










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.72 n.7 Johannesburg Aug. 2017
RESEARCH
A BhayatI; TK MadibaII
IBDS, MSc, MPH, M Dent (Community Dentistry). Department of Community Dentistry, School of Dentistry, Faculty of Health Sciences, University of Pretoria, South Africa
IIB.Dent Ther, BDS, DHSM, MChD (Community Dentistry). Department of Community Dentistry, School of Dentistry, Faculty of Health Sciences, University of Pretoria, South Africa
SUMMARY
Dental caries is one of the most common childhood diseases, affecting up to 80% of all individuals at some stage of their lives. It is a debilitating and painful condition which impacts on mastication, speech, aesthetics and psychosocial behaviour. The prevalence of caries in South African children is around 40% and almost half of this burden goes untreated. The end results are pain, swelling and abscess formation, all of which have negative effects on aspects of the lives of the patients.
Although dental caries is preventable, the prevalence continues to remain relatively high.
This paper discusses the spread of caries and some of the methods by which it can be reduced and/or prevented.
INTRODUCTION
Dental caries (DC) can be defined as the localized destruction of dental hard tissues due to acidic by-products arising from bacterial fermentation of dietary carbohydrates.1 Although DC is one of the most common preventable childhood diseases, individuals and communities are susceptible to the disease throughout their lifetime.1,2 DC is classified according to the site of the tooth on which it occurs (occlusal, interproximal and root) and the number of teeth it affects (rampant or localized). In young children, early childhood caries (ECC) is very common, as shown in Figures 1 and 2 and the high incidence may be attributed to poor diet and poor oral hygiene practices.1


DC, as with many other diseases, depends on the state of balance between the attacking agents, which cause the initial lesion and acquired factors which modify the susceptibility or resistance of the tissues. In caries, the balance is between the character of the enamel and the modifying resisting factors, which are present in the immediate environment of the teeth, the plaque and the saliva.3
Aetiology of dental caries
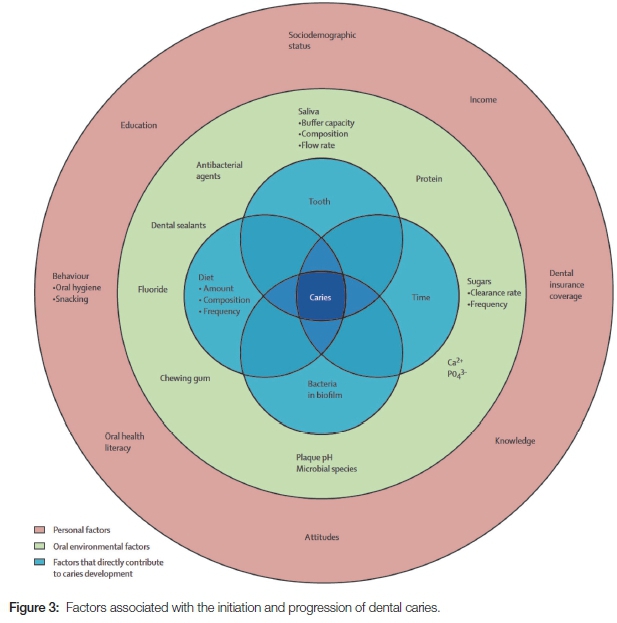
It is accepted by authorities such as the American Association of Paediatric Dentists that DC is an infectious and transmissible disease which is multifactorial and is strongly modified by diet.3-6 The aetiological factors include direct agents such as cariogenic bacteria and diet, the oral environment (saliva flow and composition) and personal factors (including oral hygiene) as reported by Selwitz et al (Figure 3).7 The personal factors also include education, socioeconomic status and immunological factors.5,6 Therefore, to control the spread of DC, there needs to be a multipronged approach targeted at both the direct and indirect etiological agents. This paper examines some of these etiological factors and provides practical solutions that could be implemented in the endeavour to control and prevent DC.
Cariogenic bacteria
The bacteria implicated in DC belong to the Streptococci mutans (SM) group, which has been shown to have a positive correlation with dental caries.3,8 There are no SM in the mouth at birth but studies show that once the teeth erupt, the prevalence of SM increases.3 The bacterium requires a non-shedding surface such as enamel to which it may adhere. With eruption of the teeth, the bacteria are provided an ideal environment in which to thrive.3
Origin of SM
Since SM are found in the mouth, transmission is likely mediated via the saliva. The primary care giver of the child (mother, father, guardian, siblings) has been implicated through genetic analysis as a donor, and studies have reported a strong positive correlation between the presence of SM in the saliva of mothers and their children.8,9 The other bacterium implicated in dental caries is Lactobacillus (LB) which is found in large proportions in cavitated lesions, suggesting that its role in dental caries is not in the initiation of the disease but rather in its progression.10
SM is part of the normal flora and as a result probably cannot be completely eliminated. However, the levels can be controlled by adequate oral hygiene and removal of plaque. Literacy and socioeconomic factors also play vital roles in the prevention and spread of DC, as these considerations affect access to oral health services and to oral hygiene necessities such as toothbrushes and fluoridated toothpaste.
Diet: Fermentable carbohydrates and time
There is overwhelming evidence that sugars and other fermentable carbohydrates, such as highly refined flour, play a role in the initiation and development of DC. Sucrose metabolism produces dextran, which promotes superior bacterial adhesion to teeth. As a result it is considered the most important substrate in the establishment of cariogenic bacteria. The frequency of sucrose intake has been shown to be more important than the total amount consumed.5,6 An increased frequency results in a decrease of the pH of the oral cavity, which enhances the establishment and dominance of SM. The duration of the sugar in the mouth directly increases the potential for enamel demineralization and reduces the time for remineralization by saliva, with the result that demineralization becomes the predominant activity.
Hence, nutritional advice is essential for the prevention of DC. However, healthy food is often more expensive and indeed inaccessible to many individuals from a low socioeconomic background. Dietary advice therefore needs to be practical and relevant for the individual and the community. The implementation of a tax on sugar sweetened beverages (SSBs) may go a long way in creating awareness of the harms of excessive sugar ingestion.11 The use of sugar free chewing gum and of xylitol as a sweetener, have also been shown to be effective in the prevention and reduction of DC.12
Susceptible tooth
A tooth is most susceptible to caries immediately after eruption. The process of enamel maturation continues following tooth eruption, the teeth becoming less susceptible to decay over time. Disturbances during embryo-logical development can result in defects on the surface enamel which could render the enamel more susceptible to DC compared with healthy enamel. These disturbances could be caused by premature birth or low-birth weight, pre- and postnatal infection/illness, nutritional deficiencies and a variety of environmental pollutants such as maternal smoking.6,13 Many of these disturbances can be prevented with adequate knowledge, access to health care and an improvement in education and literacy. As oral health practitioners, it is our duty to provide nutritional and educational advice to pregnant mothers to reduce the possibility of these defects.
Saliva flow and composition
Saliva is often referred to as "liquid gold" in the oral environment.13 It consists of a complex composition having, amongst other components, ions, enzymes and antibodies. The ions include calcium, fluoride, and magnesium, all of which are essential for tooth remineralisation. As long as the saliva is saturated with these ions, remineralization of the tooth is possible which would result in the reversal of the initiation of early DC.13 Saliva also has the ability to buffer the pH of the oral cavity, and to shift it from an acidic (demineralization) to a basic environment which promotes remineralisation. As a result, salivary flow and favourable composition are essential in the natural prevention of DC.14 Studies have also shown that children with a low saliva buffering capacity and high counts of SM and LB were more likely to develop severe DC compared with controls with lower bacterial counts and better saliva buffering capacity.10 Hence, oral health practitioners should test patients' saliva flow and composition with chair side saliva test kits which would then allow them to provide tailor made oral hygiene and diet instructions for each individual.
A reduced salivary flow could be the result of side effects of certain medications, old age, dehydration and other genetic factors. High- risk patients should have their saliva flow and composition monitored regularly and if necessary, saliva substitutes and stimulants (sugar free chewing gum) can be discussed and recommended. Clinical signs of a dry mouth include rampant caries, burning mouth, dry tongue, and halitosis.
Fluoride and fissure sealants
Fluoride, whether administered systemically or topically, has incontrovertibly been shown to reduce DC.15 The introduction of fluoridated toothpaste has indeed been shown to be the major factor in the reduction of the incidence of DC over the past ten years.14 Fluoride in drinking water, at concentrations between 0.5 and 0.7 parts per million (PPM), has been proven to reduce dental caries drastically without any side effects such as fluorosis.15 This has been the most effective public health measure in controlling DC.16
Another effective prevention strategy is the placement of fissure sealants (FSs) on permanent molars.17 These sealants protect the most vulnerable surface of the tooth (occlusal pits and fissures), and as a result have reduced the global prevalence of DC. The placement of FSs is simple and cost effective, and sealants have been proven to reduce both the initiation and progression of DC.17 Indeed, it may be argued that all children should receive FSs on their permanent molars as soon as these teeth erupt in the mouth.
Behavioural and psychosocial causal mechanisms
The importance of the interactions between biological, behavioural, cultural, social, and environmental factors in understanding health and disease is vital. Although DC can be linked to specific actions or behaviours, socio-economic status (SES) and income levels also play an important role in the prevalence of DC.18 A systematic review identified strong evidence of a consistent and significant inverse relationship between SES and the incidence of caries in children under 6 years.18 Children from poor backgrounds had more DC when compared with children who had a high SES.18
CONCLUSION
There is strong evidence that SM is transmitted from mother to infants and therefore DC is indeed a contagious disease. The affliction, however, has multiple etiological factors and if at least one or more of these factors can be controlled, then the prevalence would be reduced or the disease altogether prevented. The prevalence of DC is still relatively high, and only a multifactorial approach will be effective in its prevention and reduction. Thus, there are a host of factors that need to be addressed, and preventive programs focusing on as many of the etiological agents as possible should be initiated and this may suppress transmission of the bacteria. A few general approaches that can be used include:
a. Community based strategies that focus on educating mothers regarding their dietary habits may also influence the habits of their infants. Also included should be water fluoridation policies, and personal and community preventive programmes in high risk communities. These initiatives should incorporate oral health education to all communities using a variety of media campaigns, including mass media campaigns, as well as one-to-one counselling at a private practice level.
b. Provision of examination and preventive care in dental clinics and private practices. This includes screenings, early detection of caries, and the early identification of high risk patients such as young children, geriatrics, patients on medication, drug users, pregnant mothers, and mentally and physically handicapped individuals.
c. Encouraging private practitioners to focus on preventive rather than curative care, by increasing the financial remuneration and incentives received from Medical Aid Schemes.
d. The delivery of oral health education and instruction on improving oral hygiene and dietary practices at schools, homes, crèches and other public areas.
ACRONYM
DC: Dental caries
ECC: early childhood caries
FSs: fissure sealants
LB: Lactobacillus
SES: socio-economic status
SM: Streptococci mutans
References
1. Tinanoff N. Introduction to the Early Childhood Caries Conference: initial description and current understanding. Community Dent Oral Epidemiol. 1998;26(S1):5-7. [ Links ]
2. Milgrom P, Ly KA, Tut OK, Mancl L, Roberts MC, Briand K, et al. Xylitol pediatric topical oral syrup to prevent dental caries: a double-blind randomized clinical trial of efficacy. Arch Pediatr Adolesc Med. 2009;163(7):601-7. [ Links ]
3. Guideline on Infant Oral Health Care. The American Association of Paediatric Dentists Clinical Practice Guidelines Reference Manual 2014; 37(6):15-16. [ Links ]
4. Davies GN. Early childhood caries-a synopsis. Community Dent Oral Epidemiol. 1998;26(S1):106-16. [ Links ]
5. Gussy MG, Waters EG, Walsh O, Kilpatrick NM. Early childhood caries: current evidence for aetiology and prevention. J Paediatr Child Health. 2006;42(12):37-43. [ Links ]
6. Seow WK. Biological mechanisms of early childhood caries. Comm Dent Oral Epidemiol. 1998;26(S1):8-27. [ Links ]
7. Selwitz RH, Ismail AI, Pitts NB. Dental caries. The Lancet. 2007;12(369):51-9. [ Links ]
8. Damle SG, Yadav R, Garg S, Dhindsa A, Beniwal V, Loomba A, et al. Transmission of mutans streptococci in mother-child pairs. Indian Journal of Medical Research. 2016;144(2):264. [ Links ]
9. Niji R, Arita K, Abe Y, Lucas ME, Nishino M, Mitome M. Maternal age at birth and other risk factors in early childhood caries. Pediatr Dent. 2010;32(7):493-8. [ Links ]
10. Bhayat A, Ahmad MS, Hifnawy T, Mahrous MS, Al-Shorman H, Abu Naba'a L et al. Correlating dental caries with oral bacteria and the buffering capacity of saliva in children in Madinah, Saudi Arabia. J Int Soc Prevent Communit Dent. 2013;3:38-43. [ Links ]
11. Brownell KD, Farley T, Willett WC, Popkin BM, Chaloupka FJ, Thompson JW et al. The public health and economic benefits of taxing sugar-sweetened beverages. N Engl J Med. 2010; 362:1599-1605. [ Links ]
12. Hayes C. The effect of non-cariogenic sweeteners on the prevention of dental caries: a review of the evidence. JDE. 2001;65(10):1106-9. [ Links ]
13. Stookey GK. The effect of saliva on dental caries. JADA. 2008; 31;139:11S-7S. [ Links ]
14. García-Godoy F, Hicks MJ. Maintaining the integrity of the enamel surface: the role of dental biofilm, saliva and preventive agents in enamel demineralization and remineralization. JADA. 2008;139:25S-34S. [ Links ]
15. Marinho VC, Higgins J, Logan S, Sheiham A. Fluoride toothpastes for preventing dental caries in children and adolescents. The Cochrane Library. 2003. [ Links ]
16. Petersen PE, Lennon MA. Effective use of fluorides for the prevention of dental caries in the 21st century: the WHO approach. Community Dentistry and Oral Epidemiology. 2004;32(5):319-21. [ Links ]
17. Beauchamp J, Caufield PW, Crall JJ, Donly K, Feigal R, Gooch B et al. Evidence-based clinical recommendations for the use of pit-and-fissure sealants: a report of the American Dental Association Council on Scientific Affairs. JADA. 2008 Mar 31;139(3):257-68. [ Links ]
18. Saliba Moimaz SA, Borges HC, Saliba O, Saliba Garbin CA, Saliba NA, Moimaz SA et al. Early childhood caries: epidemiology, severity and socio-behavioural determinants. Oral Health Prev Dent. 2016;1:14(1). [ Links ]
 Correspondence:
Correspondence:
Ahmed Bhayat
P O Box 1266, Pretoria 0001, South Africa
Department of Community Dentistry, School of Dentistry
Faculty of Health Sciences, University of Pretoria, South Africa
Tel: 012 319 2299
E-mail: ahmed.bhayat@up.ac.za


{kind=link}