










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.72 n.2 Johannesburg Mar. 2017
RESEARCH
Biaxial flexural strength of three ceramic oxide core materials
H DullabhI; D HerbstII; L SykesIII; N BiseswarIV
IBChD, MSc, MDent. Professor and Head of Department of Prosthodontics, School of Oral Health Sciences, University of Pretoria
IIBSc, BChD, MChD, FCD(SA) Prost. Senior Specialist, Department of Prosthodontics, School of Oral Health Sciences, University of Pretoria
IIIBSc, BDS, M.Dent. Principal Specialist and Associate Professor, Department of Prosthodontics, School of Oral Health Sciences, University of Pretoria
IVBDS, MChD. Specialist, Department of Prosthodontics, School of Oral Health Sciences, University of Pretoria
ABSTRACT
INTRODUCTION: Brittleness and low strength render conventional ceramic systems unsuitable for routine restorative use in molars. Modern, high-strength ceramic core materials such as high purity aluminum oxide (Al2O3) and yttrium - partially stabilized zirconia (Y-PSZ) have been designed for aesthetic, metal-free, all-ceramics in posterior teeth.
AIMS AND OBJECTIVES: 1. To compare the biaxial flexural strengths of these two core materials.
2. To compare the strengths of Y-PSZ samples produced by two manufacturers.
MATERIALS AND METHODS: Three groups of discs measuring 16mm diameter and 2mm thickness were prepared for each of the sample materials, high purity Al2O3, commercially available as Turkom-Cera, and Y-PSZ, commercially available as Cercon and LAVA. The Biaxial flexural strengths were measured using a Zwick Z010 Material Testing Machine. Reliability was compared using Weibull Moduli.
RESULTS: Mean strengths for LAVA, Cercon and Turkom-Cera were 866.44, 586.92, 155.71 MPa respectively. Statistically significant differences were shown between the mean values.
DISCUSSION AND CONCLUSIONS: This project showed that the samples of Y-PSZ had higher biaxial flexural strengths than those of high purity Al2O3. The biaxial flexural strengths of Y-PSZ, sourced from two manufacturers, are significantly different. It is suggested that Y-PSZ is suitable and indicated for restorative use in molar regions.
Keywords: High-strength ceramics; tensile stress.
INTRODUCTION
The continued development of ceramic restorative materials has resulted in a wide choice of products being available for the dentist. When selecting the most appropriate for each clinical situation, a number of factors need to be considered. Of these, material strength is often cited as the most pivotal for long-term success of the restoration.1 In many of the older porcelains, despite the glazed surfaces providing resistance to mechanical abrasion and accumulation of bacterial plaque,1 the bulk material was brittle, with a low tensile strength, rendering the restoration prone to stress-induced fractures over time.1-3
A number of new core ceramic materials offering higher tensile, compressive and flexural strengths as well as improved aesthetics have been developed in the endeavour to overcome this problem, as well as to address the increased public demand for metal free restorations.4,5 Two such products of interest are Y-PSZ, (commercially available as Cercon from Dentsply, and LAVA from 3M ESPE) and high purity Al2O3 (marketed as Turkom-Cera from Turkom-Ceramic, comprising 99.98% Al2O3).6,7 The Cercon and Lava systems are often referred to as "all-ceramic", with both having Y-PSZ as their core materials, and fabrication of the prosthesis is generally completed with computer-assisted design (CAD) and computer-assisted manufacturing (CAM) technology. However, each is characterized by their own unique software, recommendations and handling properties.
Research on the fracture resistance of high purity Al2O3 reports good five-year survival rates when the material is used for single crown restorations in the posterior re-gion.8,9 In these studies, however, survival and success were measured on samples which relied on different inclusion and exclusion criteria. While the use of both Y-PSZ and Al2O3 as core materials is widely advocated,5,8-10 there is still scepticism about their strength when used in all-ceramic systems.
LITERATURE REVIEW
The word "ceramic" evolved from the Greek word keramos, which indicates a material that is fabricated by burning or firing.1 Early dental ceramics consisted of a blend of kaolin and other minerals such as silica and feldspar, which imparted both strength and translucency.1 The first metal-free jacket crown was fabricated in the late 1800s by moulding platinum foil over an abutment, and then layering this with porcelain. This mould was then repeatedly fired until the desired characteristics were obtained.11 Many years later (1965), high alumina jacket crowns were developed in the attempt to overcome the low fracture resistance of the metal- free jacket crowns. These were produced by spreading alumina particles into a glassy matrix, and moulding this over the platinum foil.12 The resulting reinforced porcelain core contained about 40 to 50% alumina which reportedly increased the strength of the final crown by about 50%.1213 In the late 1900s, the use of platinum-bonded alumina was extended to include fixed partial dentures. It was hoped that its increased strength would address the problem of fracture through the connector area while doing away with the original cast metal substructure.14 Unfortunately this material still suffered high fracture rates. Since then, there has been a vast expansion of growth and research into dental ceramics. At present these can be divided into three distinct groups: Silica-based, Aluminum oxide-based and Zirconium oxide-based.15
a. Silica based ceramics
Conventional silica based ceramics, or feldspathic porcelains, were the first types of porcelains used for dental crowns.15 These ceramics offered adequate translucency, but their major disadvantage was low flexural strength and compromised longevity.15 The development of platinum bonded alumina cores seemed to be a promising breakthrough in terms of strength, allowing them to be used for fixed partial dentures. However, inadequate wetting of the platinum foil resulted in poor bonding between the substructures and the overlying porcelain, which became a major clinical problem.12,13
This led Innotek to develop the Cerestore system which made use of an epoxy die and an injection moulded aluminous porcelain core.13 The process involved the use of a wax pattern flasked onto an epoxy die, then the wax was boiled out, the ceramic material was heated, injected into the space and immediately fired.1316 By controlling the firing process and by converting alumina and magnesium oxide to a magnesium oxide crystal, a totally shrink-free crown was produced.13,16 The high alumina concentration appreciably improved strength, which allowed these crowns to be used in posterior regions, however, despite improved light transmission, aesthetics were compromised due to the high content of alumina particles.13 Further disadvantages were the costly equipment and the restorations were found to be no stronger than conventional sintered alumina restorations.1
Dicor (Dentsply International) revolutionised a castable glass method by using a conventional wax pattern that was invested, burnt out and then cast with a glass consisting mainly of: SiO2, K2O, MgO and MgF2.15,16 The advantages of this system were the minimal tooth preparation required along with improved aesthetics.
The Renaissance system (Williams Gold Refining Company) then developed a material based on the premise that if the platinum foil were left on the inside of the core, the strength could be improved.2 However, the new material replaced the platinum with a gold foil in an attempt to enhance the natural tooth colour and improve aesthetics. Not only was this system technically challenging, but once again the lack of a core made these restorations weak.
The IPS-Empress system (Ivoclar), is a metal-free ceramic consisting of silicone dioxide, lower amounts of aluminium dioxide, and reinforced with leucite. It was developed as a cast-free ceramic with the intent to exclude the micro-porosities seen in materials that had undergone a firing process.13,17 The first system, Empress 1, accommodated preparations using a conventional wax mould as well as those created digitally using a CAD/CAM processes. The main problem was that the product had low fracture resistance and could only be used for single restorations.13,15 Later, Empress 2 was developed using an identical manufacturing progress, but with the inclusion of a lithium dis-ilicate glass core which improved its flexural strength to 300-400 MPa18. Unfortunately it has a discouragingly challenging technique- sensitive laboratory process.15
b. Aluminum oxide (Al2O3) based ceramics
These all have Al2O3 cores interspersed with infiltrates in varying proportions depending on the manufacturers and the systems. In-Ceram Spinell (Vita Zahnfabrik, Bad Säckingen) is infiltrated with magnesium, and is suited to the anterior regions of the mouth due to its enhanced translu-cency,19 but the material has inadequate flexural strength for use in the posterior regions. In-Ceram Alumina (Vita), was the first ceramic system that could be used for three unit fixed partial dentures due to the increased flexu-ral strength gifted by the partially sintered alumina (352 to 600 MPa).7,20 Despite the alumina being denser than leucite glass, the final product still has excellent aesthetics. In-Ceram also offers two fabrication methods. In the dry press method, pre-sintered blanks are milled with or without CAD/CAM software.15 In the slip method, alumina particles are spread into an aqueous solution, which is then plastered onto the die.15,21,22 The long-term survival rates of the In-Ceram Alumina restorations are contentious, with reported higher failure rates in premolar and molar restorations than in the anterior region.23
The Procera AllCeram System (Nobel Biocare) aims to maximize on the strength of alumina, and uses a pure, densely sintered aluminum oxide core (99.9% Al2O3).24 The flexural strength is between 480-700 MPa, allowing it to be used in both anterior and posterior restorations.15,25,26 Although some studies have reported higher failure rates in posterior restorations,24,27 there are sufficient short-term clinical studies demonstrating success,8,9 as well as reports showing good accuracy when used for crown sub-structures.28,29
TurkomCera (Turkom Ceramics) is another high purity Al2O3 (99.98%),7 but in contrast to those mentioned above, the system employs conventional methods of crown fabrication. This eliminates the need for costly CAD/CAM systems, making it an appealing option.7
c. Zirconium oxide based ceramics
Zirconium oxide based ceramics consist of predominantly zirconium-oxide polycrystalline cores, which are prepared at much higher sintering temperatures than used in other ceramic systems. One of the early zirconium based ceramics was In-Ceram Zirconia (Vita). It consists of a 35% partially stabilized zirconia reinforced aluminium base which greatly enhanced flexural strength (600 and 800 MPa), and provided a fracture toughness that was much higher than that achieved in the Empress 2 system.30,31 It was thus advocated for use in both anterior and posterior regions as well as for fixed partial dentures.4,30 However, there are contraindications, the main problem being that the zirconia reinforcement prevents adequate light transmission.15 Attempts to overcome this by reducing the thickness of the concentrated aluminium core resulted in a decrease in the flexural strength of the final prosthesis.30 Therefore, if this system is to be used, more tooth reduction is necessary to maintain the required thickness.
Structurally, zirconium oxide is a multiphase material having three forms, depending on the temperature to which it is exposed. Pure zirconia, at 23700C, has a cubic structure.6 When it starts to cool to between 21000C and 11700C, it presents with a tetragonal structure.6 Below 11700C, the tetragonal phase shifts into a monoclinic phase during which it undergoes a volume expansion of about 3%.6 This volume expansion can enhance crack propagation through the material which is undesirable. Stabilizing agents can be added to the zirconia to control this volumetric expansion.1,33 For example, addition of yttrium oxide stabilizes the transforming zirconia system in the tetragonal phase and retains the layer of compressive stresses. The subsequent formation of a yttrium-stabilized tetragonal zirconia polycrystalline (Y-PSZ) ceramic permits the characteristic high fracture strength.4,31-33 This is the concept of transformation toughening, which is the basis for longevity associated with Y-PSZ ceramic systems.4,31-3
Recently the use of yttrium tetragonal zirconia polycrystals (Y-PSZ) as high strength core materials has received increased focus.4,31,32 Many ceramic systems like LAVA and Cercon embrace the use of this Y-PSZ. These high strength ceramic systems depend mainly on the reliability of CAD/ CAM technology. The Cercon system involves conventional waxing up procedures for designing the substructure.34 The zirconia cores are milled by the Cercon-smart ceramics system using Cercon blanks made of yttrium-partially stabilized zirconium (Y-PSZ).34 The first step is the laser scanning process of the hand carved wax pattern of the substructure. Then the enlarged shape of the core is milled out of prefabricated blanks and then sintered to full density. During firing, the framework shrinks to the desired definitive dimensions. The milling process is faster and the abrasion of hardware is less than the milling from a fully sintered blank.34
The LAVA system also employs Y-PSZ core materials, but unlike the Cercon system, it is fully CAD/CAM dependant. The LAVA copings are manufactured using partially sintered zirconium oxide blanks, because fully sintered blanks are too hard to be machined efficiently.31These partially sintered milled copings, (greatly oversized to compensate for shrinkage), are then fully sintered and fitted onto the abutment die.31
Although positive clinical outcomes have been reported using Y-PSZ systems, the majority of studies are short term, and reports that compare different manufacturers are scarce.31,34,35 Biaxial flexural strength of between 900 and 1200 MP for Y-PSZ have been cited. 6,32,33
Computer aided design/Computer aided manufacturing (CAD/CAM)
The first CAD/CAM use in dentistry was in 1985, when Sirona launched Cerec 1 to produce direct computer-aided ceramic inlays.36 After further development of the milling unit and refining the resolution of the cameras, Cerec 2 emerged which helped improve the marginal accuracy and to increase the scope of use of the system.36 There are numerous long-term reports showing the success of veneers prepared with CAD/CAM technology, and stating that the quality of fit was comparable with that produced by hand in laboratories.37,38
There are now many modern CAD/CAM systems for producing ceramic restorations, all of which claim to minimize flaws otherwise associated with the conventional fabrication method. Thus the quality of the final finished product is en-hanced.33,36 The process involves scanning a die and then sending the data to a laboratory where alumina or zirconia cores are fabricated, after which the final porcelain is processed onto the restoration. Each type of modern ceramic is linked to a specific CAD/CAM system which includes scanning, a unique manufacturing plant and specific software. The operator uses precision software to program the design of the coping, and to then instruct the milling machine on the correct manufacturing routine for the final restoration. LAVA and Cercon are among these modern systems.
Laboratory CAD/CAM systems recreate occlusal anatomy and functional contacts using accurately replicated abutment dies, in the attempt to minimize the amount of intraoral occlusal adjustments.37 The main advantage of CAD/ CAM technology is that it allows predictable machining of high-strength core materials like Y-PSZ, that would otherwise be almost impossible, because grinding by hand, without accurate cooling, would create surface cracks and flaws and thus reduce final strength values. In addition, CAD/CAM technology reduces the number of appointments and chairside stages (impressions), eliminates many of the problems that arise from indirect fabrication, and allows for the use of stronger and more resistant ceramic materials.33,34 For example, without a computer it would be tedious and probably inaccurate to try to estimate the shrinkage of zirconium oxide. Thus specific software has been created to calculate this shrinkage, and the extent of enlargement of the die, which is required in compensation. With so many systems being marketed, more scientific reports are needed on the performance and long-term successes of the restorations which are produced with each system.
Most dental ceramics are able to withstand compres-sive better than tensile stresses. The latter are more pronounced during function and parafunction, and should be the focus of analysis when testing the performance of ce-ramics.39 Although uniaxial strength tests were common in the past, it is recognised that biaxial flexural tests are more reliable.40 This is because with most ceramic restorations there is already a state of biaxial stress present thus test results from uniaxial tests cannot be totally ac-curate.41 In addition, unwanted edge fractures can occur during uniaxial testing, which would influence the precision of measurement of the final strength value.39-41 In biaxial flexural strength tests, the edges are not under load and the accuracy of the results is improved.5,39 This study has therefore relied on biaxial flexural strength tests and calculation of the Weibull moduli.5,39
AIM
The aim of this in-vitro study was to compare the biaxial flexural strengths of three different ceramic core materials.
These consisted of two Y-PSZ products (Cercon and LAVA), and one Al2O3 product (Turkom-Cera). Additionally, there was an objective to assess whether there were any differences in the strengths of the samples of Y-PSZ produced by the two manufacturers.
MATERIALS AND METHODS
The test material consisted of three different all-ceramic high-strength systems, namely: LAVA (3M ESPE, Dental Products, Saint Paul, Minnesota, United States of America), a polycrystalline ceramic of Y-PSZ used in a system in which the restoration is completely CAD/CAM fabricated; Cercon (Dentsply, Degudent Rodenbacher, Hanu, Germany),a polycrystalline ceramic, Y-PSZ, the restoration being CAD fabricated from a scanned wax pattern; Turkom-Cera (Turkom-Ceramic, (M) SDN. BHD, 238 Jalan Tun Razak, 50400 Kuala Lumpur, Malaysia), a high purity aluminium oxide used to produce restorations through conventional processes using indirect laboratory procedures. Two groups of test specimen discs were prepared from each material. The dimensions were as follows (Figure 1):


Turkom-Cera:
16 samples of 1.2mm thickness and 16mm diameter 16 samples of 2mm thickness and 16 mm diameter
LAVA:
16 samples of 1.2mm thickness and 16mm diameter 16 samples of 2mm thickness and 16mm diameter
Cercon:
16 samples of 1.2mm thickness and 16mm diameter
16 samples of 2mm thickness and 16mm diameter
Biaxial flexural strength was tested using a Zwick Z010 electronic hydraulic testing frame (Wirsam Scientific and Precision Equipment (Pty) Ltd.). The reliability of strength was also compared using Weibull Moduli as described in the studies by Pittayachawan et al., and Wagner and Chu.9,39
• (LAVA and TurkomCera samples were sponsored by the respective manufacturers. Cercon samples were purchased directly from manufacturer.)
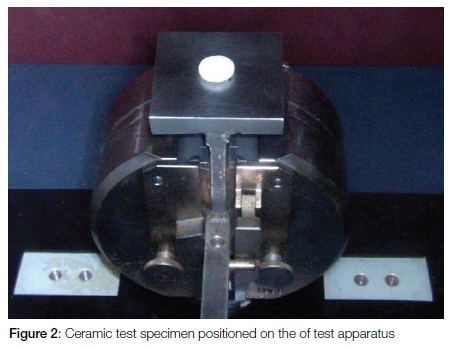
The test apparatus (Figure 4) is made up of a specimen placement surface consisting of three steel ball bearings (4mm in diameter), positioned in a circular arrangement, 120 degrees apart, on a support table (10mm diameter). Each disc specimen is placed centrally on the table (Figure 2). The upper arm is the loading table which exerts the required force to the test specimen from above, via a loading pin with a 1mm radius tip (Figure 3). A cross head speed of 1mm/min was set and each specimen was loaded until fracture occurred. The load at failure (N) of each specimen was noted as a measure of the biaxial flexural strength.


Statistical analysis and recording of data
The test results were automatically recorded and saved using the software program Testexpert, which is linked to the Zwick Z010 Electronic Hydraulic testing machine. Strength values were analysed with an analysis of variance (ANOVA) and Scheffe tests at a significance level of 0.05. In addition, Weibull moduli were calculated to assess variability between samples from the same manufacturer. A high value demonstrates homogeneity between the samples. After failure, all specimens from each company were collected and photographed under a light microscope in order to be able to describe the patterns of failure.
RESULTS
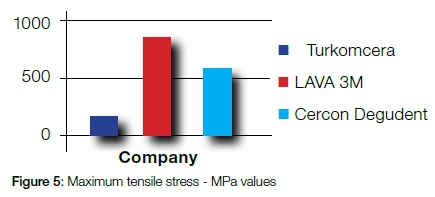
There were statistically significant differences noted in the biaxial flexural strength between each of three materials tested (Figure 5). Turkom-Cera had the lowest value (155.71 MPa), Cercon was higher (586.92 MPa), and LAVA was the highest (866.44 MPa).
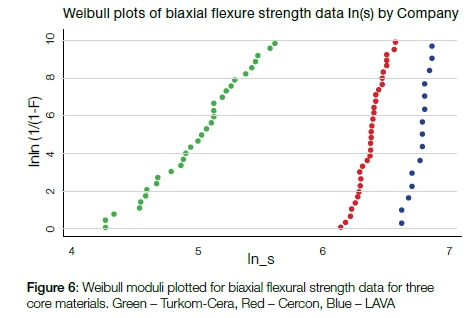
The Weibull moduli were calculated as 4.98, 6.76, and 6.37 for Turkom-Cera, LAVA and Cercon, respectively (Figure 6). The high values for LAVA and Cercon demonstrate that these materials are reliable and that there is consistency between samples. Turkom-Cera had a much wider range of strength between samples. The most consistent range was seen with LAVA (Figure 6).
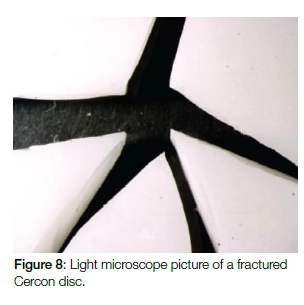
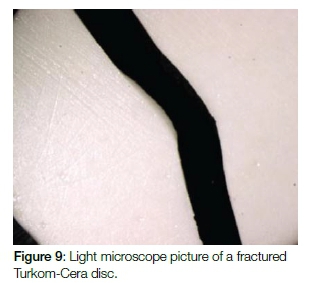
All fractured samples were realigned and spaced, and then viewed under a light microscope. The patterns of fracture were described in an attempt to analyse conformity between materials. While LAVA and Cercon demonstrated similar patterns of multiple fractures Turkom-Cera exhibited a pattern of fewer fractures (Figures 7, 8 and 9).

DISCUSSION
The preference of patients for metal-free restorations, and their high aesthetic demands, are fundamental factors influencing treatment planning and restorative options. This in turn has led to major advances in the development, production and use of dental ceramics.42,43 Due to the inherent brittle nature of these ceramics, the materials generally handle compressive forces better than they do the tensile stresses induced during mastication.41
It has been reported that while the average chewing force in posterior sites is about 350N, this can rise to over 1200N in severe bruxers.34 The strength of the core material which supports the overlying porcelain is a key factor in determining the long-term success of ceramic restorations.40,41 For this reason it is relevant that the flexural strengths of available high-strength ceramic core materials be tested to guide selection and techniques.
Three point, four point and biaxial flexural strength tests have been used for dental ceramics.40 The three point bending test, although extensively used, is influenced by the microstructure of the edges of the sample.34 The biaxial flexural strength test used in this study focused on the central area of the samples thus avoiding inaccuracies from irregular edges.34
The results of this in-vitro test showed significant differences between all three materials tested. Turkom-Cera ceramic core (high purity Al2O3) had the lowest mean biaxial flexural strength (155.71 MPa), LAVA ceramic core (Y-PSZ) the highest (866.44 MPa), and Cercon ceramic core (Y-PSZ) had an intermediate mean value (586.92 MPa). These differences suggest a significant superiority of partially stabilized zirconia over high purity Al2O3. Despite the relatively low value of Turkom-Cera, all three of the tested ceramic core materials had higher strength values than the older silica based ceramic systems.
The strength values found in this study were lower than those previously reported in the literature, which is an inexplicable concern. These were in the range of 900-1200 MPa for yttrium partially stabilized zirconia and 487-699 MPa for densely sintered high purity Al2O3.4 Another study by Yilmaz and Aydin, which compared six different all-ceramic materials, found the mean biaxial flexural strength of Y-PSZ and aluminum-based glass infiltrated ceramics to be 1140.89MPa and 341.89MPa respectively.34
The Weibull analysis revealed that Turkom Cera had a wide range of strength values between individual samples, while LAVA exhibited the most consistency, followed by Cercon. In addition, the fracture patterns for LAVA and Cercon were very similar to each other and in strong contrast to those of Turkom-Cera. There is a scarcity of literature regarding the relevance of patterns of fracture of ceramic materials, and this may be a suitable focus for future research.
Inadequate core material has often been cited as the reason for failure of all-ceramic restorations, as the core is the foundation that reinforces the overlying porcelain veneer. The biaxial flexural strengths of LAVA and Cercon as found in this study approximated the strength of metal substructures, and satisfy the suggested strengths required for use in the posterior segments of the dentition. Turkom-Cera, however, did not demonstrate sufficiently high strength values and its application for restorations on posterior teeth may therefore be limited.
Another factor of concern was the difference in biaxial flexural strength of samples of the same material but produced by different manufacturers. This may be attributable to a lack of standardization with regard to the software and the processing employed for the production of Y-PSZ. However, before any definitive clinical recommendations can be made, these in-vitro results should be verified with long term clinical studies.
CONCLUSION
Within the confines of this study, it can be concluded that LAVA, Cercon and Turkom-Cera display significantly different biaxial flexural strengths. Y-PSZ presented with higher strengths compared with high purity Al2O3. It can further be concluded that the biaxial flexural strength of the Y-PSZ samples in this study is manufacturer dependent. The results of this in-vitro study highlight the need for long term clinical studies aimed at assessing the strength of newer core materials.
Acknowledgements and Conflict of interest
The authors thank 3M ESPE and Turkom-Ceramic for donating the LAVA and Turkom-Cera test material. Cercon samples were purchased directly from the manufacturer. No conflict of interest is declared with respect to the donated test material.
ACRONYMS
CA: computer-assisted design
CAM: computer-assisted manufacturing
Y-PSZ: yttrium - partially stabilized zirconia
References
1. McCabe JF, Walls AWG. Applied Dental Materials. 8th ed. 1998; 77-83. [ Links ]
2. Yoshinari M, Derand T. Fracture strength of all-ceramic crowns. Int J Prosthodont 1994; 7: 329-38. [ Links ]
3. Griggs JA. Recent advances in materials for all-ceramic restorations. Dent Clin N Am. 2007; 51:713-27. [ Links ]
4. Raigrodski AJ. Contemporary materials and technologies for all-ceramic fixed partial dentures: A review of the literature. J Prosthet Dent. 2004; 92;557-62. [ Links ]
5. Pittayachawan P, McDonald A, Petrie A, Knowles JC. The biaxial flexural strength and fatigue property of LAVA Y-TZP dental ceramic. Dent Mater. 2007; 23:1018-29. [ Links ]
6. Pilathadka S, Vahalova D, Vosahlo T. The Zirconia: a new dental ceramic material. An overview. Prague Medical Report. 2007: 108(1); 5-12. [ Links ]
7. Al-Makramani BM, Razak AA, Abu-Hasan DI. Comparison of the load at fracture of Turkom-Cera to Procera All-Ceram and In-Ceram all ceramic restorations. J. Prosthodont. 2009;178:484-8. Available from: http://www.turkom-cera.com [Accessed 25 October 2008] [ Links ]
8. Yoshinari M, Derand T. Fracture strength of all-ceramic crowns. Int J Prosthodont 1994; 7: 329-38. [ Links ]
9. Griggs JA. Recent advances in materials for all-ceramic restorations. Dent Clin N Am. 2007; 51:713-27. [ Links ]
10. Minguez C, Lyons K. Failure of crowns and bridges - a review of the literature. New Zealand Dental Journal. 2007; 1:7-13. [ Links ]
11. Schmidseder J. Aesthetic Dentistry. Thieme; 2000;pp 5-6. [ Links ]
12. Preston JD. Perspectives in Dental Ceramics. 1988; pp 156-7. [ Links ]
13. Wall JG, Cipra DL. Alternative crown systems: is the metal-ceramic crown always the restoration of choice? Dent Clin N Am. 1992; 36(3):765-82 . [ Links ]
14. McLean JW. Alumina reinforced ceramics special applications. In: The Science and Art of Dental Ceramics. Vol.2: Bridge design and laboratory procedures in dental ceramics. Chicago: Quintessence; 1982;474-9. [ Links ]
15. Ahmad I. Protocols for Predictable Aesthetic Dental Restorations. Blackwell Munksgaard. 2006, pp 55-76. [ Links ]
16. Davies T. Clinical efficacy of all-ceramic crowns: The experience of a general practitioner. Compendium of Continuing Education in Dentistry. 1985: 6;744-9. [ Links ]
17. Dong JK, Luthy H, Wohlwend A, Scharer P. Heat pressed ceramics: technology and strength. Int J Prosthodont. 1992: 5(1);9-16. [ Links ]
18. Schweiger M, Holand W, Frank M, Drescher H, Rheinberger V. IPS Empress 2: a new pressable high strength glass ceramic for aesthetic all ceramic restorations. Quintessence Dent Technol. 1999; 22:143-51. [ Links ]
19. Fradeani M, Aquilino A, Corrado M. Clinical experience with In-Ceram Alumina and Spinell crowns: 5 year follow up. Int J Periodont Rest Dent. 2002: 22(6);525-33. [ Links ]
20. Seghi RR, Sorensen JA. Relative flexural strength of six new ceramic materials. Int J Prosthodont. 1995: 8;239-46. [ Links ]
21. Probster L. Survival Rate of In-Ceram Restorations. Int J Prosthodont. 1993; 6:259-63. [ Links ]
22. Hwang JW, Yang JH. Fracture strength of copy-milled and conventional In-Ceram crowns. J Oral Rehab. 2001; 28:678-83. [ Links ]
23. McLaren EA, White SN. Survival of In-Ceram crowns in a private practice: a prospective clinical trial. J Prosthet Dent. 2000;83:216-22. [ Links ]
24. Oden A, Andersson M, Krystek-Ondracek I, Magnusson D. Five year evaluation of Procera AllCeram crowns. J Prosthet Dent. 1998; 80:450-6. [ Links ]
25. Brunton PA, Smith P, McCord JF, Wilson NHF. Procera all-ceramic crowns: a new approach to an old problem. British Dent J. 1999; 186(9):430-4. [ Links ]
26. Zitzmann NU, Galindo ML, Hagmann E, Marinello CP. Clinical evaluation of Procera AllCeram crowns in the anterior and posterior regions. Int J Prosthodont. 2007; 20:239-41. [ Links ]
27. Odman P, Andersson B. Procera AllCeram crowns followed for 5 to 10.5 years: a prospective clinical study. Int J Prosthodont. 2001; 14:504-9. [ Links ]
28. May KB, Russell MM, Razzoog ME, Lang BR. Precision of fit: The Procera AllCeram crown. J Prosthet Dent. 1998; 80:394-404. [ Links ]
29. Kokubo Y, Ohkubo C, Tsumita M, Miyashita A, Vult Von Steyern P, Fukushima S. Clinical marginal and internal gaps of Procera AllCeram crowns. J Oral Rehab. 2005; 32:526-30. [ Links ]
30. McLaren EA, White SN. Glass-infiltrated Zirconia/Alumina-based ceramic for crowns and fixed partial dentures: clinical and laboratory guidelines. Quintessence Dent Technol. 2000:63-76. [ Links ]
31. Raigrodski AJ, Chiche GJ, Potiket N, Hochstedler JL, Mohamed SE, Billiot S, Mercante DE. The efficacy of posterior three unit zirconium oxide- based ceramic fixed partial dental prostheses: a prospective clinical pilot study. J Prosthet Dent. 2006;96:237-44. [ Links ]
32. Kohal RJ, Klaus G. A Zirconia Implant-Crown System: a case report. Int J Periodontics Restorative Dent. 2004; 24:147-53. [ Links ]
33. Suttor D. Lava Zirconia crowns and bridges. Int J Computerized Dent. 2004; 7:67-76. [ Links ]
34. Yilmaz H, Aydin C. Flexural strength and fracture toughness of dental core ceramics. J Prosthet Dent. 2007; 98: 120-8. [ Links ]
35. Sailer I, Filser F, Gauckler LJ, Hammerle CHF. Prospective clinical study of zirconia posterior fixed partial dentures: 3 year follow-up. Quintessence Int. 2006; 37:685-93. [ Links ]
36. Attia A, Abdelaziz KM, Freitag S, Kern M. Fracture load of composite resin and feldspathic all-ceramic CAD/CAM crowns. J Prosthet Dent. 2006; 95:117-23. [ Links ]
37. De Jager N, Pallav P, Feilzer AJ. The influence of design parame ters on the FEA- determined stress distribution in CAD/CAM produced all-ceramic dental crowns. Dent Mater. 2005; 21:242-51. [ Links ]
38. Wiedhahn K, Kerschbaum Th, Fasbinder DF. Clinical longterm results with 617 Cerec veneers: a nine-year report. Int J Computerized Dent. 2005; 8:233-46. [ Links ]
39. Wagner WC, Chu TM. Biaxial flexural strength and indentation fracture toughness of three new dental core ceramics. J Prosthet Dent. 1996; 76:140-4. [ Links ]
40. Ban S, Anusavice KJ. Influence of test method on failure stress of brittle dental materials. J Dent Res. 1990; 69(12):1791-9. [ Links ]
41. Hsueh C-H, Luttrell CR, Becher PF. Analyses of multilayered dental ceramics subjected to biaxial flexural tests. Dent Mater. 2006; 22:460-9. [ Links ]
42. Donovan TE. Factors essential for successful all-ceramic restorations. JADA. 2008; 139:14s-18s. [ Links ]
43. Toksavul S, Turkun M, Toman M. Esthetic enhancement of ceramic crowns with zirconia dowels and cores: A clinical report. J Prosthet Dent. 2004; 92:116-9. [ Links ]
 Correspondence:
Correspondence:
Leanne sykes:
E-mail: Leanne.sykes@up.ac.za

