variables considered in the present study.12
All four groups had dentine damage in the coronal area, and this observation is in agreement with previous studies by Priya et al.21 In the coronal area (9mm from apex), WaveOne use had produced a 16,67% incidence of dentine damage, the ProTaper NEXT group recorded 26,67% dentine damage and the iRaCe and BT-Race groups were associated with an incidence of 13,33% and 26,67% respectively.
The dentine damage seen in the samples treated with the ProTaper NEXT nickel-titanium system was 26,67% in the coronal third, 20% In the middle third and 13,33% in the apical third. This decrease from the coronal third to the apical third could be attributed to the variable taper of the instrument (X1 has 0.04 taper, X2 has 0.06 taper and X3 has 0.07taper), The ProTaper NEXT files have an off-centred rectangular cross-section which promotes a swaggering motion in the canal. It decreases taper lock and screw effect. At any given time only two points of the file's cross section will make contact with the root canal wall.33 This may be the reason for decreasing damage in root canal from the coronal third to the apical third.
In the BT-Race™ group, 6,67% of dentine damage was noted in the apical third which may be attributed to the BT2 instrument having no taper, while BT3 has a taper of 4%. ProTaper NEXT™ has a variable taper as noted asbove. iRaCe™ has a 4% taper and WaveOne™ has a taper of 8%. These variations in design may have contributed to the differences in dentine damage in the apical third between the different rotary systems.
Rotary instruments with large tapers may cause more complete and incomplete dentinal cracks.17,21 Decreasing the taper sequence of finishing files increases the strength of the files but also increases the stiffness at the tip of the instrument and the larger and more tapered instruments should be used with caution.36 The taper of rotary files could be a contributing factor In the generation of cracks due to increased stress concentration on root canal walls.6,37 Stainless steel files have 0, 02 taper and no rotational force which could contribute to the lack of dentine damage in the stainless steel group compared with the effects seen in the NiTi rotary instrumentation groups.
The stiffness of a file is related to cross-section, size, taper, method of manufacture, and material of the instrument.19 The differences between the instruments tested regarding the incidence of dentinal damage may be due to the cross-sectional design of the instruments, which influences the behaviour of the files in the canal. ProTaper NEXT has a modified rectangular cross-section, WaveOne has a modified convex triangular cross-section and both BT-Race and iRaCe have triangular cross-sections.
Both ProTaper NEXT and WaveOne are manufactured with M-wire to increase strength and resist cyclic fatigue. Any difference In dentine damage between ProTaper NEXT and WaveOne compared with BT-Race and iRaCe at the different segmentation levels could be attributed to the flexibility of the M-wire when compared with nickel titanium.
WaveOne is a single file system and less time is required during preparation.15 The difference at segmentation levels could be attributed to a single file used for canal shaping compared with multiple files used for canal shaping in the ProTaper NEXT, BT-Race and iRaCe preparations.
BT-Race features a booster tip which is designed to allow files to follow curvatures in the root without undue stress on instruments and root canal walls, while keeping files centred in the root canal. This allows canals to be instrumented to the correct biological size. The booster tip may be a plausible factor to explain the difference In apical dentine damage compared with the other sample groups. iRaCe features a rounded safety tip which allows for canal centering and guidance in the root canal, which may contribute towards the explanation of differences between sample groups.
The ability of dentine to resist fracture is an important structural characteristic, forming a barrier preventing crack propagation from the enamel.38, 39 Thus, any factors that could result in changes to dentine structure will potentially result in the incidence of dentinal damage. The use of root canal irrigants and chelating agents in combination with nickel titanium rotary instrumentation has a potential effect on root dentine. In this study, sodium hypochlorite solution at a concentration of 5,25% and 17% EDTA (Glyde™) was used during root canal debridement and shaping. Studies have shown that sodium hypochlorite alters the mechanical properties and surface characteristics of root canal dentine during canal preparation.24 A higher concentration of sodium hypochlorite solution enhances efficacy but also significantly reduces the modulus of elasticity and flexural strength of root dentine.7,20,23
The use of sodium hypochlorite as a root canal irrigant is the most common choice during root canal treatment, but the concentration varies according to the clinician's preference.40 The concentration and contact time of sodium hypochlorite on dentine microhardness is a factor to consider when looking at the effect on dentine, especially in terms of dentinal damage. It is tempting in the clinical situation to use a higher concentration of sodium hypochlorite.41 Slutzky-Goldberg et al.25 and other workers42,44 found that a higher concentration of sodium hypochlorite (5.25% and 6%) and increased contact time resulted in a greater decrease in dentine microhardness compared with the effect of a lower concentration. At these higher concentrations a greater decrease of flexural strength has been observed.45,46
Pop et al.11 used 1% sodium hypochlorite and this limited the effect on dentine, so damage could be ascribed mostly to the mechanical shaping. It can be deduced that an increased concentration of sodium hypochlorite may have an effect on dentine structure and consequently induce dentine damage.
In this study sodium hypochlorite was used at 5, 25% and thus the modulus of elasticity, mineral composition, flexural strength and micro-hardness of dentine could have been influenced by both the irrigant and the chelating agent, which possibly contributed to the dentine damage observed. Although many studies have been conducted to evaluate the dentine damage caused by various instruments, very few have studied the effect of different irrigation solutions on dentine damage. Further investigations are required to evaluate this possibility.
Once root canal debridement is started, a smear layer forms on the root canal wall and the removal of this smear layer contributes to the success of root canal treatment.27 An irrigation regimen of EDTA and sodium hypochlorite is recommended for complete removal of the smear layer so that both the inorganic and organic components are removed.47,48 EDTA is used as a chelator to remove the inorganic component of the smear layer, while sodium hypochlorite removes the organic component. The concentration of EDTA is preferred at 17%.49 Time of exposure with EDTA also has an effect on the dentine decalcification, so increased exposure will result in greater decalcification of dentine.50 As chelating agents alter the calcium to phosphorous ratio, there may be an effect on the dentine microstructure.51 Taneja et al.52 found that exposure of dentine to a combination of 5,25% sodium hypochlorite and 17% EDTA caused a reduction in dentine microhardness. Belli et al.53 reported that 17% EDTA also resulted in increased stresses in root dentine which may contribute to the risk of fracture. The current study relied on the same combination and concentration of sodium hypochlorite and EDTA, and although dentine microhardness was not investigated, it is clear that the effect may have been associated with the observed dentine damage.
CONCLUSION
Within the confines of the present study, the following can be concluded:
1. Even though this in vitro study did not reproduce the complete clinical scenario, it confirmed that all the NiTi rotary instrumentation systems studied resulted in dentine damage to varying degrees.
2. Stainless steel instrumentation did not result in dentine damage.
3. Differences were found between NiTi rotary systems with regard to the amount of dentine damage and also in relation to the specific third of the root (apical, middle or coronal) affected.
ACRONYMS
EDTA: Ethylenediaminetetra-acetic acid
References
1. Peters OA. Current challenges and concepts in the preparation of root canal systems: A review. J Endod 2004; 30(8): 559-67. [ Links ]
2. Cohen S, Hargreaves KM. Cohen's Pathways of the Pulp, 10th ed. Mosby Elsevier, 2011: 287-89. [ Links ]
3. De-Deus G, Garcia-Filho P. Influence of the NiTi rotary system on the debridement quality of the root canal space. Oral Surg Oral Med Oral Pathol Radiol 2009; 108(4): e71-e76. [ Links ]
4. Young GR, Parashos P , Messer HH. The principles of techniques for cleaning root canals. Aust Dent J 2007; 52(1): S52-S63. [ Links ]
5. Shemesh H, Roeleveld AC, Wesselink PR, Wu MK. Damage to root dentin during retreatment procedures. J Endod 2011; 37(1): 63-6. [ Links ]
6. Yoldas O, Yilmaz S, Atakan G, Kuden C, Kasan Ζ. Dentinal microcrack formation during root canal preparations by different NiTi rotary instruments and the Self-Adjusting File. J Endod 2012; 38(2): 232-5. [ Links ]
7. Adorno CG, Yoshioka T, Jindan P, Kobayashi C, Suda H. The effect of endodontic procedures on apical crack initiation and propagation ex vivo. Int Endod J 2013; 46(8): 763-8. [ Links ]
8. Arias A, Lee YH, Peters CI, Gluskin AH, Peters OA. Comparison of two canal preparation techniques in the induction of microcracks: A pilot study with cadaver mandibles. JEndod 2014; 40(7):982-5. [ Links ]
9. Çiçek E, Kocak MM, Saglam BC, Kogak S. Evaluation of microcrack formation in root canals after instrumentation with different NiTi rotary file systems: A scanning electron microscopy study. Scanning 2015; 37(1): 49-53. [ Links ]
10. El Sayed MAAM, M'gharfaoui MR. Radicular dentinal defects incidence after using EDTA gel with different root canal instrumentation techniques. J Rest Dent 2015; 3(1): 21-5. [ Links ]
11. Pop I, Manoharan A, Zanini F, Tromba G, Patel S, Foschi, F. Synchrotron light-based pCT to analyse the presence of dentinal microcracks post-rotary and reciprocating NiTi instrumentation. Clinical Oral Investigation 2015; 19(1): 11-6. [ Links ]
12. Bürklein S, Tsotsis P, Schäfer Ε. Incidence of dentinal defects after root canal preparation: reciprocating versus rotary instrumentation. J Endod 2013; 39(4): 501-4. [ Links ]
13. Hin ES, Wu MK, Wesselink PR, Shemesh H. Effects of Self-Adjusting File, Mtwo and PrcTaper on the root canal wall. JEndod2013; 39(2): 262-4. [ Links ]
14. Bier CAS, Shemesh H, Tanomaru-Filho M, Wesselink PR, Wu MK. The ability of different nickel-titanium rotary instruments to induce dentinal damage during canal preparation. J Endod 2009; 35(2): 236-8. [ Links ]
15. Ashwinkumar V, Krithikadatta J, Surendan S, Velmurugan N. Effect of reciprocating file motion on microcrack formation in root canals: an SEM Study. Int EndodJ 2014; 47(7): 622-7. [ Links ]
16. Al-Zaka IM. The effects of canal preparation by different NiTi rotary instruments and reciprocating WaveOne file on the incidence of dentinal defects. Μ DJ 2012; 9(2): 137-42. [ Links ]
17. Milani AS, Froughreyhani M, Rahimi S, Jafarabadi MA, Paksefat S. The effect of root canal preparation on the development of dentin cracks. Iran Endod J 2012; 7(4): 177-82. [ Links ]
18. Adl A, Sedigh-Shams M, Majd M. The effect of using RC Prep during root canal preparation on the incidence of dentinal defects. J Endod 2015; 41(3): 376-9. [ Links ]
19. El Nasr HMA, El Kader KGA. Dentinal damage and fracture resistance of oval roots prepared with single-file systems using different kinematics. J Endod 2014; 40(6): 849-51. [ Links ]
20. Kansal R, Rajput A, Talwar S, Roongta R, Verma M. Assessment of dentinal damage during canal preparation using reciprocating and rotary files. J Endod 2014; 40(9): 1443-6. [ Links ]
21. Priya NT, Chandeasekhar V, Anita S, Tummala M, Raj TBP, Badami V, Kumar P, Soujanya E. "Dentinal microcracks after root canal preparation" A comparative evaluation with hand, rotary and reciprocating instrumentation. J Clin Diag Res 2014; 8(12): 70-2. [ Links ]
22. Ustun Y, Asian T, Sagsen B, Kesim B. The effects of different nickel-titanium instruments on dentinal microcrack formations during root canal preparation. Eur J Dent 2015; 9(1): 41-6. [ Links ]
23. Karunakaran JV, Kumar SS, Kumar M, Chandrasekhar S, Namitha D. The effects of various irrigating solutions on intra-radicular dentinal surface: A SEM analysis. J Pharm BioAllied Sei 2012; 4(6): 125-130. [ Links ]
24. Oliveira LD, Carvalho CAT, Nunes W, Valera MC, Carmango CHR, Jorge AOC, dos Campos SJ. Effects of Chlorhexidine and sodium hypochlorite on the microhardness of root canal dentin. Oral Surg.Oral Med Oral Pathol Oral Radiol 2007; 104(4): e125-e128. [ Links ]
25. Slutzky-Goldberg I, Maree Μ, Liberman R, Heling I. Effect of sodium hypochlorite on dentin microhardness. J Endod 2004; 30(12): 880-2. [ Links ]
26. Ulusoy OlA, Görgül G. 2013. Effects of different irrigation solutions on root dentine microhardness, smear layer removal and erosion. Aust Endod J 2013; 39(2): 66-72. [ Links ]
27. Kalluru RS, Kumar ND, Ahmed S, Sathish ES, Jayaprakash T, Garlapati R, Sowmya B, Reddy KN. Comparative evaluation of the effect of EDTA, EDTAC, NaOCI and MTAD on microhardness of human dentin-an in-vitro study. J Clin Diag Res 2014; 8(4): 39-41. [ Links ]
28. Eldeniz AU, Erdemir A, Belli S. Effect of EDTA and citric acid solutions on the microhardness and the roughness of human root canal dentin. J Endod 2005; 31 (2): 107-110. [ Links ]
29. Shemesh H, Bier CAS, Wu MK, Tanomaru-Filho M, Wesselink PR. The effects of canal preparation and filling on the incidence of dentinal defects. Int Endod J 2009; 42(3): 208-13. [ Links ]
30. Pasqualini D, Scotti N, Tamagnone L, Ellena F, Berutti E. Hand-operated and rotary ProTaper instruments: A comparison of working time and number of rotations in simulated root canals. J Endod 2008; 34(3): 314-17. [ Links ]
31. Kim HC, Lee MH. Yum J, Versluis A, Lee CJ, Kim BM. Potential relationship between design of nickel-titanium rotary instruments and vertical root fracture. J Endod 2010; 36(7): 1195-9. [ Links ]
32. Berutti E, Chiandussi G, Paulino DS, Scotti N, Cantatore G, Castelluccl A, Pasqualini D. Canal shaping with WaveOne primary reciprocating files and ProTaper System: A comparative study. J Endod 2012; 38(4): 505-9. [ Links ]
33. Capar ID, Arslan H, Akcay M, Uysal Β. Effects of ProTaper Universal, ProTaper Next, and HyFlex instruments on crack formation in dentin. J Endod 2014; 40(9): 1482-4. [ Links ]
34. Kim HC, Cheung GSP, Lee CJ, Kim BMK, Park JK, Kang SI. Comparison of forces generated during root canal shaping and residual stresses of three nickel-titanium rotary files by using a three-dimensional finite-element analysis. J Endod 2008; 34(6): 743-7. [ Links ]
35. Topcuoglu HS, Düzgün S, Kesim B, Tuncay O. Incidence of apical crack initiation and propagation during the removal of root canal filling material with ProTaper and Mtwo rotary nickel-titanium retreatment instruments and hand files. J Endod 2014; 40 (7): 1009-12. [ Links ]
36. Yang GB, Zhou XD, Zhang H, Wu HK. Shaping ability of progressive versus constant taper instruments in simulated root canals. IntEndod J 2006; 39(10): 791-9. [ Links ]
37. Adorno CG, Yoshioka Τ, Suda Η. The effect of root canal preparation technique and instrumentation length on the development of apical root cracks. JEndod 2009; 35(3): 389-92. [ Links ]
38. Imbeni I, Nalla RK, Bosi C, Kinney JH, Ritchie RO. In vitro fracture toughness of human dentin. J Biomed Mat Res 2003; 61(1): 1-9. [ Links ]
39. Giannini M, Soares CJ, de Carvalho RM. Ultimate tensile strength of tooth structures. Dental Materials 2004; 20(4): 322-9. [ Links ]
40. SiqueiraJF, Röcas IN, FavieriA, LimaKC. Chemo-mechanicalreduction of the bacterial population in the root canal after instrumentation and Irrigation with 1%, 2.5%, and 5.25% sodium hypochlorite. J Endod 2000; 26(6): 331-4. [ Links ]
41. Sim TPC, Knowles JC, Ng YL, Shelton J, Gulabiwala K. Effect of sodium hypochlorite on mechanical properties of dentine and tooth surface strain. Int Endod J 2001; 34(2): 120-32. [ Links ]
42. Butt N, Talwar S. In-vitro evaluation of various solvents for retrieval of mineral trioxide aggregate and their effects on microhardness of dentine. J Conserv Dent2013; 16(3): 199-202. [ Links ]
43. Zaparolli D, Saquy PC, Cruz-Filho AM. Effect of sodium hypochlorite and EDTA irrigation, individually and in alternation, on dentine microhardness at the furcation area of mandibular molars. Braz Dent J 2012; 23(6): 654-8. [ Links ]
44. Aslantas EE, Buzoglu HD, Altundasar E, Serper A. Effect of EDTA, sodium hypochlorite, and Chlorhexidine gluconate with or without surface modifiers on dentine microhardness. JEndod 2014; 40 (6): 876-9. [ Links ]
45. Marending Μ, Luder HU, Brunner TJ, Knecht S, Stark WJ, Zehnder M. Effect of sodium hypochlorite on human root dentine- mechanical, chemical and structural evaluation. Int Endod J 2007; 40 (10): 786-93. [ Links ]
46. Ari H, Erdemir A, Belli S. Evaluation of the effect of endodontic Irrigation solutions on the microhardness and the roughness of root canal dentin. JEndod 2004; 30(11): 792-5. [ Links ]
47. Marending Μ, Paqué F, Fischer J, Zehnder M.lmpact of irrigant sequence on mechanical properties of human root dentin. J Endod 2007; 33(11): 1325-28. [ Links ]
48. Tartarí Τ, Silva e Souza Pd-AR, de Almeida BVN, Silva Júnior JOC, Pessoa OF, Silva e Sousa Junior MH. A new weak chelator in endodontics: Effects of different irrigation regimens with Etidronate on root dentin microhardness. Int J Dent2013; 1-6. [ Links ]
49. Aranda-Garcia AJ, Kuga MC, Chavéz-Andrade GM, Kalatzis-Sousa NG, Duarte ΜΑΗ, Faria G, So MVR, Faria-Junior NB. Effect of final Irrigation protocols on microhardness and erosion of root canal dentin. Microsc Res Tech 2013; 76(10): 1079-83. [ Links ]
50. Pérez-Heredia Μ, Fener-Luque CM, González-Rodríguez MP, Martín-Peinado FJ, González-López S. Decalcifying effect of 15%EDTA, 15% citric acid, 5% phosphoric acid, and 2,5% sodium hypochlorite on root canal dentine. Int Endod J 2008; 41(5): 418-23. [ Links ]
51. Tuncer AK, Tuncer S, Siso SH. Effect QMix irrigant on the microhardness of root canal dentine. Aust DentJ 2015; (60): 1-5. [ Links ]
52. Taneja S, Kumari M, Anand S. Effect of QMix, peracetic acid and ethylenediaminetetra-acetic acid on calcium loss and microhardness of root dentine. JConserv Dent 2014; 17(2): 155-8. [ Links ]
53. Belli S, Eraslan O, Eskitascioglu M, Eskitascioglu G. Effects of NaOCI, EDTA and MTAD when applied to dentine on stress distribution in post-restored roots with flared canals. Int Endod J 2014; 47(12): 1123-32. [ Links ]
 Correspondence:
Correspondence:
Dr Suwayda Ahmed
Restorative Dentistry, Faculty of Dentistry
University of the Western Cape
Cissy Gool Avenue Rylands Estate
Cape Town, 7764
Tel no.: (021) 937 3091. 32
Email address: suahmed@uwc.ac.za

