










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.72 n.8 Johannesburg Sep. 2017
http://dx.doi.org/10.17159/2519-0105/2017/v72no8a8
CLINICAL WINDOWS
What's new for the clinician? Summaries of and excerpts from recently published papers
Jeff Yengopal
BChD, MChD (Community Dentistry) Stellenbosch. Department of Community Dentistry, School of Oral Health Sciences, University of the Witwatersrand. E-mail: Veerasamy.Yengopal@wits.ac.za
1. Antimicrobial photodynamic therapy vs. local minocycline in addition to non-surgical therapy of deep periodontal pockets: a controlled randomized clinical trial.
Tabenski, L, Moder, D., Cieplik, F. et al.. Clin Oral Invest; 2017: 21: 2253 - 2264
Periodontal disease results from inflammation of the supporting structure of the teeth and in response to chronic infection caused by various periodontopathic bacteria. In the treatment of periodontally involved teeth, current concepts are based on mechanical scaling and root planing (SRP) to remove bacterial deposits, calculus, and cementum contaminated by bacteria and endotoxins.1 However, the efficacy of mechanical non-surgical debridement is limited in areas difficult to reach by instruments, e.g., furcation lesions or deep narrow intrabony defects.1 The subgingival application of antiseptic rinsing solutions, e.g., chlorhexidine digluconate or povidone-iodine, additionally to SRP, has shown significant improvements on clinical healing parameters.1 However, in progressive periodontal disease and residual deep periodontal pockets, antiseptic solutions seem not effective enough for bacterial elimination.
Photodynamic therapy (PDT) has emerged in recent years as a non - invasive therapeutic modality for the treatment of various infections by bacteria, fungi, and viruses. PDT can be applied topically into a periodontal pocket, avoiding overdoses and side effects associated with the systemic antimicrobial agent administration. It also minimizes the development of bacterial resistance.1 Photodynamic antimicrobial chemotherapy represents an alternate antibacterial, antifungal, and antiviral treatment against drug - resistant organisms.1 Applications of PDT in dentistry are growing rapidly. The technique is also used in the treatment of oral cancer, bacterial and fungal infections, and in the photodynamic diagnosis of the malignant transformation of oral lesions.1
During the last decade, antimicrobial PDT has become an accepted therapy for biofilm-induced diseases in several medical disciplines. The therapy requires in the first instance that a photosensitizer binds to the target cells. Activation with light of a suitable wavelength results in the generation of singlet oxygen and reactive oxygen species, which are toxic to the target cells or microorganisms.
Tabenski and colleagues from Germany (2017)1 reported on a trial that sought to investigate the additional influence of antimicrobial (aPDT) vs. local application of minocycline microspheres following non-surgical periodontal therapy in deep periodontal pockets. The scientific rationale was to find an effective procedure to treat deep periodontal defects whilst avoiding the use of antibiotics or surgical interventions.
MATERIALS AND METHODS
For inclusion into this 12 month parallel randomized control trial, patients had to have good health; be >35 years old;1 have a minimum of 16 residual teeth; have untreated generalized moderate to severe chronic periodontitis with a minimum of four teeth having probing pocket depth (PPD) >6 mm, an approximal plaque index (API) >25% and a papillary bleeding index (PBI) <25%. Heavy smokers, those with uncontrolled medical conditions, or pregnant or those having aggressive periodontitis or having periodontal treatment during the last 3 months were excluded.
The study comprised three randomly selected groups of 18 patients each. Each patient was periodontally treated within one session. In all three groups, SRP was carried out using a sonic scaler and Gracey curettes. This was followed by a PDT in the test group (aPDT + SRP). The photosensitizer was based on phenothiazinium chloride. Activation was achieved through application of a laser beam generated by a handheld diode laser with a laser wavelength of 670 nm and an irradiance of 75mW/cm2. The dye was applied subgingivally for three min. After rinsing with 0.9% sodium chloride solution, the pocket was exposed to the laser light by using a fibre optic application for ten seconds at six sites per tooth (1 min per tooth). In accord with the manufacturer's instructions, this procedure was repeated after seven days. In the positive control group (MC + SRP), all teeth with PPD >6 mm received an additional application of one-unit dosage of minocycline (MC) hydrochloride microspheres. Patients of the negative control group (SRP-alone) received no further treatment beside SRP. For the investigation, each patient contributed four experimental teeth: one tooth of each quadrant with the deepest periodontal pocket but at least with PPD = six mm and bleeding upon probing (BOP) at baseline. The following clinical parameters were assessed at baseline as well as at six weeks, three months, six months, and 12 months after active periodontal therapy: Approximal plaque index (API); papillary bleeding index (PBI) bleeding on probing (BOP), probing pocket depth (PPD), and clinical attachment level (CAL) were recorded at six sites per tooth.
Following periodontal treatment, all patients were instructed to continue their regular daily oral hygiene and to rinse with a 0.2% chlorhexidine solution for 1 min twice a day for the following 5 days. Patients in the positive control group (MC + SRP) had to avoid mechanical plaque control for the first 12 hours and to discontinue subgingival flossing for the first 10 days to avoid mechanical removal of the minocycline.
Supportive periodontal therapy was performed six weeks as well as three six, nine and 12 months after subgingival periodontal treatment in every patient. At these time-points, the compliance of the patients with good oral hygiene was controlled. If necessary, oral hygiene reinstructions were given and all teeth were cleaned and polished supragingivally. Additionally, the indices API, PBI, and BOP were recorded sixweeks, three, six and 12 months after subgingival periodontal treatment. To avoid any interference with the effect of the initial active treatment phase, subgingival re-instrumentation had to be avoided during the 12-month study period as far as was ethically possible. Only in cases of massive signs of inflammation (pain, suppuration, extensive bleeding on probing) was re-treatment indicated. In this case, in the individual patient, the same treatment protocol had to be applied as in the initial active treatment phase and had to be reported.
All examiners in this trial were blinded to the therapy method used in the individual patient.
For the microbial evaluation, subgingival microbiological samples were obtained from the deepest site of each of the four experimental teeth per patient at baseline, as well as at six weeks, three months, six months, and 12 months after subgingival therapy. The samples were analyzed for Aggregatibacter actinomycetemcomitans (A.a.), Porphyromonas gingivalis (P.g.), Tannerella forsythia (T.f.), and Treponema denticola (T.d.). Furthermore, the total marker load (TML: number of periodontal pathogens related to the total number of bacteria in the sample) and the total bacterial load (TBL: total amount of bacteria in the sample) were determined.
RESULTS
While for the SRP-alone group 18 patients could be recruited, for the aPDT + SRP and MC + SRP groups, only 15 patients could be followed over the study period. Thus,for symmetry reasons, only 45 patients (age range 54-57) were included for data analysis. The evaluations of the clinical and microbiological healing outcomes are based on only the four experimental teeth (PPD >6 mm) from each patient. After the six-month evaluation and in one patient each of the MC + SRP and SRP-alone groups, one experimental tooth was lost due to prosthodontic reasons. During the entire study period, the researchers could not observe any signs of adverse reactions related either to aPDT or minocycline (MC) application.
With exception of the API, none of the other healing parameters (PBI, BOP, PPD, CAL) revealed any statistically significant differences between the three treatment groups at any time-point. During the periodontal maintenance, none of the 45 patients required subgingival re-instrumentation, which would have been performed according to the study protocol. Thus, the reported healing results describe the effects of the initial active treatment.
After completion of the pre-treatment phase, all patients showed an acceptable compliance with good oral hygiene at baseline. While in the MC + SRP group and in the SRP-alone group the API was below the threshold of 25%, in the aPDT + SRP group, a median API of 29% had to be accepted. However, the long-term parameter for good oral hygiene, the PBI, was by far below the threshold of 25% in all therapy groups. With regard to the API, the aPDT + SRP group showed significantly less plaque compared with the MC + SRP group after six weeks, three months, and six months. Twelve months after treatment, both the aPDT + SRP group and the SRP-alone group had significantly better oral hygiene status than the MC + SRP group. However, all patients could maintain relatively low plaque and gingivitis scores during the entire study period.
At baseline, in each group, the median percentage of BOP-positive experimental teeth was 100%. Compared with baseline, a statistically significant reduction of BOP-positive experimental teeth was found for each group during the 12-month period. No statistically significant differences could be found between the three treatment groups. After six weeks, 50% of the experimental teeth in the aPDT + SRP and MC + SRP groups as well as 75% of experimental teeth in the SRP-alone group still bled on probing. After three months, the percentage of BOP-positive experimental teeth was reduced to 50% in each group. At six months, bleeding was found in 25% of the experimental teeth in the aPDT + SRP group and in 50% of the experimental teeth in the MC + SRP and SRP-alone groups. After 12 months, BOP values increased again significantly in the aPDT + SRP and SRP-alone groups and remained stable in the MC + SRP group, considering that one experimental tooth each was lost in the MC + SRP and SRP-alone groups after the six-month examination (aPDT + SRP 75%, MC + SRP 33.3%, SRP-alone 66.7%).
There were no statistically significant differences between the three groups at baseline for PDD. During the 12-month study period, the three treatment modalities achieved statistically significant reductions in PPD at each follow-up compared to baseline. At no time-point and no examination interval, were any statistically significant differences found between the three groups.
At baseline, there were no significant differences in CAL between the three groups. Statistically significant CAL improvements were observed in each group during the 12-month study period with no statistically significant differences between the three groups at any examination time-point or interval.
The bacterial strain A.a. was detected only in very few sites with no clinical or statistical relevance. For T.d., T.f., and P.g. and for TBL and TML, the three groups showed a similar bacterial load at baseline. In the MC + SRP group, significantly less T.f. were found after 6 weeks compared to the aPDT + SRP group. After three months, the SRP-alone group revealed significantly less P.g. compared to the aPDT + SRP group. For all other bacterial species and time-points, no significant differences were found between the groups. The reduction of the bacterial load over time was statistically significant for P.g. in each group at every follow-up compared with baseline with the exception of the 12-month time-point in the SRP-alone group. For T.f., a statistically significant reduction at each examination time-point was found in each group with exception of the three-month time-point in the MC + SRP group. For T.d., a statistically significant reduction could be detected in the aPDT + SRP group only after six months; in the MC + SRP group after six weeks, three months, and six months; and in the SRP-alone group at the three-, six-and 12-month examination time-point. The total bacterial load was significantly reduced in the aPDT + SRP group and the MC + SRP group after six weeks and 12 months and in the SRP-alone group at each follow-up. The total marker load was significantly reduced in the aPDT + SRP group six weeks and three months after treatment, in the SRP-alone group three and six months after treatment, and in the MC + SRP group at each examination time-point.
CONCLUSIONS
Within the limits of this clinical study, , all three treatment modalities (aPDT + SRP, MC + SRP, SRP-alone) achieved statistically significant clinical and microbiological improvements over time in deep periodontal pockets (PPD >6 mm). However, the additional use of aPDT or minocycline failed to show any significant additional positive effects compared with SRP alone in deep periodontal pockets.
IMPLICATIONS FOR PRACTICE
This trial showed that the new interventions tested showed no additional benefit over the standard approach of SRP in patients with periodontitis. Clinicians should note that the small sample size may have masked the true treatment effects.
ACRONYMS
API: Approximal Plaque Index
BOP: bleeding upon probing
MC: minocycline (MC) hydrochloride microspheres
PBI: papillary bleeding index
PDT: Photodynamic therapy
PPD: probing pocket depth
SRP: scaling and root planing
TBL: total amount of bacteria in the sample
TML: total marker load
Reference
1. Tabenski, L, Moder, D, Cieplik, F. et al. Antimicrobial photodynamic therapy vs. local minocycline in addition to non-surgical therapy of deep periodontal pockets: a controlled randomized clinical trial. Clin Oral Invest; 2017: 21: 2253 - 2264. [ Links ]
2. Effects of photodynamic therapy in periodontal treatment: A randomized, controlled clinical trial
Segarra-Vidal M, Guerra-Ojeda S, Vallés LS, et al. J Clin Periodontol. 2017;44:915-925
Scaling and root planing (SRP) is the gold standard for reducing biofilm in nonsurgical management of periodontal disease.1 However, SRP is not able to remove all periodontal pathogenic bacteria, particularly those found within periodontal tissues or in deep periodontal pockets. As a result, bacterial recolonization occurs from the non-eliminated subgingival plaque or from other oral reservoirs.1 Photodynamic therapy (PDT) has been introduced as a noninvasive intervention which is based on the use of a photosensitizing agent that is activated by light of an adequate wavelength. In the presence of oxygen, this generates free radicals and singlet oxygen, which have been found to be toxic to bacteria.1 However, there is no agreement to date on the benefits of PDT as a co-adjuvant to SRP. Segarra-Vidal and colleagues from Spain (2017)1 reported on a trial that sought to assess additional clinical, microbiological and biochemical effects of PDT in the initial management of chronic periodontitis. The null hypothesis was that PDT as a co-adjuvant therapy would result in improved basic periodontal management.
MATERIALS AND METHODS
Forty patients (12 men and 28 women) between 33 and 74 years of age (mean 55 ± 2) with chronic periodontitis took part in this study. Inclusion criteria for this trial was: four or more periodontal pockets with a probing depth >5 mm and bleeding on probing. Patients who had undergone periodontal, antibiotic, photosensitizing or anticoagulant treatment in the last three months, were smokers, had a Silness and Löe plaque index of 2 for more than 30% of the teeth, were pregnant or breastfeeding, or were allergic to the components used in the treatments, were excluded. The patients were divided into two groups of 20 individuals according to the type of treatment prescribed. One group underwent basic periodontal treatment consisting of scaling and root planing (SRP group); the second group underwent this basic periodontal treatment plus photodynamic therapy (SRP + PDT group). A third group consisted of 20 systemically and periodonally healthy individuals (control group) recruited during routine periodical checkups, who were monitored only once during the screening visit, at the same time as the other two groups.
A randomized, single-blind, controlled design was used. Simple randomization of the patients (1:1 allocation ratio) to the SRP or SRP + PDT group was carried out by staff external to the study using a computer-generated random number table. Blinding to the randomization was ensured using sealed and opaque envelopes numbered in sequence.
The calculated required sample size was 40 patients. This sample size was determined to provide 90% power in recognizing a significant difference in the clinical attachment level of 0.75 mm between groups, with a standard deviation of 1.5 (d = 0.5) and a 95% confidence interval (α = 0.05).
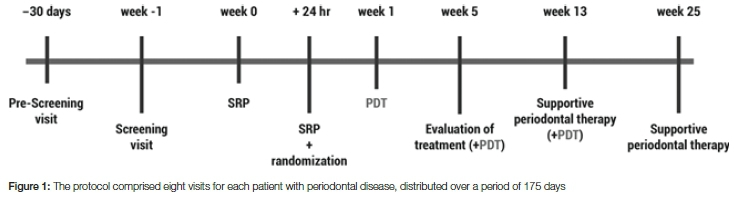
The protocol comprised eight visits for each patient with periodontal disease, distributed over a period of 175 days as shown in Figure 1.
A blinded examiner conducted a periodontal evaluation of the patients at six sites per tooth. In addition, four samples of gingival crevicular fluid were collected, always at the same locations (probing depth >5 mm and bleeding on probing), during the screening visit and after five, 13 and 25 weeks. Samples were collected from the control group on a single occasion.
Both study groups underwent SRP with combined ultrasound and the use of Gracey and Columbia curettes under local anaesthesia at week 0 and 24 hours later. The randomization envelope was opened after SRP was completed (week 0 + 24 hr). Supporting periodontal treatment-consisting of SRP, with reinforcement of brushing techniques, including the use of interproximal hygiene measures-was performed at weeks 13 and 25.
In addition to SRP, the patients in the SRP + PDT group received co-adjuvant PDT using the Periowave® system. Methylene blue at a concentration of 0.005% was used as a photosensitizing agent and was applied following the instructions of the manufacturer using a blunt needle over the periodontal pocket. Diode laser irradiation (670 nm, 150 mW) was carried out with a flexible tip for 60 seconds in each periodontal pocket (depth > 5 mm). The treatment was applied at weeks one, five and 13.
All patients received instructions on proper toothbrushing. Reinforcement of these instructions was carried out during each visit.
Clinical parameters were recorded at six sites per tooth by a single calibrated examiner who was blinded to the type of treatment received by the patient. Clinical parameters for each patient was monitored in the following order:
1. gingival crevicular fluid;
2. plaque index;
3. probing depth;
4. clinical recession;
5. clinical attachment level;
6. bleeding on probing.
Comparison of the treatments was performed at critical sites, defined as sites at which the periodontal pocket measured >5 mm in depth with bleeding on probing at the screening visit. The effective study sample, therefore, comprised 809 data points (381 corresponding to SRP and 428 to SRP + PDT).
Probing depth was measured in millimetres from the gingival margin to the depth of the periodontal pocket. Clinical recession in turn was measured in millimetres from the gingival margin to the cementoenamel junction. The clinical attachment level was measured in millimetres from the cementoenamel junction to the end of the pocket. Bleeding on probing was documented according to the absence or presence of bleeding 30 seconds after probing. Improvement in the clinical attachment level was regarded as the primary endpoint. Secondary endpoints were improvement in probing depth and reduction of bleeding on probing, clinical recession and the plaque index.
Microbiological and biochemical samples were taken before any subgingival instrumentation was carried out. Following the removal of supra-gingival plaque and calculus using periodontal curettes, gingival crevicular fluid samples were pooled during the screening visit and at weeks five, 13 and 25 from four experimental sites, namely, the deepest periodontal pocket in each quadrant (probing depth >5 mm, accompanied by bleeding on the screening visit) was considered to be representative of the entire oral cavity. Samples for microbiological analysis were obtained by inserting a sterile number 30 paper endodontic tip (Dentsply®, Maillefer) into the bottom of the periodontal pocket for 10 seconds; a sterile Periopaper® strip (Oralflow®) was inserted for 30 seconds in the case of sampling for biochemical analysis. Samples containing blood or plaque were rejected. The gingival crevicular fluid volume was recorded using Periopaper® strips with a Periotron 8000® (Oralflow®). The samples were stored at -80°C in sterile Eppendorf® tubes until processing.
For the healthy control group, a single sampling was performed in the groove between distal-vestibular teeth 1.2 and 2.2 and mesio-vestibular teeth 1.6 and 2.6. Both samples were pooled and treated as described above.
Gene expression levels of the main bacteria implicated in chronic periodontitis
(Aggregatibacter actinomycetemcomitans, Tannerella forsythia, Porphyromonas gingivalis, Treponema denticola, Prevotella intermedia and Campylobacter rectus) in gingival crevicular fluid using real-time polymerase chain reaction (RT-PCR) was determined. Commercial enzyme-linked immunosorbent assay (ELISA) kits were used for the determination of biochemical markers.
RESULTS
Thirty-seven patients (26 women and 11 men, with a mean age of 55 ± 2 years) completed the six month trial. At baseline, the clinical attachment level was 6.19 ± 1.42 mm in the SRP group and 6.47 ± 1.60 mm in the SRP + PDT group (p > .05). These values decreased over time, independent of the treatment received (4.19 ± 1.60 mm and 4.67 ± 1.83 mm for SRP and SRP + PDT, respectively; p > .05). Secondary clinical parameters improved in both groups, with the exception of clinical recession, which increased significantly in both groups. No significant differences were noted between treatments. At baseline, the mean gingival crevicular fluid volume in the SRP group was 0.62 ± 0.40 μl, compared with 0.55 ± 0.37 μl in the SRP + PDT group (p > .05). The corresponding mean volume in the healthy controls was significantly lower than that in the patients with periodontal disease (0.18 ± 0.05 μl; p < .001). The gingival crevicular fluid volume in the patients with periodontal disease decreased over time, with no significant differences between treatments and without reaching the control values at the end of the study.
Compared with the control group, the patients with periodontal disease showed increased bacterial burden corresponding to A. actinomycetemcomitans, P. gingivalis, T. forsythia, T. denticola, P. intermedia and C. rectus at the screening visit. Although SRP treatment alone did not alter the pathogenic burden of A. actinomycetemcomitans, the addition of PDT significantly lowered the abundance of this species (p < .001) to levels consistent with those of the healthy individuals. Both SRP and SRP + PDT were found to be effective at lowering the bacterial burden of P. gingivalis and T. forsythia to levels similar to those in the controls, without significant differences between treatments. Conversely, neither treatment modified the T. denticola, P. intermedia or C. rectus burden, which remained higher than that of the control group at the end of the study.
At baseline, pro-inflammatory cytokine (IL-1 ß, IL-6 and TNF-α) levels in the gingival crevicular fluid of the patients with periodontal disease were higher than those in the control group. Independent of the treatment received, the TNF-a and IL-1 ß concentrations decreased, reaching values similar to those in the controls, though there were no changes in IL-6, which remained at an elevated level at the end of treatment.
Regarding bone metabolic markers, by the end of the study, both treatments resulted in similar non-significant levels/ratios (p > .05).
CONCLUSIONS
The authors concluded that PDT did not provide additional benefits in terms of clinical attachment level or any secondary clinical outcome compared with the effects of SRP. Clinical improvement was consistent with a decrease in the concentrations of cytokines and biochemical markers. Based on the findings of this trial, the authors did not support the use of PDT as a co-adjuvant in the treatment of moderate-to-severe chronic periodontitis.
IMPLICATIONS FOR PRACTICE
This study adds to the weight of evidence that suggests that PDT is not useful in the treatment of moderate-to-severe-periodontitis.
ACRONYMS
PDT: Photodynamic therapy
SRP: Scaling and root planing
Reference
1. Segarra-Vidal M, Guerra-Ojeda S, Vallés LS, et al. Effects of photodynamic therapy in periodontal treatment: A randomized, controlled clinical trial. J Clin Periodontol. 2017;44:915-925. [ Links ]


{kind=link}