










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.72 n.1 Johannesburg Feb. 2017
RESEARCH
The self-perceived sources of stress among dental students at a South African Dental School and their methods of coping
A BhayatI; TK MadibaII
IBDS, MSc, MPH, M Dent (Community Dentistry). Department of Community Dentistry, School of Dentistry, Faculty of Health Sciences, University of Pretoria, South Africa
IIB Dent Ther, BDS, DHSM, MChD (Community Dentistry). Senior Lecturer and Head of Clinical Unit, Department of Community Dentistry, School of Dentistry, Faculty of Health Sciences,University of Pretoria, South Africa
ABSTRACT
INTRODUCTION: Dental students have reported that, as a result of the nature of the dental curriculum, they are under severe stress while studying.
AIM: to determine how students perceived the sources of stress and to identify the coping mechanisms used.
METHODS: This was a cross-sectional analytical study using a standardized self-administered questionnaire. All dental students registered in 2015 were invited to participate. All data was secured as confidential and anonymous.
RESULTS: Responses were received from 224 students (74%, of whom 26% were male). One third of responding males and 45% of responding females reported severe levels of stress. Clinical students reported a significantly higher (p=0.002) prevalence of severe stress over non-clinical students. The most common causes of severe stress were fear of failure (47%) and high workload (38%). The coping mechanisms included sleeping (64%) and watching television (55%). More than a quarter contemplated changing from Dentistry as a result of their perceived stress. Those who reported having severe stress were 1.8 and 2.1 times more likely to quit Dentistry or to commit suicide.
CONCLUSION: Females and clinical students reported higher levels of severe stress. Those with severe stress were significantly more likely to contemplate quitting Dentistry or suicide.
INTRODUCTION
Tertiary education leading to any qualification is often associated with high levels of stress.1,2 Stress can be defined as pressure, external demands and anxiety acting on an individual's mental and physical state and caused by a problematic external environment.3 The perception of stress depends on an individual's beliefs, knowledge, attitude and behaviour.2,4 Dental students reported considerably more stress symptoms while studying, were more anxious and showed higher levels of depression, obsessive-compulsive disorders and interpersonal sensitivity than age-matched controls.3 This could be due to a multitude of factors including self-efficacy beliefs, assigned workload and performance pressure.3,5 Additionally and importantly, dental students are faced with stress related to clinical sessions and patient management.3 These include late or failed patient appointments, clinical quotas, dealing with uncooperative patients, highly skilled technical work, academic capability and financial factors.1,5 These stressors can lead to absenteeism, poor academic results, unsatisfactory work ethic, substance abuse and depression.6-9
Previous studies related to stress among dental students focused mainly on clinical students without regard for pre-clinical classes.3 Some studies concentrated on only one gender or compared the results with studies on medical students while others focused solely on negative and harmful coping mechanisms.7,9 Most studies took into consideration the effects of coping on the health and/or grades of students but very few have determined the types of mechanisms best suited for dental students.10 Limited studies have been carried out and published in South Africa in the past, most of which have been done in the Western Cape and while the majority were on dental students, one involved oral hygiene students.2,5,10-12 However, none of these studies have examined the coping mechanisms employed by the students to help deal with the stressors.
The aim of the current study was to determine the self-perceived stress levels, sources and coping mechanisms at a dental school in Gauteng, South Africa. The results provide baseline information on local stressors among dental students and may assist in the implementation and evaluation of stress management programs, if these are required. The study is unique as it compares data between the different years of study and the gender on the stressors affecting the students and the coping mechanisms on which they relied.
METHODS
This was a cross sectional analytical study and all dental students registered at a Gauteng dental school during the 2015 academic year were invited to participate (n=301). A standardised validated questionnaire was used to elicit the prerequisite information.13 The questionnaire had been used in previous studies and as a result was not piloted nor modified in any way.14,15 It was hand delivered to each class and all students were invited to complete it anonymously. It consisted of four sections with 29 closed and three open-ended questions. The first section elicited information on the student demographics including age, gender and year of study. The second section was based on the stressors, the third on coping mechanisms and the fourth on possible interventions that students felt could be implemented.
Each student was asked to rate, based on their personal experience, a list of possible stressors as being responsible for either "low", "moderate" or "severe" stress in their daily lives. The items that received the highest number of "severe" stress responses were identified as the most common stressors among each class or cohort. The results were considered in two categories: pre-clinical (first and second year students) and clinical (third, fourth and fifth year students).14-16 This categorization was based on the fact that as students move into a clinical environment, they are required to treat patients, including the administration of anaesthetics, undertaking extractions, completing restorations etc. This transition and enhanced responsibility has been shown to be extremely stressful and as a result, many studies have separated the students into pre-clinical and clinical categories.14-16
All data were treated as strictly confidential and were entered and analyzed using the SPSS software package.17 Frequency distributions were utilised to identify the common stressors and the common coping mechanisms while the chi-square test was used to determine any association between the stressors and the gender and year of study. A logistic regression was done to identify behaviour patterns that were strongly associated with high levels of stress and for this analysis, "low" and "moderate" stress were combined to form one category while "severe" stress formed a second category.
RESULTS
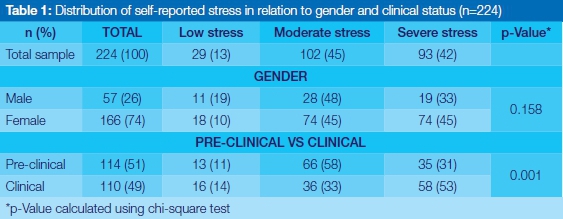
Of the 301 students registered in 2015, 224 (74%) completed the questionnaire satisfactorily. The majority of students were female (74%) and most of the respondents felt that they had either moderate (45%) or severe stress (42%). The association between the self-perceived levels of stress and the gender and clinical status is shown in Table 1. There were no significant differences in the levels of self-reported stress between male and female students (p=0.158). Almost half of the males (48%) reported having moderate stress and almost the same percentage of females reported either moderate (45%) or severe (45%) levels of stress. The clinical students reported a significantly higher prevalence of severe stress compared with pre-clinical students.
The most common stressors, the coping mechanisms and the strategies that could be used to reduce stress are listed in descending order in Table 2. (Many students selected more than one stressor and as a result, the combined percentages are greater than one hundred.) Overall, most of the students felt the fear of failure (47%) and an inability to keep up with the workload (37%) were the overiding stressors.

The most commonly used coping mechanism, irrespective of gender, was sleeping (64%), while 13% of students reported using recreational drugs to help cope. There were no significant differences in the coping mechanisms employed between males and females, however, more females (25%) felt that they became emotional when stressed compared with males (12%). More males (21%) compared with females (10%) disclosed that they were likely to use recreational drugs to help cope. Almost half of the students (46%) felt that the levels of stress could be reduced by decreasing the workload while 38% requested that lectures on how to deal with stress be included in the teaching curriculum.
The most common stressors, coping mechanisms and strategies that were used to reduce stress in relation to the clinical status are shown in Table 3.

Table 4 shows the breakdown of students who contemplated changing their course of study, quitting Dentistry or committing suicide as a result of stress. A significantly larger proportion of clinical students had considered quitting Dentistry compared with pre-clinical students (p=0.001). In general, males and clinical students were more likely to change their course, quit Dentistry or commit suicide.
The logistic regression identified three behaviour patterns as significantly associated with high stress levels (Table 5). Those with severe stress were almost twice as likely to consider quitting Dentistry (adjusted OR 1.84; CI -0.39-0.00) and more than twice as likely to contemplate committing suicide (adjusted OR 2.21; CI -0.90-0.13) compared with their counterparts. These results need to be interpreted with caution as the study utilised a cross sectional design.
DISCUSSION
The response rate was 74%, a result similar to previous studies. Missing were students who were absent or who did not complete the questionnaires satisfactorily. Almost three quarters were female, representative of the gender profile of the registered students.
The majority of the respondents reported having either moderate (45%) or severe stress (42%) which was in accordance with other published studies.18 The clinical students reported significantly higher levels of severe stress compared with the pre-clinical students and this was in accord with other studies.19 The high levels of severe stress among clinical students has been attributed to stress that is caused by clinical procedures, clinical quotas, failed appointments and other patient- related issues.3,5,19
Almost half of the females (45%) in the current study reported having 'severe' stress compared with 33% of the males (Table 1) and a quarter of all females (25%) reported becoming emotional as a result of stress. This could be related to different psychological characteristics, with females tending to express their concerns more freely than do males who are constrained by their perceived masculinity and ego status.20,21
Irrespective of the gender or the clinical status, the most common perceived stressor was the fear of failure and examinations (Tables 2 and 3) which was consistent with the findings of other studies.5,19,20 More than half (52%) of the pre-clinical students were afraid of failing their examinations (Table 3) possibly as a result of the transition from a school to a tertiary environment (and perhaps their inability to manage their time adequately). Considerably more clinical compared with pre-clinical students (31% versus 15%) felt that there was too much work outside lecture times which resulted in severe stress (Table 3). This could be related to the demands of clinical quotas and the tensions of treating patients which often takes up considerable periods of time, as reported by previous studies.5, 14,18
Stressors such as receiving criticism and the pressures of financial responsibilities were common for all students irrespective of gender and clinical status and have been shown to apply to students from other fields of study as well.1,12,22 Indeed a study carried out in 1982 had identified "sensitivity to criticism"" as the top stressor. Little appears to have changed.12
Almost two thirds (64%) of respondents claimed that sleeping helped them cope with stress. As suggested in other papers, this could be due to their exhaustion as a result of the perceived increased workload and patient demands.23
Other common coping mechanisms included watching television or movies, socializing with friends and physical exercise; these release options were similar to those described in previous studies.20,21
It is evident that programs need to be implemented to address the high stress levels experienced by the students. Many students (46%) perceived an overwhelmingly high workload. This combined with a request to include guidance on coping mechanisms in the undergraduate training should be of concern to dental academics and should be openly discussed in pursuit of solutions. Social activities have been shown to reduce stress24 and a quarter of students (25%) felt that such events would help them cope with their stress. This might be a viable option requiring minimal costs and infrastructure compared with other possible interventions.24
Of concern was the fact that 21% of males and 16% of clinical students reported the use of recreational drugs to help them cope with stress (Tables 2 and 3). Admittedly, a previous study carried out in 2002 in the United Kingdom, had reported a much higher prevalence of illicit drugs and alcohol abuse.7 Since then, knowledge and attitudes regarding drugs, alcohol and smoking have escalated. It is also possible, of course, that the current cohort did not answer honestly due to fear and the possible legal and social repercussions that may arise due to their disclosure.
Almost a third of all clinical students (Table 3) either wanted to change their course (31%) or to quit Dentistry (31%). This could be as a result of the burgeoning workload, high patient expectations and the number of clinical requirements demanded of them.
There were six students who had contemplated committing suicide as a result of stress associated with studying Dentistry. This serious discovery must be noted and appropriate stress management programs implemented.21
The students who reported having severe stress were 1.8 and 2.1 times more likely to quit Dentistry or to commit suicide as compared with those suffering moderate and low stress respectively. This confirms existing literature which highlights that dentists in general are unable to cope with stress and lack adequate stress-coping mechanisms.25 As a result many authors have suggested that the dental curriculum should include lectures on stress management, time management, communication skills and behaviour management.25,26 The respondents in the current study do in fact receive lectures on communication and time and practice management. However, these lectures are towards the end of the dental curriculum and perhaps should be moved to earlier on in the curriculum. This could help students cope with the current stress levels and also equip them to deal with stress in their future professional careers.
LIMITATIONS
These results were obtained from a single School of Dentistry in Gauteng and as a result are not necessarily representative of all dental students in South Africa.
CONCLUSION
Stress amongst dental students has been shown to be of considerable concern, with severe levels causing a few students to even contemplate suicide. Effective means of reducing stress should be explored together with determining effective methods of coping with the tensions.
RECOMMENDATIONS
Urgent intervention is needed to address the high levels of stress in order to prevent students from using recreational drugs and other unhealthy alternatives. It is recommended that stress management lectures are included early in the curriculum so that students are given the tools to help them cope with the increased demands of studying Dentistry. In addition, social activities such as sports days, regular social evenings, team building exercises etc. could be introduced which could help staff and students to interact and possibly create a more socially acceptable and stress-free friendly environment. The dental curriculum should be examined to identify areas which could be major causes of stress and methods devised to alleviate the problem as much as possible.
Acknowledgements
The author would like to thank the following dental students for their assistance in the questionnaire distribution and data collection: Knoetze, Khan, Randal-Smith, Peer and Smyth.
References
1. Campbell R, Svenson L, Jarvis G. Perceived level of stress among university undergraduate students in Edmonton, Canada. Percept Mot Skills 1992; 75(2): 552-4. [ Links ]
2. Gordon NA, Rayner CA, Wilson VJ, Crombie K, Shaikh AB, Yasin-Harnekar S. Perceived stressors of oral hygiene students in the dental environment. Afr J Health Professions Educ 2016; 8(1):20-4. [ Links ]
3. Paudel S, Subedi N, Shrestha A. Stress and its relief among undergraduate dental students in a tertiary health care centre in eastern Nepal. Dentistry 2013; 3(157). doi:10.4172/2161-1122.1000157. [ Links ]
4. Sandars J, R Patel, Steele H, McAreavey M. Developmental student support in undergraduate medical education: AMEE Guide No. 92. Medical Teacher 2014; 36(12): 1015-26. [ Links ]
5. Wilson VJ, Rayner CA, Gordon NA, Shaikh AB, Crombie K, Yasin-Harnekar S. Perceived stress among dental students at the University of the Western Cape. SADJ 2015; 70(6): 255-9. [ Links ]
6. Naidu RS, Adams JS, Simeon D, Persad S. Sources of stress and psychological disturbance among dental students in the West Indies. J Dent Educ 2002; 66: 1021-30. [ Links ]
7. Newbury-Birch D, Lowry RJ, Kamali F. The changing patterns of drinking, illicit drug use, stress, anxiety and depression in dental students in a UK dental school: a longitudinal study. Br Dent J 2002; 192(11): 646-9. [ Links ]
8. Sanders AE, Lushington K. Sources of stress for Australian dental students. J Dent Educ 1999; 63(9): 688-97. [ Links ]
9. K Aboulshamat, X Hou, E Strodl. Psychological well-being status among medical and dental students in Makkah, Saudi Arabia: A cross-sectional study. Med Teach 2015; 37: S75-S81. [ Links ]
10. Hendricks SJH, Joshi A, Crombie K, Moola MH. Perceived sources of stress among black dental students in South Africa. J Dent Educ 1994; 58(6): 406-10. [ Links ]
11. Naidoo S, Pau A. Emotional intelligence and perceived stress. SADJ 2008; 63(6): 148-51. [ Links ]
12. Cohen H, Hurwitz M, Lanesman B, Myburgh N, Prinsloo B. The perception and response to stress by dental students of the University of the Witwatersrand, Johannesburg. Diastema 1982; 16-21. [ Links ]
13. Westerman GH, Grandy TG, Ocanto RA, CG Erskine. Perceived sources of stress in the dental school environment. J Dent Educ 1993; 57(3): 225-31. [ Links ]
14. Polychronopoulou A, Divaris K. Perceived sources of stress among Greek dental students. J Dent Educ 2005; 69: 687-92. [ Links ]
15. Sanders AE, Lushington K. Effect of perceived stress on student performance in dental school. J Dent Educ 2002; 66(1):75-81. [ Links ]
16. Gorter R, Freeman R, Hammen S, Murtomaa H, Blinkhorn A, Humprhis G. Psychological stress and health in undergraduate dental students: Fifth year outcomes compared with first year baseline results from five European dental schools. Eur J Dental Ed 2008; 12(2): 61-8. [ Links ]
17. IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp. [ Links ]
18. Elani HW, Allison PJ, Kumar RA, Mancini L, Lambrou A, Bedos C. A systematic review of stress in dental students. J Dent Educ 2014; 78(2): 226-42. [ Links ]
19. Rajab LD. Perceived sources of stress among dental students at the University of Jordan. J Dent Educ. 2001; 65(3): 232-41. [ Links ]
20. Acharya SH. Factors affecting stress among Indian dental students. J Dent Educ 2003; 67:1140-8. [ Links ]
21. Al-Saleh SA, Al-Madi EM, Al-Angari NS, Al-Shehri HA, Shukri MM. Survey of perceived stress-inducing problems among dental students, Saudi Arabia. Saudi Dental Journal 2010; 22(2): 83-8. [ Links ]
22. Alzahem AM, Van der Molen HT, Alaujan AH, De Boer BJ. Stress management in dental students: a systematic review. Adv Med Educ Pract 2014; 5: 167-76. [ Links ]
23. Shaikh BT, Kahloon A, Kazmi M, Khalid H, Nawaz K, Khan NA et al. Students, stress and coping strategies: a case of Pakistani Medical School. Education for Health 2004; 17: 346-53. [ Links ]
24. Misra R, McKean M. College students' academic stress and its relation to their anxiety, time management, and leisure satisfaction. Am J Health Stud 2000;16(1):41-5. [ Links ]
25. Vanishree N, Jeswin J, Madhusudhan S. Suicide Amongst dentists - are you at risk? J Oral Health Comm Dent 2011; 5(3): 160-3. [ Links ]
26. Orner G, Mumma RD Jr. Mortality Study of Dentists: Final Report, December 30, 1976. Philadelphia: Temple University; 1976. [ Links ]
 Correspondence:
Correspondence:
Ahmed Bhayat
Departmwent of Community Dentistry. University of Pretoria
Tel: 012 319 2299
Cell: 084 020 9906
Fax: 012 323 7616
E-mail: ahmed.bhayat@up.ac.za


{kind=link}
{kind=link}