










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.72 n.1 Johannesburg Feb. 2017
RESEARCH
Analysis of the need for, and scope of training in, maxillo-facial prosthodontics in the South African dental technology programme
KMP TsĭtãI; CP OwenII
IDental Technologist, Department of Sport, Rehabilitation and Dental Sciences, Tshwane University of Technology, Pretoria. South Africa
IIDepartment of Oral Rehabilitation, School of Oral Health Science, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
PURPOSE: To investigate the need for additional training for dental technologists in the field of maxillo-facial prosthodontics (MFP), and to try to seek consensus on the scope of that training.
METHOD: There were four phases: Phase 1 investigated current curricula; Phase 2, completion of questionnaires by students, qualified dental technicians and technologists, and clinicians; Phase 3, interviews with the Heads of the three Universities of Technology and the Heads of the department responsible for MFP at the four Dental Schools; and Phase 4, a Delphi survey amongst technicians and clinicians using questions derived from the previous phases.
RESULTS: There was widespread agreement that the current dental technology curriculum did not cover sufficient aspects of MFP to provide graduates with the required skills, and that a postgraduate course should be initiated. However, technicians agreed whilst clinicians were against, whether a maxillo-facial technologist should be permitted to work with patients and carry out clinical procedures. There was general consensus that a one-year full-time course was required.
CONCLUSIONS: A postgraduate course should be instituted to improve the training of dental technologists in MFP. The South African Dental Technicians' Council should initiate workshops to determine the curriculum, and the regulation of the maxillo-facial technologist.
Keywords: maxillo-facial prosthodontics; dental technologist; scope of practice; education and training; postgraduate course.
INTRODUCTION
Craniofacial defects are severely debilitating, both physically and psychologically and the provision of rehabilitation prostheses can make enormous differences to the quality of life of the patient. The support of the entire team of health care providers before, during and after surgical treatment and rehabilitation, is required and appreciated by afflicted patients.
In South Africa there are three Universities of Technology: Durban University of Technology (DUT), Tshwane University of Technology (TUT) and Cape Peninsula University of Technology (CPUT). These three Universities train dental technicians (via a three-year qualification leading to a National Diploma) and dental technologists (via a four-year qualification leading to a B-Tech degree). The question arises as to whether adequate training in MP is provided.
Maxillofacial Prosthetics is defined by the current Glossary of Prosthodontic Terms1 as follows:
"The branch of prosthodontics concerned with the restoration and/or replacement of the stomatognathic and craniofacial structures with prostheses that may or may not be removed on a regular or elective basis."
A maxillo-facial prosthesis (MP) is defined as: "any prosthesis used to replace part or all of any stomatognathic and/or craniofacial structure". An editorial note stated that "the taxonomy for maxillo-facial prostheses may include modifiers (adjectives) to provide descriptive evidence of the nature of the prosthesis including anatomic location, retention, support, time, materials, and form. Frequently, the means of retention is used, and may encompass descriptive adjectives tissue such as the adjacent tissue, teeth, dental/craniofacial implants, or a combination of such, thus appropriate terminology can include: tissue retained MP, tooth retained MP, implant retained MP, tissue/implant retained MP. Descriptive terminology may also be included to delineate time utilization for the prosthesis such as surgical, interim and definitive."
In the field of dental technology there has been controversy concerning the issue of dental technicians working directly with patients. A category of Clinical Dental Technologist was provided in the Dental Technicians Act (19 of 1945 as amended in 1979) for the treatment of edentulous patients only, but regulations putting this into effect were never promulgated. The present study is concerned with those dental technicians who provide a service, possibly involving clinical input, for patients requiring maxillo-facial prosthodontic rehabilitation.
Internationally, there are programmes which specifically train dental technicians in the field of maxillo-facial prosthodontics (MFP) who are then permitted to deal directly with patients. A good example is that of the UK, where dental technicians may be involved in the treatment of patients requiring MFP. At Kings College, London, Maxillo-facial and Craniofacial technology forms a two-year Masters programme open to dental technicians and to dentists, and both are registered with the General Dental Council (GDC).2
In the US the situation is similar, where such persons form a specialty of dental technology referred to as Anaplastologists, and many of the members of the International Anaplastology Association (IAA)3 have advanced academic degrees in medical, dental, and allied health fields. The majority have an extensive art background in addition to their scientific knowledge and profession. However, they are permitted to work directly with patients only on extra-oral appliances.
In South Africa, maxillo-facial prosthetic services are mainly provided at the four dental schools, and by a few private prosthodontic practices. Very few dental technicians/technologists in the country are trained or provide technical services in this field. Certainly at the dental schools there are long waiting lists and high workloads and there is clearly a need for such services to be expanded within the scope of dental technology and in the three Universities of Technology.
There are two inter-related aspects to this specialised field of MFP. The first is the adequacy of the training in this field, and the second is the question of whether there should be direct patient contact by the dental technologist. The aim of this study was to address these two challenges and to determine whether it is possible to reach consensus amongst the relevant role-players for solutions which may improve the services rendered to the increasing numbers of patients who require maxillo-facial rehabilitation.
METHOD
A survey research design was conceived involving both quantitative and qualitative techniques in which questionnaires were to be distributed and follow up interviews conducted where necessary. Ethical clearance was obtained from the Research Ethics Committee of the Tshwane University of Technology, clearance reference number REC 2012/10/021. Following analysis of the results of these surveys, a questionnaire to be used as a Delphi study was devised. The study population included all specialist prosthodontic dental educators in South Africa, registered prosthodontists, prosthodontic registrars, the Heads and staff of the Departments of Dental Technology in the Technical Universities, registered dental technicians/technologists, and dental student technicians/technologists. (A note on terminology: a dental technician refers to a person who obtained a National Diploma in three years, and a dental technologist as one who obtained a BTech degree in four years.)
The study comprised four phases:
Phase 1: Curricula
The three Heads of Dental Technology were contacted and requested to provide their respective curricula. These were analysed to determine the timing and scope of training in maxillo-facial prosthodontics currently being undertaken.
Phase 2: Questionnaires
All questionnaires were piloted to improve the validity of the questions. The study populations were sent correspondence via e-mail, explaining the study and requesting their participation. All respondents were requested to complete the questionnaires via the Survey Monkey website, as this ensured the confidentiality and anonymity of the data. However, if respondents felt more comfortable with responding via e-mail, then confidentiality was assured by the anonymous transference of data. At least two follow-up e-mails were used to encourage a sufficient sample of at least 15% of the population.
Phase 3: Interviews
One of the authors (KPMT) visited each of the three Universities of Technology, having previously requested personal interviews with the Heads of the Departments of Dental Technology and the Heads of the Departments of Prosthodontics in each of the dental schools. Interview questions were structured around the questionnaires, and the interviewees' opinions on the current training, scope of practice, and possible future alternatives. The responses helped to form the basis of the questions and statements which were to be used in the Delphi study.
Phase 4: Delphi study
The Delphi technique is a method of obtaining consensus amongst a group of experts. First used and described by the RAND Corporation in the 1950s for technological forecasting,4 it is named after the Pythia, the High Priestess of the Temple of Apollo at Delphi, Greece.5 It is a technique which seeks to obtain group consensus by combining the opinions of participating experts who are responding to a series of questionnaires. The participants remain anonymous. The results of each round of questionnaires are fed back to the experts who are then again asked their opinion on any modifications that may have been made to the statements as a result of the previous round, and this process is repeated for two of three iterations.6-8 In this study, all statements receiving 70% or better agreement in the first round were accepted, and the remaining questions were re-formulated and similar agreement sought. It was found that sufficient consensus was obtained after two rounds, and a final proposal for training needs, the scope, and manner of MFP technology was formulated.
Data were analysed in SPSS (Statistical Package and Service Solutions Inc, Chicago, USA). A p-value ≤ 0.05 indicated a significant statistical difference at a 95% confidence interval. Cross tabulations, Pearson Product-Moment Correlation and descriptive statistics were used to analyse the data. Validity tests and reliability tests were also performed.
RESULTS
Phase 1: Curricula
Of relevance to this study are the topics in MFP, but unfortunately the curriculum documents received from DUT and CPUT did not specify particular details. It was assumed that maxillo-facial prosthetic topics were subsumed within the course "Dental Technology 4" in the last year of study, at least for CPUT. Students at DUT, however, confirmed that maxillo-facial prosthetics was not part of their curriculum.
Tshwane University of Technology has advanced subjects which form part of the BTech degree, and which include the manufacture of obturators, splints, hearing aids, and mouth-controlled appliances for disabled persons. However, the students reported that only two aspects are covered: the manufacture of an artificial eye, and obturators.
Phase 2: Questionnaires
The three Heads of Technology and the four Heads of Prosthodontic Departments all responded. Seventy percent of the dental specialists/registrars responded (21 out of 30), 60% (48 out of 88) of the dental technicians/technologists and 86% (215 out of 250) of the students. A large amount of data were collected for each of the groups, although not all will be included in this report for reasons of space. Of most interest are the areas where it was felt that opinions would help influence future outcomes and policies, and therefore data from the groups of respondents were pooled to investigate any trends in frequency distribution. In addition, comparisons between the responses of the clinicians and the dental technicians / technologists were carried out.
Pooled data
For pooled data only the responses of the Fourth Year dental technology students were included with that of the dental technicians / technologists, specialists and registrars, as it was felt the more junior students would not have sufficient insight and might therefore skew the outcomes. The areas investigated were:
• the need for training in maxillo-facial prosthodontics;
• the length of any additional training;
• where that training should take place;
• whether it should be a specialty of dental technology;
• the question of clinical contact of the maxillo-facial technician with patients;
• which statutory body should regulate maxillo-facial technicians should they be permitted patient contact.
The need for training in maxillo-facial prosthodontics and the length of training
Data were available only from the dental technicians/technologists, specialists and registrars, of whom 64% agreed that there was a need for training but were divided on the length, with the majority (59%) stating it should be of one year's duration.
Where additional training should take place
Data were available from all three groups, but the results were inconclusive: 46% felt it should be at both a Dental School and a University of Technology, 31% felt it should only be at a University of Technology, and 23% only at a Dental School.
Whether maxillo-facial prosthodontics should be a specialty of dental technology
Data were available from all three groups: 80% agreed that it should be a speciality.
The question of clinical contact of the maxillo-facial technician with patients
Data were available from all three groups, and 74% felt that there should be clinical contact with patients.
Which statutory body should regulate maxillo-facial technicians if they should be permitted patient contact?
Data were available from all three groups, and the majority (57%) felt there should be joint regulation between the HPCSA and the SADTC.
Comparative Data
For the comparative data, the responses of the Fourth year dental technology students were included with the dental technicians / technologists and compared with those of the specialists and registrars. The areas investigated were:
• the question of clinical contact of the maxillo-facial technician with patients;
• the length of any additional training;
• where that training should take place;
• which statutory body should regulate maxillo-facial technicians if they should be permitted patient contact.
The question of clinical contact of the maxillo-facial technician with patients
Responses to the two relevant questions are shown in Table 1. The term 'Technicians' refers to the Fourth year students and the dental technicians/technologists; the term 'Clinicians' refers to the specialists and registrars.
The length of any additional training
The comparative responses are shown in Table 2. In this case, the responses excluded the students of dental technology. There was a statistically significant difference (χ2=11.77, p=0.008) in the overall responses between the technicians and clinicians.
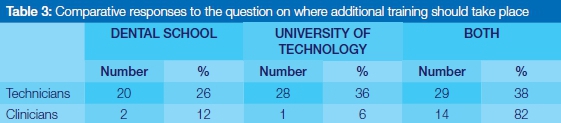
Where additional training should take place
The comparative responses are shown in Table 3. There was a statistically significant difference (χ2=11.48, p=0.003) in the overall responses between the technicians and clinicians.
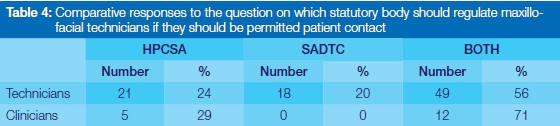
Which statutory body should regulate maxillo-facial technicians if they should be permitted patient contact?
The comparative responses are shown in Table 4. There was a statistically significant difference (χ2=17.46, p<0.001) in the overall responses between the technicians and clinicians.
Phase 3: Interviews
Universities of Technology: Heads of Department: summary
The Heads of Dental Technology seemed to agree that currently the syllabus or training does not equip the students with the full scope of MFP. The syllabus aimed to provide basic training, but only to a limited degree. The Heads agreed that MFP should be an elective course for those students who want to pursue this field and that successful candidates should became specialised maxillo-facial prosthetists. However, all expressed concerns about the cost implications for a postgraduate course.
Heads and Specialists in the Dental Schools: summary
There was common agreement that a full-time specialised course for maxillo-facial technicians was necessary and that this would help cope with the obvious need. All clinicians felt that the maxillo-facial technician should have some clinical exposure and knowledge, but when doing clinical work this should be done together with the prosthodontist and not independently.
Phase 4: Delphi study
Questionnaires were sent by email to each of the Universities of Technology as well as to technologists known to be active in the field. Nine questionnaires were sent out and four responses were received (44%). One was from a University of Technology Head, one from a technician working in a Dental School, and two from technicians active in making maxillo-facial prostheses. To target prosthodontists, 46 questionnaires were sent out to each of the dental schools as well as to members of the Academy of Prosthodontics of South Africa. Nineteen responses were received (41%) from the first round, and 18 from a second round. All responses were entered anonymously into an MS Excel® spreadsheet, including all the comments received.
Conclusions from Round 1
An extraordinary level of agreement was reached in the responses to certain questions. Delphi studies generally regard an agreement of more than 70% to be at a level sufficiently high to inform practical application to the issue in question. There was general consensus on a wide variety of issues (see Discussion) but some did require further exploration in the second round.
The main area where there was no clear consensus was the whole issue of clinical training and clinical contact for the maxillo-facial technician. Although Round 1 demonstrated agreement that the postgraduate training should not include clinical training, the respondents were divided on the issue of patient contact and team work with a clinician. The question needed further exploration to obtain clarity and to try to obtain consensus amongst the respondents. Therefore the relevant questions for Round 2 were re-formulated with regard to all the responses and comments from Round 1, sometimes to clarify those responses, sometimes to obtain more detail, and sometimes to seek consensus when there was none.
Round 2
The respondents were given the information of the results from the first round as a preamble to this second round. The reformulated questions were designed to provide greater clarity and perhaps to give guidance to what should be included in the postgraduate curriculum.
DISCUSSION
No evidence of studies on this topic could be found for South Africa, and it became clear that there is very little information available as to the extent of the need for maxillo-facial prosthodontic rehabilitation throughout the country. Further investigation is warranted.
Encouragingly, 68% of the students reported they were interested in MFP. Of the 205 answering positively to this question, 72% would take an expanded course in MFP were it to be offered immediately after qualification. Most, though, preferred to follow a part-time course, probably understandable after four years of study. The Universities of Technology should take note of this opinion. Most student respondents also agreed with the notion that MFP should become a specialty of dental technology. The responses of the dental technicians and dental technologists largely reflected those of the students. The majority (84%) expressed a need for further training, stating that that their training had been inadequate and 75% felt MFP should become a specialty of dental technology.
Although 81% of the dental technicians / technologists felt that they should be allowed to carry out direct clinical work, only 56% felt this could be done independently of the clinician, which perhaps is an expression of an understanding of the complexities (and complications) of independent clinical practice. The clinicians reflected this to a greater extent, as none agreed that dental technologists should carry out clinical work independently from the clinician. Given the inexperience of the technicians in this field and the experience of the clinicians, this result may not be so surprising. This would also have implications as to how the maxillo-facial technologist should be regulated, as clearly contact with patients would have to be regulated by the Health Professions Council of South Africa.
There was a 64% agreement amongst all respondents that there was a need for postgraduate training in MFP for dental technologists and 59% considered this should be a one year full time course. Amongst the combined group of dental technology students and the technicians / technologists, 80% agreed that MFP should become a specialty of dental technology.
The Delphi survey proved to be a very useful method to obtain consensus on a number of aspects but especially on what should be included in a postgraduate specialty course. Although many Delphi surveys accept a majority rating as agreement, it was felt that for this survey, 70% or better agreement would be representative of a need for change. A high level of agreement was reached to many of the questions from the first round which enabled formulation of the questions for the second round. Once again a high level of agreement was reached, thus obviating the need for a third round. The following are the positive statements which have been derived from both of the rounds, having 70% or better agreement:
• Training in maxillo-facial prosthodontics should be included in the undergraduate curriculum for dental technologists, but only at a basic level and only for the following:
• An intra-ocular prosthesis
• An extra-ocular prosthesis
• A nasal prosthesis
• An auricular prosthesis
• A maxillary bulb obturator prosthesis
• A speech appliance
• A cleft lip appliance
• Further training should be at the postgraduate level as an additional course and this should be done jointly with a Dental School.
• After receiving postgraduate training, the maxillo-facial dental technologist should be present where applicable in the clinical environment to assist the clinician.
• The maxillo-facial dental technologist should be permitted to place extra-oral appliances on their own without a clinician being present.
• The maxillo-facial dental technologist should be permitted to assist the clinician with the placement and adjustment of intra-oral appliances, but should be permitted only to adjust them out of the mouth and should not be permitted to work directly on the patient.
• Postgraduate training should include observational exposure of surgical procedures in the disciplines of Maxillo-Facial and Oral Surgery, ENT, and Plastic Surgery.
• The following should at least be included in the postgraduate training:
• An intra-ocular prosthesis
• Theoretical training in 3D radiography
• An extra-ocular prosthesis
• A nasal prosthesis
• An auricular prosthesis
• A maxillary bulb obturator prosthesis
• A speech appliance
• A cleft lip appliance
• Surgical obturators
• Mandibular defect appliances
• Implant-supported prostheses
• Training in software for digital planning
• Training in the use of Rapid Prototyping
• The science of the dental materials used in maxillo-facial prosthodontics
• If the postgraduate trained maxillo-facial dental technologists can have clinical contact with patients, regulation should be by both the SADTC and the HPCSA.
• If the postgraduate trained maxillo-facial dental technologist cannot have patient contact, regulation should be by the SADTC only.
CONCLUSIONS AND RECOMMENDATIONS
The consensus statements derived from the Delphi survey were largely in accordance with the questionnaire survey results, with the exception of the question of clinical contact. This was largely due to the fact that the Delphi respondents included more clinicians than technicians, and that the questionnaire responses showed that the technicians were more in favour of clinical contact.
All however, strongly agreed on the need for improved training in MFP at the undergraduate level and, more importantly, on the need for postgraduate training.
At present, there is no postgraduate training in dental technology, and although there is legislation which allows for a category of "clinical dental technologist" this was only for the treatment of edentulous patients.
Based on this, and the results from this study, the following conclusions and recommendations can be made:
1. There should be better communication between the Universities of Technology to (a) ensure a common curriculum with respect to maxillo-facial prosthodontics and (b) to open discussions on a postgraduate course.
2. A postgraduate course in maxillo-facial prosthodontics should be instituted, either as a full-time course or twice the length as a part-time course. This could result in a certification or a Diploma or even eventually as a recognised specialty of dental technology. This should be done in conjunction with the Dental Schools.
3. The course should include all the topics derived from the consensus reached in this study.
4. It is recommended that the South African Dental Technician's Council provides resources so that workshops may be initiated with the following role-players and stake-holders:
a. The three Universities of Technology
b. The four Dental Schools
c. The South African Dental Technician's Association
d. The South African Dental Association
The workshops should have the mandate to endeavour to define the curriculum; to decide on the scope and time required for a postgraduate course in maxillo-facial prosthodontics; to recommend regulations pertinent to the maxillofacial technologist; and to advise on a joint training programme including clinical observation and extra-oral contact.
Acknowledgements
The authors are most grateful for all the participants in this study for having taken the time and trouble to answer the questionnaires and to proffer their suggestions for the Delphi process. Thanks are due to Prof A Toriola of the Department of Sport, Rehabilitation and Dental Sciences, who assisted with the initial planning, sourcing of funding, and compliance with the requirements of the Tshwane University of Technology. Mr TS Ntuli assisted with the statistical analysis.
References
1. GPT 8.The glossary of prosthodontic terms, eighth edition (GPT-8). Journal of Prosthetic Dentistry 2005; 94:10-92. [ Links ]
2. Kings College.Maxillofacial & Craniofacial Technology. Available from http://www.kcl.ac.uk/prospectus/graduate/maxillofacial-technology/print [Accessed 22/05/2012]. [ Links ]
3. IAA. Education & Training 2012 [Online] Available from: http://www.anaplastology.org/education-training. [Accessed 23/04/2012]. [ Links ]
4. Dalkey N, Helmer O. An experimental application of the Delphi method to the use of experts. Management Science 1963; 9:458-46. [ Links ]
5. Hale JR, De Boer JZ, Chanton JP, Spiller HA. Questioning the Delphic Oracle. Science American 2003;289:57-63. [ Links ]
6. McKenna HP. The Delphi technique: a worthwhile approach for nursing? Journal of Advanced Nursing 1994;19:1221-5. [ Links ]
7. Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. Journal of Advanced Nursing 2000;32:1008-15. [ Links ]
8. Owen C.P. Guidelines for a minimum acceptable protocol for the construction of complete dentures. International Journal of Prosthodontics 2006;19:467-74. [ Links ]
 Correspondence:
Correspondence:
CP Owen
Department of Oral Rehabilitation, School of Oral Health Science
Faculty of Health Sciences, University of the Witwatersrand
7 York Road, Parktown 2193
Cell: +27 83 679 2205
Fax: +27 86 553 4800
E-mail: peter.owen@wits.ac.za


{kind=link}
{kind=link}