










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.72 n.3 Johannesburg Apr. 2017
RADIOLOGY CASE
Maxillofacial radiology case 149
CJ Nortjé
BChD, PhD, ABOMR, DSc. Faculty of Dentistry, University of the western Cape. e-mail: cnortje@uwc.ac.za
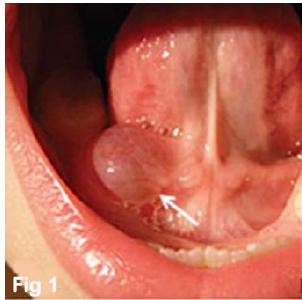
Below is a clinical picture and radiographic images of pathology which may present in the secretory portions and ducts of the salivary glands of the jaws. What are the most important findings and what is your diagnosis?

INTERPRETATION
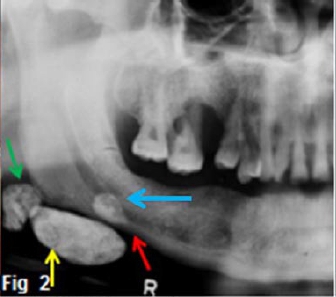
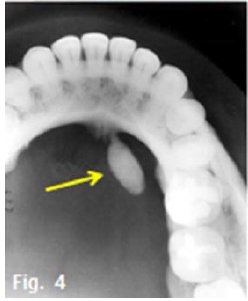
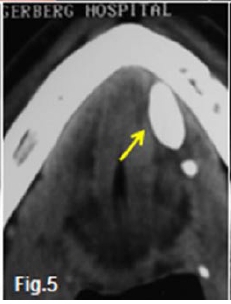
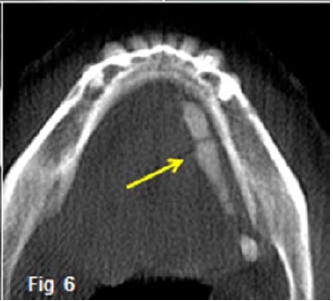
The most obvious clinical finding is the presence of a localized swelling (Fig. 1 white arrow) and multiple radiopacities at the angle of the right side of the mandible. A diagnosis of multiple calculi (sialolithiasis) within the submandibular gland (yellow arrow) and duct (blue arrow) as well as calcifications of some cervical lymph node (green arrow) was made (Fig. 2). Fig. 3 shows the salivary gland stone which was removed during surgery. An interesting observation is the erosion (red arrow, Fig 2) of the cortex of the mandible above the gigantic sialolith, which is suggestive that this stone may have been present for a long time. Ninety two percent of calculi occur in the submandibular gland, 6% in the parotid gland, and 2% in both the sublingual and minor salivary glands. Sialoliths are calcareous deposits in the ducts of major or minor salivary glands themselves. It is believed that sialoliths form by deposition of calcium salts around a central nidus that may consist of desquamated epithelial cells, foreign bodies, bacteria, abnormal mucous material, or bacterial debris. Although the cause and pathogenesis of salivary calculi are not known, several theories have been proposed. One, proposed by Rabinov and Weber (1985), is that the pathogenesis of salivary gland calculi appears to be related to the greater alkalinity of the submandibular gland as opposed to the more acidic product of the parotid gland. This difference in ph. may explain the greater incidence of stone formation in the submandibular gland. Eversole and Sabes (1971) stated that the localization of major salivary calculi primarily in the submandibular gland and the minor salivary gland calculi to the buccal mucosa suggests that local factors, such as trauma and duct morphologic characteristics, may be involved. Wharton's duct of the submandibular gland is much more irregular and longer than Stenson's duct of the parotid: Wharton's duct follows an uphill course that encourages stagnation of saliva, and stagnation leads to calculus formation. The use of an occlusal radiograph or axial CT scan is very helpful to demonstrate the very dense oval shaped mass located along the right Wharton duct. (Fig. 4 & 5 arrows)The Axial CBCT scan of the submandibular gland (Fig. 6) shows multiple strictures and dilations in Wharton's duct (string of "sausage appearance") caused by chronic infection and obstruction. After being involved by infection, the nodes become fibrous, and foci of dystrophic calcification subsequently develop.
Reference
1. Rabinov K & Weber AC: Radiology of the salivary glands. Boston:C K Hull Med publishers 1985. [ Links ]
2. Eversole L R & Sabes W R: Minor salivary duct changes due to obstruction. Arch Otolaryngology 1971;94:19 [ Links ]

