










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.71 n.10 Johannesburg Nov. 2016
RADIOLOGY CASE
Maxillo-facial radiology case 146
CJ Nortjé
BChD, PhD, ABOMR, DSc. Faculty of Dentistry, University of the Western Cape. E-mail: cnortje@uwc.ac.za
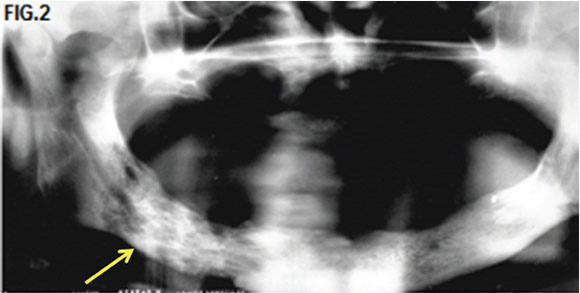
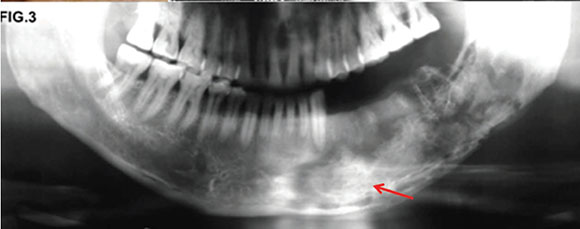
Below are a clinical picture and radiographs of patients who have been treated with radiation therapy for squamous carcinoma of the floor of the mouth.
INTERPRETATION
When radiotherapy is used in the treatment of malignant lesions in the oral cavity and related structures, detrimental changes of the mandible and maxilla are usually unavoidable. Osteoradionecrosis (ONR) is defined as bone necrosis secondary to radiation damage. Osteomyelitis does not occur until infection is introduced into devitalized bone. The classic sequence is radiation, trauma and infection. ONR is not a primary infection but a complex metabolic and tissue homeostatic deficiency caused by radiation-induced cellular damage. Micro-organisms only play a contaminant role, leading to superimposed osteomyelitis. ONR with osteomyelitis is more common in the mandible than the maxilla and more common in males than females. Patients usually have severe pain and swelling, with or without draining sinuses. There may be sloughing of the oral mucosa with subsequent exposure of large areas of bone (Fig.1). Note "moth eaten appearance " (yellow arrow, Fig.2).The cardinal radiological features include no changes in the early stages, progressing to areas of bone rarefaction, cortical destruction that is ill-defined resulting in a mixed sclerotic lucent pattern and sequestration, especially affecting the buccal bone( red arrow, Fig.3). Absence of soft tissue mass is an important feature in differentiating it from neoplastic recurrence, but the presence of soft tissue does not exclude osteoradionecrosis. In advanced cases pathological fractures may occur. Radiographically, the condition is indistinguishable from a rarefying osteomyelitis with a pure microbial origin. Therapeutically, prevention of infection of an irradiated bone is very important. Teeth in an area to be irradiated should be extracted10-14 days before irradiation. Primary closure of the mucous membrane is to be performed. Differential diagnoses include osteomyelitis and malignancies.

ACRONYM
ONR: Osteoradionecrosis
Reference
1. Farman AG, Nortjé CJ & Wood R E: Oral and Maxillofacial Imaging, 1st Ed, Mosby. St. Louis, Missouri 1993, p 206-7. [ Links ]
