










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.72 n.1 Johannesburg Feb. 2017
RADIOLOGY
Maxillo-facial radiology case 147
CJ Nortjé
BChD, PhD, ABOMR, DSc. Faculty of Dentistry, University of the Western Cape
Below are cases of cutaneous extra oral sinus tracts/fistulas presenting in the maxillofacial region. A proper diagnosis is important and forms a key to the successful management of these sinus tracts/fistulas in the head and neck region.
INTERPRETATION
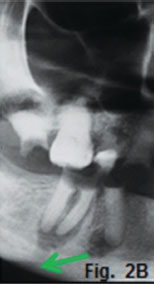
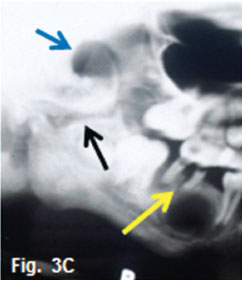
Fig 1A and B demonstrates an example of an infection of the canine fossa. The infection is commonly caused by the spread of infection from the maxillary canine and premolars. Fig. 1B shows a slight widening of the periodontal ligament space (Red arrow) suggestive of an apical infection. The canine fossa contains considerable connective tissue and fat, which allow accumulation of tissue fluids and pus between. These infections are most often controlled with antibiotics. However if the infection becomes localised, drainage is indicated. In the second case the patient presented for treatment of a lesion of her right mandible (Fig. 2A) which have been present for many months. The cropped radiograph (Fig.2B) demonstrates two root rests of a molar tooth with a draining sinus perforating the cortex (green arrows). After removing the root rests the lesion disappeared spontaneously within three weeks. A diagnosis of a cutaneous odontogenic fistula was made. The third case, a 12-year old boy, presented with a six year history of a septic draining sinus in the right temporal region (Fig. 3A).The patient had had his first infection of the right infra orbital region when he was one day old. Since that time he had five surgical procedures, which included craniotomies of the temporal region as well as a condylectomy for treatment of an ankyloses of the right TMJ. On examination, a 2x2 cm opening was found in the right temporal region; (Fig.3B). The patient could not open his mouth. The cropped pantomograph (Fig. 3C) showed an apical cystic lesion in the 46 region (yellow arrow), previous attempted condylectomy scar (black arrow) and the presence of a temporal sinus tract (blue arrow). The first surgical procedure involved removal of all infected focal areas of dental origin. This resulted in uneventful healing of the sinus tract (Fig.3D). A successful condylectomy was performed a few weeks later. Orofacial fistulas are not common but intraoral sinus tracts due to dental infections are common. If the tooth causing the problem is treated endodontically or by extraction the lesion will resolve.






Reference
1. Butow K-W, Vogel H, Grotepass FW. Temporal sinus tracts arising from mandibular fractures. American Association of Oral and Maxillofacial Surgeons. 1982;40 (1) : 56-9. [ Links ]
2. Thoma Kurt H. Oral Surgery.CV Mosby, 1963: p 736-37. [ Links ]
 Correspondence:
Correspondence:
CJ Nortjé
E-mail: cnortje@uwc.ac.za

