










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Dental Journal
versión On-line ISSN 0375-1562
versión impresa ISSN 0011-8516
S. Afr. dent. j. vol.73 no.3 Johannesburg abr. 2018
RESEARCH
Head and neck cancers among HIV-positive patients: A five year retrospective study from a Johannesburg hospital, South Africa
Zwane NBI; Mohangi GUII; Shangase SLIII
IZwane Nompumelelo Benedicta. B Rad(Diagn.), BDS (MEDUNSA); MSSc(Dent) (Wits). Dentist/Lecturer, Department of Oral Medicine and Periodontology, School of Oral Health Sciences, University of the Witwatersrand, Johannesburg
IIMohangi Govindrau Udaibhan. MChD-OMP'(Pret). Specialist Consultant, Department of Oral Medicine and Periodontology, School of Oral Health Sciences, University of the Witwatersrand, Johannesburg
IIIShangase Sindisiwe Londiwe. BDS, MDent(MEDUNSA). Professor-Head of Department, Oral Medicine and Periodontology, School of Oral Health Sciences, University of the Witwatersrand, Johannesburg
ABSTRACT
INTRODUCTION: Cancer is a significant cause of morbidity and mortality among HIV infected individuals, but information is lacking in South Africa regarding Head and Neck AIDS-defining cancers (ADCs).
AIM To profile head and neck cancers (HNC) in HIV-positive patients in the Department of Oral Pathology, Wits Oral Health Centre over a five year period.
Methods and data analysis: A records-based retrospective descriptive study with an analytic component. Archived records (2009 to 2013) in the Department of Oral Pathology were reviewed. HIV serology results, CD4+T-cell counts and the viral load were verified from National Health Laboratory Service archived records. IBM SPSS 23.0 was used for data analysis.
RESULTS 1605 cases of HNC were recorded, with 389 (24.2%) confirmed HIV-positive ( mean age of 38 ± 11.0 years), of whom 52.3% were females . The likelihood of patients with HIV infection to be diagnosed with Kaposi Sarcoma (KS)and Non Hodgkin's Lymphoma(NHL) was significantly greater at 35.7% and 34.2% respectively with a p value < 0.05, compared with any other cancer type.
CONCLUSION: KS and NHL, both ADCs, were the two most common HNCs diagnosed among HIV-positive patients. Third was Oral squamous cell carcinoma (OSCC), a Non Aids Defining Cancer (NADC).
Keywords: Head and neck cancer; AIDS-defining cancer; Non-AIDS-defining cancer; Kaposi sarcoma; Non-Hodgkin's lymphoma; Oral squamous cell carcinoma.
INTRODUCTION
The human immunodeficiency virus (HIV) is an RNA retrovirus belonging to the Lentivirus subfamily. It is the cause of HIV infection. Since its discovery, HIV infection has spread at an alarming rate, more so in the resource-poor countries. In South Africa (SA) the number of people living with HIV was estimated at 6. 4 million during 2013 with 500 000 being new infections.1 By 2015 this figure had increased to 7 million, with a prevalence rate of 19.2% in adults aged 15 - 49 years.2 The most advanced stage of HIV infection is acquired immuno-deficiency syndrome (AIDS). AIDS is diagnosed when an individual has a CD4+ T-cell count of < 200 cells/mm3 and suffers opportunistic infections because of a suppressed immune system.3 AIDS still remains the number one cause of deaths in Africa and the second among young people globally.1 Oral lesions are a common finding in people infected with HIV,3 are often the presenting feature, and may predict a deteriorating immune system and a poor prognosis for the individual.4 The occurrence of these lesions may also predict HIV infection and herald a progression of HIV disease to AIDS.5,6 Cancer is another significant cause of morbidity and mortality in people infected with HIV, and is one of the recognised manifestations of the infection and progression of the individual to AIDS stage.7
There are cancers that are recognized to affect people infected with HIV, and are referred to as AIDS-defining cancers (ADCs) by the Centres for Disease Control (CDC). These cancers include Kaposi sarcoma (KS), non-Hodgkin's Lymphoma (NHL) and invasive cervical cancer (ICC). There are however, other types of cancers that appear more among HIV infected people compared with the general population but were not previously associated with HIV infection. These cancers are referred to as non-AIDS-defining cancers (NADCs) i.e. anal, lung, liver, kidney, testicular, Hodgkin's lymphoma (HL) and some head and neck cancers (HNC).8-10 Studies conducted mainly in resource-rich countries have demonstrated an increased incidence of NADCs among HIV infected individuals and a decline in ADCs, mainly after the introduction of antiretroviral therapy.11-13 For poorly resourced countries however, the same conclusion cannot be made because the incidence of ADCs is still high, even after antiretroviral therapy was introduced.14-17
This study aimed to identify and characterise the types of Head and Neck cancers (HNCs) histologically diagnosed in HIV-positive patients in the Department of Oral Pathology, Wits Oral Health Centre (WOHC), from 2009 to 2013. This was a period after the roll-out by state institutions in SA of highly active anti-retroviral therapy (HAART) to people infected with HIV who had CD4+T-cell counts < 350 cells/mm3.
MATERIALS AND METHODS
Study design
This was a records-based retrospective descriptive study with an analytical component, conducted at the Oral Pathology Department, Wits Oral Health Centre (WOHC). Permission to undertake the study was granted by WOHC and ethical clearance was obtained from the Human Research Ethics Committee of the University of the Witwatersrand (Ethical Clearance number: M140655).
Study population and sample
The study population consisted of all histologically diagnosed cases of HNC retained in the archives of the Oral Pathology Department from January 2009 - December 2013. A total sample of 1605 HNC cases was gathered. Confirmation of HIV seropositivity for the subjects was obtained from records of the National Health Laboratory Services (NHLS) of South Africa.
Statistical analysis
Data analysis was done using the IBM SPSS 23.0. Descriptive statistics of the measurements of central tendencies were used to determine the frequency, mean and standard deviation. Inferential statistics of binary and multinomial logistic regression were applied to determine the association between the independent variables (age, gender and HIV status) and the dependent variable (cancer diagnosis or type). Since the study sample size was already determined from the retrospective nature of the study, power calculations were done to minimize Type 2 errors when making comparisons. Statistical significance was inferred at p <0.05 for all analyses.
RESULTS
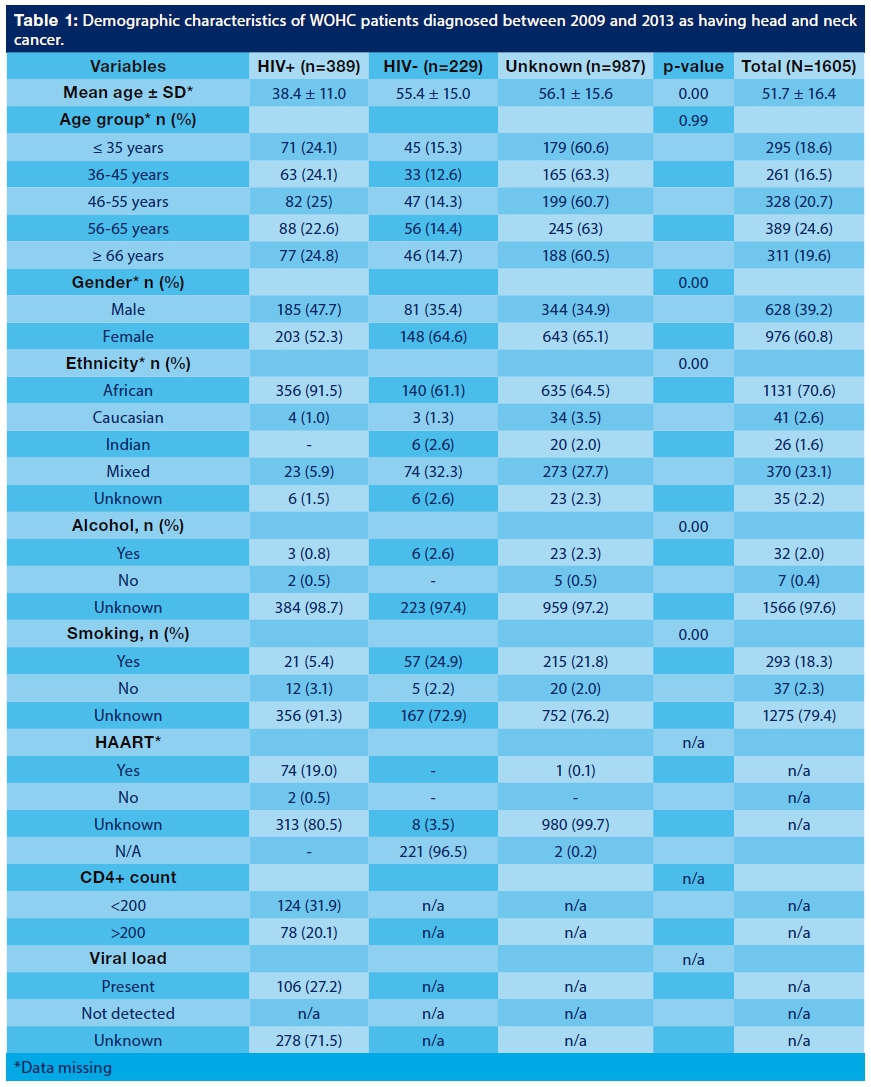
Of the 1605 recorded cases, 389 (24.2%) were confirmed as HIV-positive. The demographic characteristics of these cases are outlined in Table 1. From the remaining 1216 cases,229 (14.3%) were confirmed HIV- negative and 987 (61.5%) were unknown/unconfirmed cases. The mean age of the HIV-positive patients was 38±11 years with 46.1% lying in the 36 - 55 years age group. For the confirmed HIV-negative patients, the mean age was 52.1 ±16.9 and for the unconfirmed/unknown group, the mean age was 51.6±16.1. More females (52.3%) than males (47.7%) were confirmed as HIV-positive. HIV infection was notably higher among black patients (91.5%).
Head and neck cancers which were histologically diagnosed among HIV-positive patients included Kaposi sarcoma (KS), non-Hodgkin's lymphoma (NHL), Hodgkin's lymphoma (HL), Salivary gland tumours (SGTs), Oral squamous cell carcinoma (OSCC) and other types (nasopharyngeal cancer, basal cell carcinoma etc.). The most common HNC's diagnosed amongst HIV- positive cases were KS (35, 7%), NHL (34, 2%), and OSCC (19, 8%) (Figure 1). Hodgkin's lymphoma was diagnosed in 2.6% of HIV-positive cases and SGTs in only 1.0%.

The oral cavity was the most common anatomical site for head and neck cancer diagnosis (16.4%) followed by the larynx (15.3%), tongue (11.3%), jaws (11.2%), the palate (10.3%), neck (9.9%), the nasal cavity (7.5%), the lips (5.3%), the pharynx (4.6%), salivary glands (2.3%), ears (2.1%) and forehead (0.1%) (Figure 2). In some individuals the HNC's affected multiple sites (2.6%). The anatomical location was not specified in 0.8% of the cases.

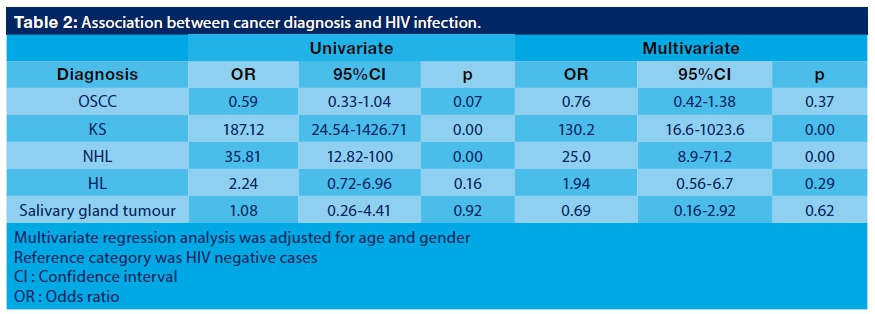
Univariate multinomial regression analysis of the data of the morphological type of cancer showed that the likelihood of patients with HIV infection to be diagnosed with KS and NHL was significantly higher at 35.7% and 34.2% respectively, with a p<0.001, compared with any other cancer type (Table 2).
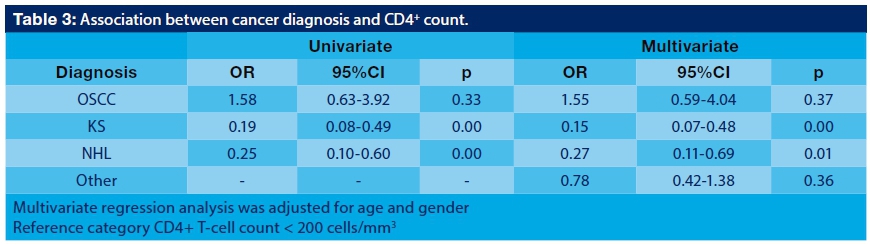
Multinomial regression analysis of cancer diagnosis showed a significant association with CD4+T-cell count in KS and NHL. The odds of a diagnosis of KS and NHL in HIV-positive patients with CD4+T-cell count > 200 cells/mm3 were increased by 0.19 and 0.25 respectively when compared with people with CD4+T-cell count < 200 cells/mm3 (p<0.001) (Table 3). Oral squamous cell carcinoma was found not to be an ADC.
DISCUSSION
This study aimed at identifying and characterizing HNCs which had been histologically diagnosed in the Department of Oral Pathology among patients infected with HIV.
Of the total number of cases sampled, 389 (24.2%) were confirmed HIV- positive. The remainder were either HIV-negative (14.3%) or diagnostically unconfirmed (61.5%) cases, even after an extensive search of the NHLS database.
The reasons for the excessive number of cases with an unknown HIV status are multifactorial, and these may be as follows: the lack of proper medical details for patients provided by the requesting clinicians, patients opting to go to the private sector or to public health facilities outside of their respective provinces for testing so as to remain anonymous and avoid stigmatization,18 older people presenting to public clinics only after becoming symptomatic21 and including socio-economic factors and the level of education affecting the community.33 More females (52.3%) were confirmed HIV-positive than males (47.7%) in this study. The high prevalence observed in women was also reported in other cohort studies conducted here in South Africa.14,18-21 One of the suggested reasons for this is the fact that women in general, and especially those of child- bearing age (15 - 49 years), have a higher participation in the free HIV counselling and testing (HCT) offered at state facilities than their male counterparts.20 Poverty also plays an important role especially when it comes to young women contracting the disease because of sexual interaction with older men in exchange for monetary gain.22 Women are also biologically more susceptible to HIV infection than males.22,23
Infection with HIV was notably higher in individuals younger than 35 years of age compared with those aged 36 to 55 years. Many reasons have been cited for this age group having such a high incidence, e.g. : most have "a higher level of education, reside in urban areas vs. rural areas and the fact that most females in this age group are in committed relationships and at child-bearing age, and are therefore frequent attenders at ante-natal clinics (ANC) and are regularly screened for HIV infection".24,25
Kaposi sarcoma (35.7%), non-Hodgkin's lymphoma (34.2%) and oral squamous cell carcinoma (19.8%) were the three most frequently diagnosed HNCs amongst HIV-positive patients in this sample. These results are similar to those of other studies carried out previously in Sub-Saharan Africa, indicating the elevated risks for KS and NHL among individuals diagnosed with HIV.14,19,21,26 KS and NHL are ADCs, according to the 1993 Centers for Disease Control classification (CDC). They are often associated with co-infections of oncogenic viruses; human herpes virus (HHV-8) for KS and Epstein-Barr virus (EBV) for NHL.27 Kaposi sarcoma was common in sub-Saharan Africa and South Africa even before HIV was discovered, and to a lesser extent was also seen in the Mediterranean countries like Italy, Greece and the Middle East.19 In SA the incidence of KS increased almost threefold between 1988 and 1996 and continued to rise as the HIV epidemic grew.20 Studies conducted in RSA and Rwanda found a definitive association between HIV infection and the development of KS with odds ratios (ORs) ranging from 21.9 to 47.1.26 KS is strongly linked with immunodeficiency, which means that the lower the CD4+T-cell count of an individual, the higher the risk of developing KS, although its occurrence remains a risk even in people with well-preserved cell counts.28 However, in this study the OR of an HIV-positive individual diagnosed with KS was found to be increased by 0.19, with a CD4+T-cell count of > 200 cells/mm3 compared with those with lower CD4+T-cell counts. A study conducted in KwaZulu-Natal, RSA, found similar results with 21% of the patients diagnosed with KS in their sample recording CD4+T-cell levels of > 350 cells/mm3.29 The reason behind these conflicting results, demonstrated between resource-rich against resource-poor countries, is not clearly understood. In the USA, Kaposi sarcoma incidence is associated with a declining CD4+T-cell count of < 200 cells/mm3, but in Africa it appears this is not necessarily true. Severe immune suppression is possibly not a prerequisite for the development of KS in African populations infected with HIV, given the early age at which the infection with HHV8 occurs in these regions.29
After the introduction of HAART in resource-rich countries, KS cases declined immediately.30 In SA however, KS prevalence among HIV-positive people remains high, despite the introduction of HAART to HIV-positive people with a CD4+T-cell count of < 200 cells/mm3 by state institutions across different provinces in April 2004.15,19 This study also found KS to be the most frequently diagnosed cancer (35.7%) amongst HIV infected people who had higher CD4+T-cell counts. Whether this high incidence of KS can be attributed to a possible immune reconstitution inflammatory syndrome (IRIS) or failure of HAART in these patients is not clear because the type of HAART regimen, the level of infection (CD4+T-cell count and RNA viral load count) as well as the time-frame between HIV diagnosis and the introduction of HAART to the patients could not be verified, leading to inconclusive results.
NHL was the second highest diagnosed cancer among HIV infected patients (34.2%). NHL is associated with a suppressed immune system in an individual. In one study three factors were significantly associated with the development of NHL in an individual namely: the age, the CD4+ T-cell count and no prior HAART.31 Studies conducted in Johannesburg, South Africa, found a strong association between HIV infection and NHL (OR = 5.0, 95%, CI = 2.7-9.5).19,32 Lymphoma cases studied from 2002-2009 in the Tygerberg area of the Western Cape, SA, were reported to be associated with HIV infection.34 The OR level at which an HIV infected person was associated with a diagnosis of NHL in this study was 0.25. Twenty-five of the 133 cases already on HAART had a CD4+T-cell count of > 200 cells/mm3. The increasing prevalence of cancer in resource-poor countries has been ascribed to the lack of sufficient HAART coverage in the population at risk for cancer, the type of HAART regimen provided or available in resource-poor countries and the higher prevalence of oncogenic viruses in these settings. These are possible reasons for the reduced impact that HAART has had in decreasing the rates of NHL and KS in Africa.17
OSCC (19.8%) was the third most commonly diagnosed cancer among HIV-positive patients in this study, but there was no significant correlation between that diagnosis and the CD4+T-cell count levels. Pro-oncogenic virus-related cancers and tobacco or alcohol-related cancers are common among HIV infected individuals because of the impaired immune surveillance.27,35,36 Missing information in the archives made it not possible to clarify how many of the OSCC cases in the current study were HPV-related or had a history of tobacco or alcohol usage. Only 5.4% of the HIV-infected individuals had a confirmed history of smoking and only 0.8% had a history of alcohol ingestion prior to diagnosis of the OSCC. The risk factors for developing OSCC among HIV infected individuals and the general population are the same and for this reason, OSCC has never been considered to be an ADC.37 In our study, OSCC was also not found to be an ADC.
The most involved sites for HNC in HIV-positive individuals were the larynx (19.2%) followed by the palate (16.5%) and the tongue (15.7%). In another study in South Africa laryngeal cancers were found only among 5.4% of HIV infected individuals.19 In Kenya, however, the larynx was reported as the most common site for HNC followed by the tongue, similar to the findings of the current study.38 The reasons for the varying anatomical sites from studies conducted in different regions of the continent are not clearly understood. Geographical location as well as sociocultural practices among people from these regions could possibly explain the dissimilarity in location of the cancer in the head and neck area.39
More studies are indicated to evaluate why the incidence of KS and NHL is not decreasing in SA; and there is a strong need for a wider, more effective distribution of HAART therapy. Better surveillance systems as well as population-based cancer registries are vital for this to happen and should be integrated with established HIV programs in South Africa and sub-Saharan Africa as a whole. It would be wise, as strongly indicated by knowledgeable and scientifically sound opinion, to ensure that HIV tests with CD4+ T-cell counts and viral loads are secured with informed consent from suspected HIV infected patients, wherever they are treated. This will assist with future studies in this particular field and will also improve the quality of services aimed at controlling and reducing the number of cancer cases and resultant deaths among HIV infected people.
LIMITATIONS OF THE STUDY
The limitations of the study were related to missing data, particularly the serology results for confirmation of the HIV status of the case subjects. Also, it was not possible to ascertain the temporal relationship between the histologic diagnoses of HNC and the tests/results for CD4+ T-cell count, including the RNA viral load.
CONCLUSION
Despite HAART being available from SA state institutions, the most commonly occurring HNCs in this region among the HIV-positive patients from 2009 to 2013 were still Kaposi sarcoma and Non-Hodgkin's lymphoma, both confirmed ADCs. These ADCs were diagnosed in patients with CD4+T-cell counts > 200 cells/mm3. The OSCC was found to be a NADC, and in this study was the third most commonly diagnosed cancer.
ACRONYMS
ADC : AIDS-defining cancer
AIDS : Acquired Immuno-deficiency Syndrome
ANC : ante-natal clinics
CDC : Centres for Disease Control
HAART : Highly Active Anti-retroviral Therapy
HNC : Head and neck cancer
ICC : invasive cervical cancer
IRIS : Immune Reconstitution Inflammatory Syndrome
KS : Kaposi sarcoma
NADC: Non-AIDS-defining cancer
NHL: non-Hodgkin's lymphoma
OSCC : Oral squamous cell carcinoma
SGT : Salivary gland tumour
WOHC : Wits Oral Health Centre
References
1. Unaids -Hiv And Aids Estimates (2015) www.unaids.org/en/regioncountries/countries/southafrica/ (accessed 04.04.2016) [ Links ]
2. Unaids/WHO Working Group on Global Hiv/Aids and Sti Surveillance (2015) - Monitoring HIV impact using population-based surveys. www.who.int/hiv/pub/surveillance/en/ (accessed 02.04.2016) [ Links ]
3. CDC. 1993 Revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. MMWR 1992;41(RR-17). [ Links ]
4. Scully C, Laskaris G, Porter SR, Reichart P. Oral manifestations of HIV infection and their management. 1. More common lesions. Oral Surg Oral Med Oral Pathol 1991; 71: 158 - 66. [ Links ]
5. Shangase L, Feller L, Blignaut E. Necrotizing ulcerative gingivitis/ periodontitis as indicators of HIV infection. South African Dental Journal 2004; 59(3): 105 - 8. [ Links ]
6. Coogan MM, Greenspan J, Challacombe S. Oral lesions in infection with human immunodeficiency virus. Bulletin of the World Health Organisation 2005; 700 -6. [ Links ]
7. Newcomb-Fernandez J. Cancer in the HIV-infected population. Res. Initiat. Treat. Action 2003; 9: 5 -13 [ Links ]
8. Barbaro G, Barbarini G. HIV infection and cancer in the era of highly active antiretroviral therapy (Review). Oncology Reports 2007; 17: 1121 - 6. [ Links ]
9. Silverberg MJ, Leyden WA, Horberg MA, et al. HIV Infection and the risk of cancers with and without a known infectious cause. AIDS 2009; 23(17): 2337 - 45. [ Links ]
10. Deeken JF, Tjen-A-Looi A, Okuliar C, Young M, et al. The rising challenge of Non-AIDS-Defining Cancers in HIV-infected patients. J Clinical Infectious Diseases 2012; 55: 1228 -35. [ Links ]
11. Engels EA, Biggar RJ, Hall I, et al. Cancer risk in people infected with Human Immunodeficiency Virus in the United States. J International Cancer 2008; 123: 187 - 94. [ Links ]
12. Engels EA. Non-AIDS-defining malignancies in HIV-infected persons: etiologic puzzles, epidemiologic perils, prevention opportunities. AIDS 2009; 23(8): 875- 85. [ Links ]
13. Cobucci RNO, Lima PH, de Souza PC, et al. Assessing the impact of HAART on the incidence of defining and non-defining AIDS cancers among patients with HIV/AIDS: A systematic review. J Infect Public Health 2014; 367: 1 - 10. [ Links ]
14. Stein L, Urban MI, Sitas F, et al. The spectrum of human immunodeficiency virus-associated cancers in a South African black population: Results from a case-control study, 1995-2004. International Journal of Cancer 2008; 122: 2260 -5. [ Links ]
15. Sasco AJ, Jaquet A, Boidin E, et al. The challenge of AIDS-related malignancies in sub-Saharan Africa. PLos ONE 2010; 5(1): e8621. [ Links ]
16. Mbulaiteye SM, Bhatia K, Adebamowo C, Sasco AJ. HIV and cancer in Africa: mutual collaboration between HIV and cancer programs may provide timely research and public health data. Infectious Agents and Cancer 2011; 6: 16. [ Links ]
17. Casper C. The increasing burden of HIV-associated malignancies in resource-limited regions. Annual Reviews of Medicine 2011; 62: 157 - 70. [ Links ]
18. Snow RC, Madalane M, Poulsen M. Are men testing? Sex differentials in HIV testing in Mpumalanga Province, South Africa. AIDS Care 2010; 22(9): 1060 - 5. [ Links ]
19. Sitas F, Pacella-Norman R, Carrara H, et al. The spectrum of HIV-1 related cancers in South Africa. International Journal of Cancer 2000; 88: 489 - 92. [ Links ]
20. Tabana H, Doherty T, Swanevelder S, et al. Knowledge of HIV status prior to a community HIV counselling and testing intervention in a rural district of South Africa: results of a community based survey. BMC Infectious Diseases 2012; 12: 73 - 80. [ Links ]
21. Sengayi M, Babb C, Egger M, Urban M. HIV testing and burden of HIV infection in black cancer patients in Johannesburg, South Africa: a cross-sectional study. BMC Cancer 2015; 15: 144 - 5. [ Links ]
22. Pettifor AE, Hudgens MG, Levandowski BA, et al. Highly efficient HIV transmission to young women in South Africa. AIDS 2007; 21: 861 - 5. [ Links ]
23. Williams BG, Gouws E, Colvin M et al. Patterns of infection: using age prevalence data to understand the epidemic of HIV in South Africa. South African Journal of Science 2000; 96: 305 -11. [ Links ]
24. Peltzer K, Matseke G, Mzolo T, Majaja M. Determinants of knowledge of HIV status in South Africa: results from a population based HIV survey. BMC Public Health 2009; 9: 174 - 85. [ Links ]
25. McPhail C, Pettifor A, Moyo W, Rees H. Factors associated with HIV testing among sexually active South African youth aged 15-24 years. AIDS Care 2009; 21(4): 456 - 67. [ Links ]
26. Newton R, Ziegler J, Beral V, et al. A case-control study of Human Immunodeficiency Virus infection and cancer in adults and children residing in Kampala, Uganda. International Journal of Cancer 2001; 92:622 - 7. [ Links ]
27. Mbulaiteye SM, Katabira ET, Wabinga H, et al. Spectrum of cancers among HIV-infected persons in Africa: The Uganda AIDS-Cancer Registry Match Study. International Journal of Cancer 2006; 118: 985 - 90. [ Links ]
28. Baker JV, Peng G, Rapkin J, et al. CD4+ count and risk of non-AIDS diseases following initial treatment for HIV infection. AIDS 2008; 22:841 - 8. [ Links ]
29. Mosam A, Hurkchand HP, Cassol E, et al. Characteristics of HIV-1-associated Kaposi's sarcoma among women and men in South Africa. International Journal of STD & AIDS 2008; 19: 400 -5. [ Links ]
30. Grulich AE. Cancer: the effects of HIV and antiretroviral therapy, and implications for early antiretroviral therapy initiation. Current Opinion in HIV and AIDS 2009; 4: 183 - 7. [ Links ]
31. Bower M, Nelson M, Young AM, et al. Immune Reconstitution Inflammatory Syndrome associated with Kaposi's sarcoma. Journal of Clinical Oncology 2005; 23(22): 5224 - 8. [ Links ]
32. Sitas F, Bezwoda WR, Levin V, et al. Association between human immunodeficiency virus type 1 infection and cancer in the black population of Johannesburg and Soweto, South Africa. British Journal of Cancer 1997; 75(11): 1704 - 7. [ Links ]
33. Mbulaiteye SM, Parkin DM, Rabkin CS. Epidemiology of AIDS-related malignancies - An international perspective. Haematol Oncol Clin N Am. 2003; 17: 673 -96. [ Links ]
34. Abayomi EA, Somers A, Grewal R, et al. Impact of the HIV epidemic and Anti-Retroviral Treatment policy on lymphoma incidence and subtypes seen in the Western Cape of South Africa, 2002 - 2009. Transfus Apher Sci. 2011; 44(2): 161 - 6. [ Links ]
35. Silverberg MJ, Chao C, Leyden WA, et al. HIV infection, immunodeficiency, viral replication, and the risk of cancer. Cancer Epidemiol Biomarkers Prev. 2011; 20(12): 2551 - 9. [ Links ]
36. Franzetti M, Adorni F, Parravicinic C, et al. Trends and predictors of non- AIDS-defining cancers in men and women with HIV infection: A single-institution retrospective study before and after the introduction of HAART. J Acquired Immune Deficiency Syndrome 2013; 62: 414 -20. [ Links ]
37. D'Souza G, Carey TE, William WN, Jr., et al. Epidemiology of head and neck squamous cell cancer among HIV-infected patients. J Acquired Immune Deficiency Syndrome 2014; 65(5): 603 - 10. [ Links ]
38. Onyango JF, Macharia IM. Delays in diagnosis, referral and management of head and neck cancer presenting at Kenyatta National Hospital, Nairobi. East African Medical Journal 2006; 83(4): 85 - 91. [ Links ]
39. Gilyoma JM, Rambau PF, Masalu N, et al. Head and neck cancers: a clinic-pathological profile and management challenges in a resource-limited setting. BMC Res Notes 2015; 8:772. [ Links ]
 Correspondence:
Correspondence:
Shangase S.L.
Oral Medicine and Periodontology, School of Oral Health Sciences
University of the Witwatersrand
Johannesburg
Tel: 011 488- 4887. Fax: 011 488- 4902 /086 207- 4358 Cell: 072 395- 2335
e-mail: sindisiwe.shangase@wits.ac.za


{kind=link}
{kind=link}
{kind=link}