










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.72 n.2 Johannesburg Mar. 2017
CASE REPORT
A compromise between orthodontics and surgery: a case report
TC Dandajena
DDS, MS, PhD. Professor and Head, Department of Orthodontics and Paediatric Dentistry, School of Oral Health Sciences, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg. E-mail: tarisai.dandajena@gmail.com
INTRODUCTION
Careful planning goes into the management of the patient who is to receive surgery to complement the orthodontic treatment, which may in fact be prolonged. Quite often, extraction of teeth is required, and the extraction spaces will, most of the time, need to be closed before the patient undergoes surgery. Space closure may demand some 18 months and even longer if there is sequential retraction of the canines followed by the incisors as in Group A anchor-age.1 The same is true in Group C anchorage where the treatment requires protraction of the posterior segments.1
Space closure prior to orthognathic surgery is the ideal situation. However, there could be a compelling reason that the surgical procedure be expedited and the surgery then performed prior to the completion of space closure. In the USA, for example, the insurance of adolescent patients was sponsored under the parent's plan, and usually termed out at 18 years. Hence the family, for insurance reasons, will want to have the surgery completed by the time their child reaches 18 years of age. In such circumstances, the surgeon and orthodontist have to work together closely to achieve a desirable result. The orthodontist in particular may have to compromise from the ideal to help the patient have the surgery before the extraction spaces are fully closed.
Paradoxically, orthodontic space closure after the operation may progress faster than prior to surgery. This has been demonstrated with corticotomies performed to expedite the orthodontic treatment.2,3 This approach of surgery first is indicated for the regular orthodontics-orthognathic surgery patient but may not be desirable in the case of severe craniofacial anomalies as in cleft palate. In the event that such an approach of early surgery is elected, it is imperative that the orthodontist be involved in the surgical setup and it is crucial that the patient be seen by the orthodontist as soon as possible after the surgery so that space closure may proceed immediately and the proper use of elastics be instituted.
The purpose of this clinical report is to show that with proper communication between the orthodontist and the surgeon, it may not be necessary to mandate space closure prior to surgery - even in patients with severe craniofacial anomalies. The report highlights a patient who underwent surgery prior to completion of space closure, the residual spaces being subsequently closed a short while later.
PATIENT HISTORY
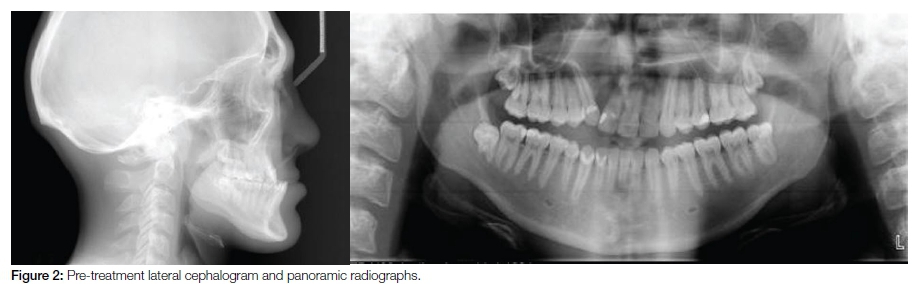
The patient was a Caucasian male with chronological age of 17 years nine months (CA = 17-9) and Class III (Cl III) occlusion (Figures 1, 2). He had a repaired Veau Class III4 hard tissue cleft to the right. Clinical and radiographic examination revealed the presence of 31 permanent teeth. The maxillary right lateral incisor was missing (UR2), which is not unusual for a patient with a cleft. There were generalized carious lesions and demineralization with the maxillary left second molar being the most affected. The patient had completed a phase of orthodontic treatment elsewhere at an earlier age as well as surgical augmentation of the nose. While the cleft had been repaired, the closure was of the soft tissue only with the bone still severely deficient in the area of the cleft. The previous orthodontist had closed the space of the missing upper right lateral incisor, resulting in the maxillary midline being displaced to the right.
Cephalometric evaluation indicated that the patient also had a prognathic mandible for which mandibular surgery was needed to harmonize the patient's occlusion and aesthetics. However, the patient's medical insurance would not authorize double jaw surgery. Notably, he was approaching 18 years and the surgery needed to be done promptly. Hence, the patient presented with the following as the major problems with the possible solutions listed:
1. The maxillary arch was one tooth smaller than the mandibular arch due to the missing UR2. It would not be possible to re-open space for the missing lateral incisor since there was no bone in the area. Even with a bone graft, we risked damage to the maxillary right central incisor (UR1).
2. A tooth had to be extracted in the maxillary anterior segment so as to match the missing UR2. If this were not done, the midlines would never coincide since the mandibular anterior segment held one incisor more than the maxillary. Hence, we opted to extract the maxillary left lateral incisor (UL2).
3. However, we could not first extract, consolidate space and only then send the patient for surgery since at the time, the State Child Health Insurance Programme (SCHIP) a form of medical aid designed specifically for children, terminated when the child reached 18 years of age. The surgery had to be done expeditiously and grafting of bone also had to be effected at the time of surgery.
4. The mandible was prognathic thus complicating the case which ideally required double jaw surgery. The patient was, however, denied that option hence we were limited to maxillary surgery only.
FINAL TREATMENT PLAN
We planned to extract the UL2 at the time of surgery with eventual substitution of the maxillary lateral incisors by the canines. This meant that the midlines could not be used for the surgical setup. The premolars and canines had to be used as the surgical guides, with the maxillary first premolars as canines and in Class I canine relation (Figure 3). This information had to be clearly communicated to the surgeon. The bone defect on the right would be grafted during surgery as well. With the participation of the orthodontist, the pre-surgical setup was designed so that the maxillary and mandibular midlines were not coincident, and the maxillary midline was off to the right with more overjet on the left. Orthodontic treatment proceeded after the required restorations were completed and fluoride treatment was delivered.
POST TREATMENT REVIEW
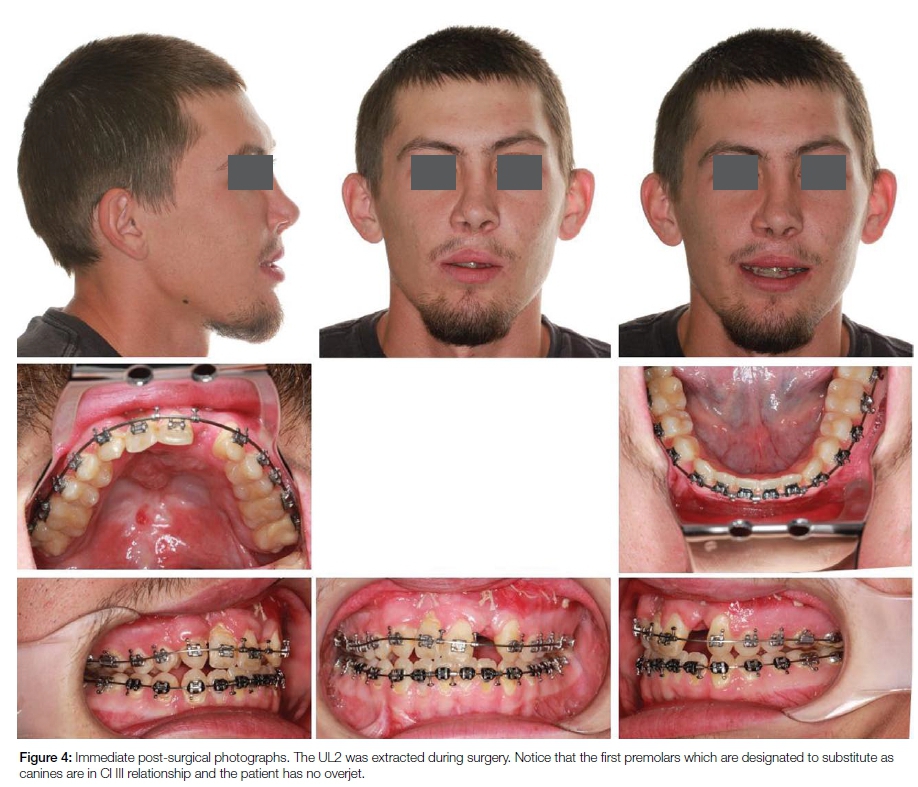
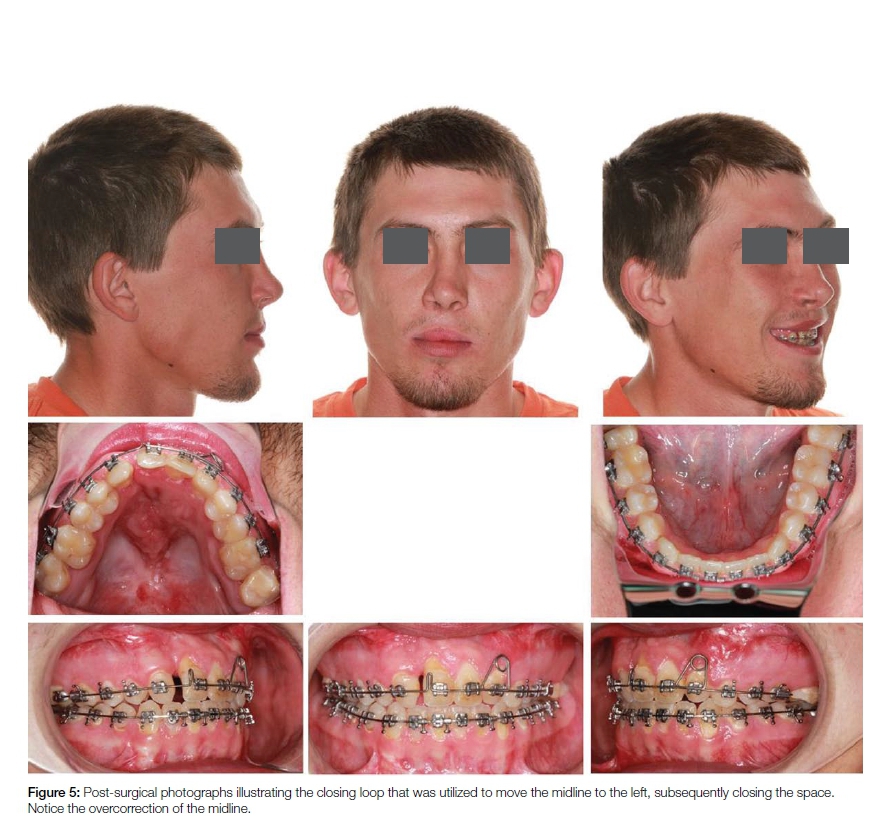
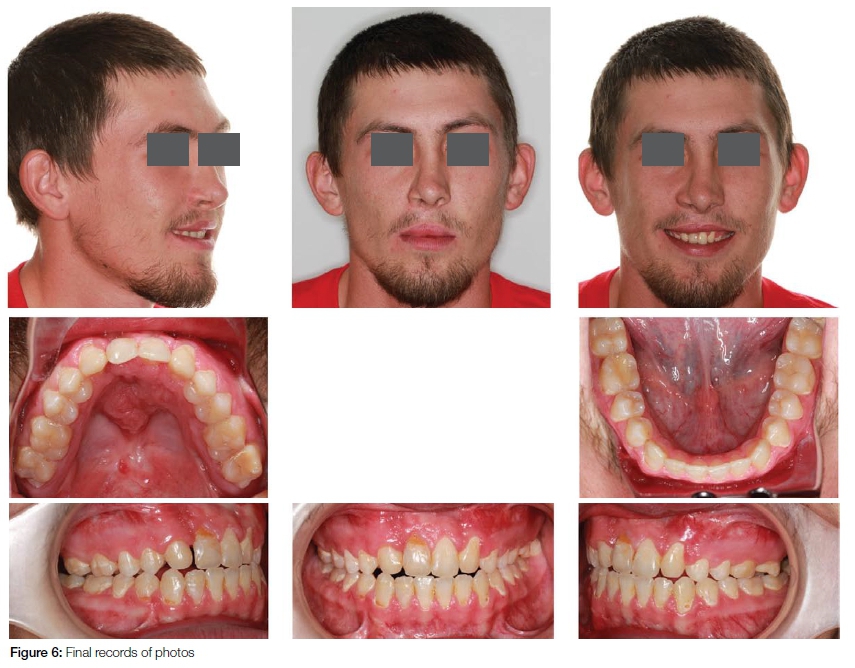
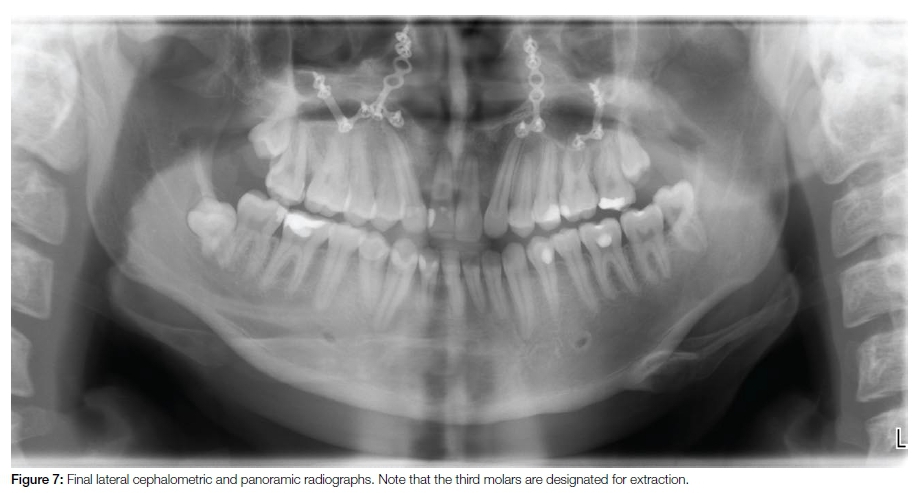
Two weeks post-surgery, the patient presented to the orthodontist with no overjet and the maxillary first premolars (now serving as the canines) in a Cl III relationship (Figure 4). We resolved to use a reverse pull headgear (RPHG) to protract the maxilla while closing the space from which the UL2 had been extracted. A midline correction loop was used to unilaterally close the space and move the maxillary midline towards the left (Figure 5). The RPGH was worn at night and Cl III elastics were used 24/7. The Cl III elastics (Moose, 6 oz, 5/16 inches, Ormco Corp, Glendora, Ca, USA) were prescribed to deliver both 1st and 2nd order vectors of force. The patient was seen every three weeks and the space was closed in three months with successful correction of the midline (Figures 6 and 7). However the occlusion was not refined as there was some relapse resulting in a less than perfect interdigitation of the teeth.
DISCUSSION
Both orthodontist and surgeon would prefer to conduct the surgical procedure when the respective dental arches are relatively well aligned and coordinated. This is especially true where extractions are involved and the situation demands prior closure of the extraction spaces. However this is not always possible for a variety of reasons, a major consideration being insurance limitations and in particular state/federally funded insurance programmes as in SCHIP.
Such programmes are an important resource. However, the cutoff age of 18 years presents some problems to patients with craniofacial anomalies since treatment is likely to extend beyond that age. Hence, the orthodontist and surgeon have to be prudent in their management of these patients to ensure the most appropriate care possible is delivered in a timely manner.
The patient presented in this paper demonstrated the importance of good communication and coordination between the orthodontist and the surgeon. Once the surgery is completed, it becomes the responsibility of the orthodontist to properly coordinate the arches. This can be a difficult challenge if the post-surgical outcome is not ideal... as indeed was the situation in this patient. While there was adequate communication between the orthodontist and the surgeon, some unpredictable things could still happen.. which in this patient was immediate post-surgical relapse.
The surgical planning should accommodate for relapse by over-correcting. This security was probably not properly provided for and the patient presented with a Cl III relationship at the orthodontic post-op appointment, which was only two weeks after surgery. In as far as this patient was concerned, better postoperative results could have been achieved had the surgical plates been removed to facilitate protraction of the maxillae. However, this was not possible since bone had been grafted over the plates. This type of grafting had to be done since the patient did not have adequate bone on the facial/buccal surfaces of the maxilla.
It is imperative that the patient visit the orthodontist as soon as immediately possible post-surgery, for a variety of reasons, one being the need for post-op control since it is the orthodontist who has the planned vision of how the teeth should interdigitate when all the procedures have been completed. A second reason in this case was that since the surgery was conducted prematurely the spaces should be closed as soon as possible post op. Teeth move by inflammation and all the relevant factors required for bone remodeling would have been activated by the surgery. Taking advantage of the surgical procedure is equivalent to performing corticotomies for enhanced tooth movement.5
The rate limiting step of tooth movement is bone resorp-tion.6 Resorption depends upon the type and quality of bone as well as osteoclast (OC) recruitment to the remodeling site. OC are members of the reticuloendothelial system. These osteoclasts do not necessarily originate from the bone marrow but develop from circulating monocytes.7 Delivery of the osteoclasts to the remodeling site is also dependent upon the vasculature. The system becomes highly active when there is inflammation. The surgical procedure provides an opportunity for faster bone remodeling since all appropriate angiogenic factors come into play after surgery. Hence, it is prudent that the patient see the orthodontist as soon as immediately possible to initiate space closure. Efficient systems need to be designed to close the spaces as shown in the case presented here.
Based on the determinants of tooth movement which include type of bone, its quality and osteoclast recruitment, it may not be necessary to complete the space closure prior to surgery. Indeed, these movements should be easier and more convenient after the surgery. However, a proper plan needs to be in place well ahead of time to ensure efficient management of the patient immediately post-surgery. The role of the orthodontist becomes critical in the pre-surgical setup.
SUMMARY AND CONCLUSION
It is not necessary to always complete space closure prior to surgery. Teeth move faster immediately post-surgery. Tooth movement is an inflammatory process and this is enhanced by the surgery.
In such cases, it is critical that the orthodontist view the surgical setup considering that the greater proportion of the space closure will be accomplished post surgery. The orthodontist will need to see the patient as soon as it is physically possible after surgery to complete the necessary, orthodontic movements. The intervals between appointments will need to be shortened since the space closure is more of a distraction than regular tooth movement. The treatment of a patient was presented which demonstrated the importance of good communication between the orthodontist and the surgeon. The presentation demonstrated that extraction space closure can be accomplished much faster post-surgery.
References
1. Nanda R, Kuhlberg A, Uribe F. Biomechanical basis of space closure. In: Nanda R, editor. Biomechanics and Esthetic Strategies in Clinical Orthodontics. Saint Louis, MO: Elsevier-Saun-ders; 2005. Pp. 194-210. [ Links ]
2. Amit G, Kalra JPS, Pankaj B, Suchinder S, Parul B. Periodontally accelerated osteogenic orthodontics (PAOO) - a review. J Clin Exp Dent 2012;4:e292-6. doi: 10.4317/jced.50822. [ Links ]
3. Bell WH, Finn RA, Buschang PH. Accelerated orthognathic surgery and increased orthodontic efficiency: a paradigm shift. J Oral Maxillofac Surg. 2009;67:2043-4. [ Links ]
4. Veau V. Treatment of the unilateral hairlip. International Dental Congress Eighth Transaction 1931:126-31. [ Links ]
5. Murphy KG, Wilcko MT, Wilcko WM, Ferguson DJ. Periodontal accelerated osteogenic orthodontics: a description of the surgical technique. J Oral Maxillofac Surg. 2009;67:2160-6. [ Links ]
6. Roberts WE. Bone physiology, metabolism and biomechanics in orthodontic practice. In Graber TM, Vanarsdall RL, Vig KWL, editors. Orthodontics: Current Principles and Techniques. Saint Louis, MO: Elsevier-Mosby; 2005. pp221-292. [ Links ]
7. Dandajena TC, Ihnat MA, Disch B, Thorpe J, Currier GF. Hypoxia triggers a HIF-mediated differentiation of peripheral blood mononuclear cells into osteoclasts. Orthod Craniofac Res 2012;15:1-9. [ Links ]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}