










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.72 n.4 Johannesburg May. 2017
RADIOLOGY CASE
Maxillo-facial radiology case 150
CJ Nortjé
BChD, PhD, ABOMR, DSc. Faculty of Dentistry, University of the Western Cape. E-mail: cnortje@uwc.ac.za
Below are a clinical picture and radiographs of two syndromes that can affect the major salivary glands. Describe the clinical and radiological features of the syndromes and what is your diagnosis?

INTERPRETATION
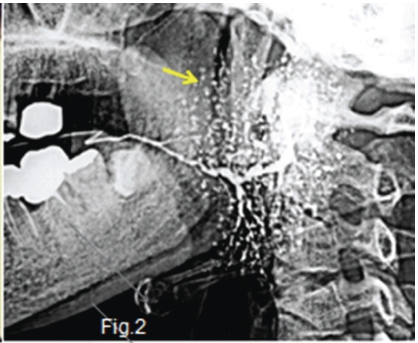
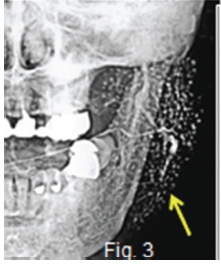
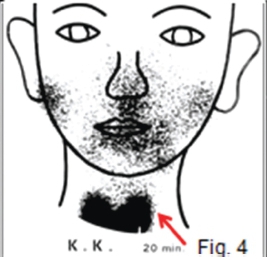
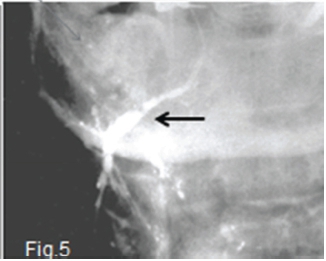
Figures 1, 2,3 & 4 refer to a syndrome reported by Sjögren in 1933, characterized by keratoconjunctivitis, dry mouth, chronic rheumatoid arthritis and swelling (green arrow) of the salivary glands. Subsequently, similar cases have been reported as Sjögren's Syndrome. The aetiology of this syndrome has remained a mystery. The syndrome occurs most commonly in middle aged women. It is a systemic disease, with the above symptoms complicated by rheumatoid arthritis, collagen disease, and autoimmune diseases, which lead to various clinical manifestations. Xerostomia is caused by hyposalivation, which may bring about arthropy, erosion, or ulcers of the oral mucosa. The cardinal sialographic findings in Sjögren's syndrome include small round shadows, called the "branchless fruit-laden tree" the appearance of which is demonstrated in Figs. 2 & 3 (yellow arrows). The degree of distension in the peripheral parts of the ducts is described as appearing in four sequential stages. Stage l is classified as the punctate pattern; Stage ll, the globular pattern; Stage lll, the cavity pattern, and Stage lV, the destructive pattern. Fig.4 is a Technetium-99 pertechnetate salivary scintigram. In contrast to strong uptake in the thyroid glands (red arrow), both submandibular and parotid glands bilaterally show minimal uptake, indicating hypofunction. In 1892, Mikulicz reported a lesion that presents as a bilateral swelling of the lacrimal glands and salivary glands. It appeared to be caused by chronic infection. Subsequently lesions with similar clinical findings have been reported, including those caused by specific inflammations, such as tuberculosis, syphilis, leukaemia and malignant lymphoma. Thus lesions resulting from any obvious cause and characterized by secondary bilateral enlargement of the major salivary glands and lacrimal glands are known are known as Mikulicz syndrome. Lesions with similar findings but of unknown origin are known as Mikulicz disease. Later, on the basis of a report by Godwin in 1962, Mikulicz disease became commonly known by the term benign lymphoeithelial lesion. The early sialographic features of this disease include irregular dilation or partial disappearance of peripheral ducts and maculation. Figure 5 is a frontal submandibular sialogram showing a distended Wharton duct (black arrow). and extensive disappearance of, or, diffuse defects of the peripheral ducts.
Reference
1. Farman AG, Nortjé CJ & Wood R E: Oral and Maxillofacial Imaging, 1st Ed, Mosby. St. Louis, Missouri 1993 pp 409-10. [ Links ]

