










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.72 no.3 Johannesburg Abr. 2017
CLINICAL REVIEW
Radix Entomolaris: Literature review and case report
PJ van der VyverI; M VorsterII
IBChD(Pret), Dip Odont(Aesth.Dent.) Dip Odont (Endo) MSc(Endo)(Pret). Department of Odontology, School of Dentistry, University of Pretoria, Pretoria, South Africa
IIBChD (Pret), PG Dip Dent (Endo)(Pret), Department of Odontology, School of Dentistry, University of Pretoria, Pretoria, South Africa
INTRODUCTION
According to Swartz, Skidmore and Griffen, mandibular first molars have a significantly lower success rate compared with other teeth.1 Missed canals and the failure to remove all the microorganisms and pulp remnants from the root canal system are probably the main reasons for persistent infection around endodontically- treated molars.2 It is therefore important that clinicians have an awareness and good understanding of the variations in root canal morphology of the mandibular first molar.
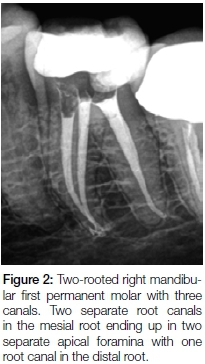
Permanent mandibular first molars in Caucasian populations are generally two rooted teeth (one mesial and one distal root) with two mesial and one distal root canals.3,4 The two mesial root canals can end up in two distinct apical foramina (Figure 1) or they can merge together at the root tip end into one apical foramen (Figure 2).5

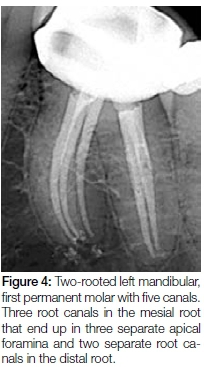
Vertucci and William (1974)6 as well as Barker et al., (1974)3 reported the presence of independent middle mesial canals in the mesial root of lower first molars (Figure 3). According to a literature review by Baugh and Wallace (2004), the prevalence of a third mid-mesial root canal in mandibular first molars is between 1-15%. They also reported that the mid-mesial canal can be independent with a separate foramen (Figure 4), or this additional canal may have a separate canal orifice and then join apically with either the mesio-buccal or mesio-lingual canal.7

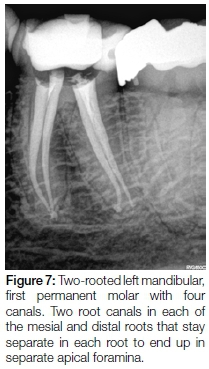
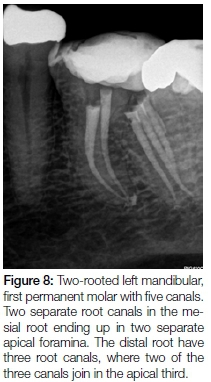
In 1971, Skidmore and Bjorndal reported that 71.1% of distal roots of mandibular first molar teeth have only one canal, 28.9% can have two canals and in rare cases it can have three root canals.8 A review article (2010) revealed that the distal root of first mandibular molars had a Vertucci Type I configuration (single pulp canal is present from the crown to the apex) in 62.7% of cases (Figure 5) followed by a Type II configuration (pulp canal separates in two near the crown and joins at the apex to form one root canal) in 14.5% of cases (Figure 6) and a Type IV configuration (pulp canal separates into two distinct canals and extends till the root apex separately) in 12.4% of cases (Figure 7).9 Another variation can also be to find three root canals in the distal roots of mandibular first molars. The incidence of three root canals in the distal root of the mandibular first molar is between 0.2% and 3% (Figure 8).10 In addition to these case reports, there have been numerous studies that clearly indicated that the mandibular first molar could present with more than four root canals.11-13


The number of roots for the mandibular first molar teeth may also vary. Carabelli (1844) was the first to report on mandibular first molars with supernumerary roots. The third root was located on the disto-lingual side and was called radix entomolaris (RE) (Figure 10).14 In very rare cases, the mandibular first molar can also present with an additional root at the mesio-buccal side and is called radix paramolaris.5,15


PREVALENCE OF RE
The presence of RE in the mandibular first molar is associated with certain ethnic groups. In populations with Mongoloid traits (for example Chinese, Eskimo and American Indians) the frequency can range from 5-30%.16-21 However, in Eurasian and Indian populations it is less than 5% and in African populations less than 3%.22
Radix entomolaris can be found on first, second and third mandibular molar teeth, occurring least frequently on second molars.23 Studies have also reported a bilateral occurrence with as frequency of 50-67%.24
ETIOLOGY OF RE
According to Calberson et al. (2007) the etiology behind the formation is still unclear but it could be related to external factors during odontogenesis.25 Racial genetic factors can also influence profound expression of a particular gene that can result in the more pronounced phenotypic manifestation.25
MORPHOLOGY OF RE
The coronal third of the disto-lingual root of RE can be fixed partially or completely to the distal root. Based on the curvature in a buccal-lingual orientation, the separate RE variants can be classified into three types according to De Moor et al. (2004).26 Type I refers to a straight root/root canal.
Type II refers to an initially curved entrance, which continues as a straight root/root canal. Type III refers to an initial curve in the coronal third of the root canal and a second curve beginning in the middle and continuing to the apical third.
RADIOGRAPHIC DIAGNOSIS OF RE
Walker and Quackenbush reported a 90% precision in the diagnosis of 3-rooted molars using only panoramic radiographs.20 However, due to the fact that the RE is found mainly in the same bucco-lingual plane of the disto-buccal root, it may cause superimposition on the preoperative periapical or panoramic image.27 This often results in inaccuracy to reveal this anatomic variation.
A major limitation of conventional radiographic images is to compress 3D anatomy into a 2D image or shadow-graph.28,29 In an attempt to overcome this drawback of conventional radiography in order to detect the presence of RE, it is helpful to take additional exposures changing the horizontal angulation of the main x-ray beam.26,30 Wang et al., demonstrated that 25-de-gree mesial radiographs were significantly better than 25-degree distal radiographs for RE visibility and determination of optimum diagnosis.31 According to Clark's rule (Also known as SLOB rule or Waltons projection), an object that moves in the same direction as the cone is located toward the lingual.32 Conversely, an object that moves in the opposite direction from the cone is located towards the buccal. Therefore, the RE image that moves distally is superimposed on the distobuccal root image that moves towards the mesial, when taking radiographs with small distal angulations.
According to Wang et al. (2011), radiographic images taken with eccentric beam angulations have the potential to improve diagnosis.31 However, they are inherently less distinct and they lose normal sharpness that is expected because anatomical structures could overlay roots and affect visibility and identification of roots and canals.33
Cone-Beam Computed Tomography (CBCT) provides dentistry with a practical tool for non-invasive and 3-dimensional (3D) reconstruction imaging for the use in endodontic applications and morphologic analyses.34 CBCT imaging allows for visualizing a new dimension, eliminate superimpositions, provide additional information for diagnosis and therefore enables a more predictable management of complex endodontic conditions compared with intraoral radiographs alone.27,35,36
CBCT imaging allows ascertaining the identification, exact location, curvature and angulation of the RE in order to prevent iatrogenic events that might occur in relation to canal curvature like instrument separation, perforation and ledge formation.37
CLINICAL DIAGNOSIS OF RE
Clinical inspection of the tooth crown and analysis of the cervical morphology of the roots by means of periodontal probing can facilitate identification of an additional root. An extra cusp (tuberculum paramolare) or more prominent occlusal distal or distolingual lobe, in combination with a cervical prominence or convexity, can indicate the presence of an additional root.5
After access cavity preparation, the location of the canal orifice of the RE can also be problematic. The orifice is generally located disto- to mesio-lingually from the main canal or canals in the distal root. The orifice is often covered with overlying dentine or pulp roof remnants and must be removed before it is possible to locate the entrance of the canal. Extension of the access cavity to the disto-lingual side also ensures easy location.
A recent study by Souza-Flamini et al., (2014) used high resolution Micro-computed tomography (uCT) to examine the internal and external morphology of RE in mandibular third molars. The spatial configuration of the canal orifices on the pulp chamber floor was mostly in a trapezoidal shape and the radix canal orifice was usually covered by a dentinal projection.27
CASE REPORT
The patient, a 45 year old female presented with pain and discomfort on her mandibular left first molar, previously restored with a ceramo-metal crown. A pre-operative radiograph revealed evidence of extensive decay on the mesial margin as well as unusual root morphology (Figure 10a). The ceramo-metal crown was removed, caries excavated and a temporary crown placed. A CBCT, axial coronal slice confirmed the presence of two roots (mesial and distal)(Figure 10b). There was no clear evidence of canal orifices in the mesial root. Two canal orifices were visible in the distal root. Another axial slice in the midroot area, revealed the presence of distal root bifurcating into two separate roots. The additional root, branching off on the lingual aspect, confirmed the presence of radix entomolaris (RE)(Figure 10c).
The canals were negotiated with size 08 C+ and K-Files to patency and a length determination was done with an electronic apex locator (Pixie, Dentsply/Maillefer) and confirmed radiographically. Reproducible glide paths were prepared with hand files and the ProGlider instrument (Dentsply/ Maillefer) and the root canals prepared with ProTaper Next X1 and X2.
GuttaCore X2 verifiers (Dentsply/ Maillefer) were fitted into the prepared root canals and a periapical radiograph revealed that the verifier in the distal root canal travelled past working length (Figure 11a). A ProTaper Next X3 guttapercha point (Dentsply/ Maillefer) was then fitted in the distal canal and a periapical radiograph confirmed a snug fit up to working length (Figure 11b). The mesio-buccal, mesio-lingual and radix entomolaris was obturated with size X2 GuttaCore obturators (Dentsply/Maillefer). The distal root canal was obturated with the ProTaper Next X3 gutta-percha point using the continuous wave of condensation technique with the Calamus Dual Obturation Unit (Dentsply/Maillefer).

Figure 12(a) depicts a parallel view of the final result after canal obturation and Figure 12(b) shows a 30 degree mesially angulated view. Note the curvature in the apical part of the radix entomolaris that was maintained during canal preparation and obturation.

DISCUSSION
Radix entomolaris, first described by Carabelli, is an anatomical variant in the first permanent mandibular molar typically characterized by an additional third root located disto-lingually.14 RE occurs in first, second and third molars with the lowest prevalence in second mandibular molars.29,38,39 Although the presence of RE differs within associated ethnical groups, it should be regarded as a normal anatomical variation within the Mongoloid population. Studies show no significant predilection for gender or side distribution with bilateral occurrence ranging between 50-67%.24 Understanding the complexity of the anatomical variants seen in the first permanent mandibular molar proves to be invaluable in the clinical approach when treating these cases endodontically.
The authors used a Global G6 (Global, USA) six-step microscope fitted with LED illumination during the clinical procedures depicted in this article. The LED light source on this microscope delivers brighter and whiter illumination compared to traditional metal halide and halogen light systems. This type of illumination makes the careful inspection of the pulp chamber floor to locate accessory canal orifices more predictable. Magnification and illumination can substantially improve the visualisation of root canal orifices. De Carvalho and Zuolo (2000) demonstrated in a study that the use of the DOM could increase the number of root canal orifices located in mandibular molars. In their study 111,93 first and second molars were examined with the naked eye followed by examination with the DOM (8-13x magnification). With the naked eye, a total of 641 canals were located. After examination with the DOM, an additional 50 canals (7.8%) were located.40
Limited field Cone Beam Computed Tomography (CBCT) with the Kodak 9000 3D (Carestream, Paris) was used as a diagnostic imaging modality for effective evaluation of the root canal morphology. Matherne et al (2008) showed that CBCT images result in the identification of a greater amount of root canal systems in teeth compared to conventional radiography.41 The study also concluded that the combination of CBCT scanning with the dental operating microscope were important diagnostic tools for locating and identifying root canals.41 In general, limited field of view (FOV) machines are preferred over larger field of view machines in Endodontics as very small structures (calcified, accessory and missed root canals) that require a high resolution for adequate interpretation are being visualized. Other advantages of the limited FOV machines include decreased radiation exposure for the patient and less responsibility for the clinician because a smaller volume needs to be interpreted.42
The Kodak 9000 3D system (Carestream) generates 3D images that provide clinicians with anatomical detail and diagnostic possibilities in the field of endodontics, implantology and oral maxillofacial surgery, periodontics, general dentistry, forensic dentistry and orthodontics. The application of CBCT technology in endodontics is not just limited to determine root canal morphology, number of roots, canals and accessory canals. It can also be used to establish the correct working length, assess existing root canal fillings, and determine the exact position and angulation of fractured instruments and to detect the presence and extent of inflammatory root resorption, just to mention a few.43
Protaper Next (Dentsply/Maillefer) was used for root canal preparation for most of the cases depicted in this article. The key benefits of Protaper Next include simplicity, excellent cutting efficiency and predictable final canal shape to allow for cone fit with tug-back. The system also ensures a 6% taper in the apical third of a canal after preparation with only two instruments, the X1 and X2.44
The Protaper Next instruments make use of the progressively tapered design. Each file presents with an increasing and decreasing percentage tapered design on a single file concept. The design ensures that there is reduced contact between the cutting flutes of the instrument and dentine wall, and reduced chance for taper lock (screw effect). At the same time, it also increases flexibility and cutting efficiency.45
Another benefit of the system is the fact that the instrument is manufactured from M-wire and not traditional nickel titanium alloy. Research by Johnson et al (2008) demonstrated that the M-wire alloy could reduce cyclic fatigue by 400% compared with similar instruments manufactured from conventional nickel titanium alloys.46 The added metallurgical benefit contributes towards more flexible instruments, increased safety and protection against instrument fracture.47
The last major advantage of root canal preparation with the Protaper Next system is the fact that the instruments present with a bilateral symmetrical, rectangular cross section (except in the last 3mm of the instrument, D0-D3). Rotation of the instrument produces a snake-like (swaggering) wave of movement. The benefits of this design characteristic include:
• It further reduces (in addition to the progressive tapered design) the engagement between the instrument and the dentine walls. This will contribute to a reduction in taper lock, screw-in effect and stress on the file.48
• Removal of debris in a coronal direction because the off-centre cross-section that allows for more space around the flutes of the instrument. This will lead to improved cutting efficiency, as the blades will stay in contact with the surrounding dentine walls. Root canal preparation is done in a very fast and effortless manner;48
• Reduces the risk of instrument fracture because there is less stress on the file and more efficient debris removal.48
• The swaggering motion of the instrument initiates activation of the irrigation solution during canal preparation improving debris removal.48
In most of the cases depicted in this article, carrier based obturation was utilized for root canal obturation. Buchanan (2009) advocates the use of carrier-based obturators in long, narrow and severely curved canals.49 The flexibility of the carrier allows for obturation of these canals, however, the stripping of the gutta-percha may cause direct contact between the plastic carrier and the dentine wall in curved canals.50 This problem has been attributed to procedural errors such as improperly shaped canals.49
GuttaCore crosslinked gutta-percha core obturators (Dentsply/Maillefer) was recently introduced to overcome these clinical challenges. GuttaCore consists of a carrier/ core manufactured from a cross-linked, thermoset elastomer of gutta-percha coated in regular gutta-percha. The core is a polyisoprene polymer cross-linked with peroxide for strength, designed to facilitate removal during retreatment and/or post space preparation by simply trephining through the core.51
CONCLUSION
The successful outcome of root canal treatment depends to a large extend on access, cleaning and shaping and three dimensional obturation of the entire root canal system. CBCT technology as well as proper angulation when acquiring radiographic images proves helpful in locating canals in especially first mandibular molars with a high incidence of anatomical variations. A thorough understanding of the prevalence of RE, its anatomical variations as well as radiographic and clinical diagnosis will provide the clinician with a better understanding of its complexity in order to ensure successful treatment outcomes.
References
1. Swartz DB, Skidmore A, Griffin J. Twenty years of endodontic success and failure. J Endod. 1983;9(5):198-202. [ Links ]
2. Himel V, McSpadden J, Goodis H, Cohen S, Hargreaves K. Pathways of the pulp, ninth edition. 2006. [ Links ]
3. Barker B, Parsons K, Mills P, Williams G. Anatomy of root canals. III. Permanent mandibular molars. Aus Dent J. 1974;19(6):408-13. [ Links ]
4. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral surg, Oral Med, Oral Pathol. 1984;58(5):589-99. [ Links ]
5. Calberson FL, De Moor RJ, Deroose CA. The radix entomolaris and paramolaris: clinical approach in endodontics. J Endod. 2007;33(1):58-63. [ Links ]
6. Vertucci F, Williams R. Root canal anatomy of the mandibular first molar. JNJ Dental Assoc. 1973;45(3):27-8 passim. [ Links ]
7. Baugh D, Wallace J. Middle mesial canal of the mandibular first molar: a case report and literature review. J Endod. 2004;30(3):185-6. [ Links ]
8. Skidmore AE, Bjorndal AM. Root canal morphology of the human mandibular first molar. Oral Surg, Oral Med, Oral Pathol. 1971;32(5):778-84. [ Links ]
9. de Pablo ÓV, Estevez R, Sánchez MP, Heilborn C, Cohenca N. Root anatomy and canal configuration of the permanent mandibular first molar: a systematic review. J Endod. 2010;36(12):1919-31. [ Links ]
10. Kottoor J, Sudha R, Velmurugan N. Middle distal canal of the mandibular first molar: a case report and literature review. Int Endod J. 2010;43(8):714-22. [ Links ]
11. Martínez-Berná A, Ruiz-Badanelli P. Maxillary first molars with six canals. J Endod. 1983;9(9):375-81. [ Links ]
12. Fabra-Campos H. Unusual root anatomy of mandibular first molars. J Endod. 1985;11(12):568-72. [ Links ]
13. Goel N, Gill K, Taneja J. Study of root canals configuration in mandibular first permanent molar. J Indian Soc Pedod Prev Dent. 1991;8(1):12-4. [ Links ]
14. Carabelli G, Carabelli G, von Lunkaszprie GC, Georg Carabelli E. Systematisches Handbuch der Zahnheilkunde: Georg Olms Verlag; 1844. [ Links ]
15. Sperber G, Moreau J. Study of the number of roots and canals in Senegalese first permanent mandibular molars. Int Endod J. 1998;31(2):117-22. [ Links ]
16. Turner CG. Three-rooted mandibular first permanent molars and the question of American Indian Origins. Am J Phys Anthropol. 1971;34(2):229-41. [ Links ]
17. Curzon M, Curzon J. Three-rooted mandibular molars in the Keewatin Eskimo. J Can Dent Assoc. 1971;37(2):71. [ Links ]
18. Yew S-c, Chan K. A retrospective study of endodontically treated mandibular first molars in a Chinese population. J Endod. 1993;19(9):471-3. [ Links ]
19. Reichart P, Metah D. Three-rooted permanent mandibular first molars in the Thai. Community Dent Oral Epidemiol. 1981;9(4):191-2. [ Links ]
20. Walker R, Quackenbush L. Three-rooted lower first permanent molars in Hong Kong Chinese. Br Dent J. 1985;159(9):298-9. [ Links ]
21. Curzon M. Three-rooted mandibular permanent molars in English Caucasians. J Dent Research. 1973;52(1):181-. [ Links ]
22. Ferraz J, Pécora JD. Three-rooted mandibular molars in patients of Mongolian, Caucasian and Negro origin. Braz Dent J. 1993;3(2):113-7. [ Links ]
23. Visser JB. Beitrag zur Kenntnis der menschlichen Zahnwurzelformen: Buchdruckerei Rotting; 1948. [ Links ]
24. Steelman R. Incidence of an accessory distal root on mandibular first permanent molars in Hispanic children. ASDC J Dent Child. 1985;53(2):122-3. [ Links ]
25. Rebeiro F, Consolaro A. Importancia clinica y antropologica de la raiz distolingual en los molars inferiors permanents. Endodoncia. 1997;15:72-8. [ Links ]
26. De Moor R, Deroose C, Calberson F. The radix entomolaris in mandibular first molars: an endodontic challenge. Int Endod J. 2004;37(11):789-99. [ Links ]
27. Souza-Flamini LE, Leoni GB, Chaves JFM, Versiani MA, Cruz-Filho AM, Pécora JD, et al. The Radix Entomolaris and Paramolaris: A Micro-Computed Tomographic Study of 3-rooted Mandibular First Molars. J Endod. 2014;40(10):1616-21. [ Links ]
28. Abella F, Mercadé M, Duran-Sindreu F, Roig M. Managing severe curvature of radix entomolaris: three-dimensional analysis with cone beam computed tomography. Int Endod J. 2011;44(9):876-85. [ Links ]
29. Tu M-G, Huang H-L, Hsue S-S, Hsu J-T, Chen S-Y, Jou M-J, et al. Detection of permanent three-rooted mandibular first molars by cone-beam computed tomography imaging in Taiwanese individuals. J Endod. 2009;35(4):503-7. [ Links ]
30. Yang Y, Zhang L-D, Ge J-p, Zhu Y-q. Prevalence of 3-rooted first permanent molars among a Shanghai Chinese population. Oral Surg, Oral Med, Oral Pathol, Oral Radiol, and Endod. 2010;110(5):e98-e101. [ Links ]
31. Wang Q, Yu G, Zhou X-d, Peters OA, Zheng Q-h, Huang D-m. Evaluation of X-ray projection angulation for successful radix entomolaris diagnosis in mandibular first molars in vitro. J Endod. 2011;37(8):1063-8. [ Links ]
32. Ingle J, Heithersay G, Hartwell G, Goerig A, Marshall F, Krasny R, et al. Endodontic diagnostic procedures. Endodontics, 5th edn Hamilton, London, UK: BC Decker Inc. 2002:203-58. [ Links ]
33. Fishel D, Buchner A, Hershkowith A, Kaffe I. Roentgenologic study of the mental foramen. Oral Surg, Oral Me, Oral Pathol. 1976;41(5):682-6. [ Links ]
34. Prashanth M, Khandelwal A. Endodontic management of three rooted, four canalled mandibular first molar (radix entomolaris): a case report. JPFA (India Section). 2012;26(2):86-8. [ Links ]
35. Patel S, Dawood A, Ford TP, Whaites E. The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J. 2007;40(10):818-30. [ Links ]
36. Tu M-G, Tsai C-C, Jou M-J, Chen W-L, Chang Y-F, Chen S-Y, et al. Prevalence of three-rooted mandibular first molars among Taiwanese individuals. J Endod. 2007;33(10):1163-6. [ Links ]
37. Mahendra M, Verma A, Tyagi S, Singh S, Malviya K, Chaddha R. Management of complex root canal curvature of bilateral radix entomolaris: three-dimensional analysis with cone beam computed tomography. Case Reports In Dentistry. 2013;2013. [ Links ]
38. Segura-Egea JJ, Jiménez-Pinzón A, Ríos-Santos JV. Endodontic therapy in a 3-rooted mandibular first molar: importance of a thorough radiographic examination. J Can Dent Assoc. 2002;68(9):541-5. [ Links ]
39. Garg AK, Tewari RK, Kumar A, Hashmi SH, Agrawal N, Mishra SK. Prevalence of three-rooted mandibular permanent first molars among the Indian population. J Endod. 2010;36(8):1302-6. [ Links ]
40. de Carvalho MCC, Zuolo ML. Orifice locating with a microscope. J Endod. 2000;26(9):532-4. [ Links ]
41. Matherne RP, Angelopoulos C, Kulild JC, Tira D. Use of cone- beam computed tomography to identify root canal systems in vitro. J Endod. 2008;34(1):87-9. [ Links ]
42. AAE A. Use of cone-beam computed tomography in endodontics Joint Position Statement of the American Association of Endodontists and the American Academy of Oral and Maxillofacial Radiology. Oral Surg, Oral Med, Oral Pathol, Oral Radiol Endod. 2011;111:234-7. [ Links ]
43. Alshehri ADMA, Alamri HM, Alshalhoob MA. CBCT applications in dental practice: A literature review. Oral and maxillofacial surgery. 2010;36:26.86. [ Links ]
44. Van der Vyver P.J. Management of an upper first molar with three mesiobuccal root canals. Endod Prac. 2013:21-25. [ Links ]
45. Ruddle CJ. The ProTaper endodontic system: geometries, features, and -guidelines for use. Dent Today. 2001;20(10):60-7. [ Links ]
46. Johnson E, Lloyd A, Kuttler S, Namerow K. Comparison between a novel nickel-titanium alloy and 508 nitinol on the cyclic fatigue life of ProFile 25/. 04 rotary instruments. J Endod. 2008;34(11):1406-9. [ Links ]
47. Gutmann J, Gao Y. Alteration in the inherent metallic and surface properties of nickel-titanium root canal instruments to enhance performance, durability and safety: a focused review. Int Endod J. 2012;45(2):113-28. [ Links ]
48. Van der Vyver P, Scianamblo M. Clinical guidelines for the use of ProTaper Next instruments: part two. Endod Prac. 2014;7(2):12-8. [ Links ]
49. Buchanan S. Common misconceptions about carrier-based obturation. Endod Prac. 2009;12(4):30-4. [ Links ]
50. Leung S, Gulabivala K. An In vitro evaluation of the influence of canal curvature on the sealing ability of Thermafil. Int Endod J. 1994;27(4):190-6. [ Links ]
51. Alhashimi RA, Mannocci F, Foxton RM, Deb S. Synthesis and preliminary evaluation of a polyolefin-based core for carrier- based root canal obturation. J Endod. 2012;38(7):983-6. [ Links ]
 Correspondence:
Correspondence:
Peet J van der Vyver
PO Box 2609, Cresta, 2118
Tel: +27 11 781 1020. Cell: 082 4104 293
E-mail: peetv@iafrica.com

