










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.71 n.10 Johannesburg Nov. 2016
SEDATION
Continuous education in sedation: Is the current sedation continuum still relevant?
JA RoelofseI; C LapereII; G BoschIII
IMB.ChB, MMed, PhD, Dip NDBA (USA). Professor University of the Western Cape, Visiting Professor, University College London
IIMB.ChB, DipPEC, DA(SA), PDD. Sedation Practitioner
IIIBSc, MB.ChB, M.Fam.Med, Dip Sed. Sedation Practitioner, Sedation Solutions, London
INTRODUCTION
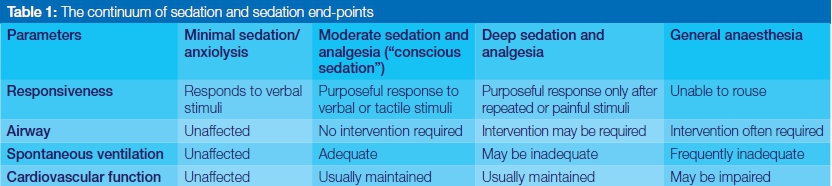
The differentiation of what is light and what is deep sedation is simplistic. Procedural sedation should be viewed as a continuum with many different possible clinical endpoints along the continuum, rather than having two end-points, mild versus deep sedation. The current sedation continuum differentiates these endpoints through patient responsiveness and other physiological parameters.
DISCUSSION
The goals of procedural sedation are first and foremost to consider patient safety and welfare as priority.1 The principles highlighted by the General Dental Council in the UK emphasize professional knowledge and competence, trust and putting first the interests of the patient. The onus is then greater and more comprehensive than we perhaps expected: it is not just about what the patient expects and needs (or pays for), but also what is expected of us as guardians of the safety of our patients.
Sedation is a drug-induced depression of consciousness, with a continuum that varies from minimal sedation/anxiolysis, and moderate sedation and analgesia, to deep sedation, and finally, general anaesthesia, as outlined in Table 1.2
Practitioners need to understand that increasing depths of sedation levels are associated with progressive respiratory depression and so the risks for potential adverse events increase. Simply put, the more drugs we give, the deeper becomes the sedation of the patient.3
Sedation levels are defined by the South African Society of Anaesthesiologists Sedation Guidelines, as well as internationally by various Sedation Societies.2,4 The graded levels of sedation accept that as the depth progresses, there is a corresponding need for expanded physiological monitoring, practitioner skills and rescue capability.3
The authors Green and Mason outlined the limitations of the current sedation continuum in terms of subjectivity, counterproductive effect and drug limitations. According to them, the current sedation continuum is vulnerable in terms of subjectivity due to its fundamental reliance on identifying and quantifying patient safety gauged on the response of the patient to verbal or tactile stimulation.5 The perceived responses are considered subjective and physicians are unlikely to consistently agree on the interpretation thereof, according to the authors. They also outlined the limitations due to patient factors, where patients are verbally or neurologically impaired, or, being developmentally compromised, would not be able to respond to tactile or verbal stimulation.
The counterproductive effect of continuously testing patient responsiveness is the fact that clinicians need to intermittently assess and reassess the patient, thereby disturbing the fundamental aim which is to induce anxiolysis, restfulness, amnesia and sleep. This leads then to the question whether sedation providers are in fact consistently and frequently reassessing the patients via response or whether the interpretation of the sedation level is made from observation only.
Certain drugs like ketamine and dexmedetomidine are thought to act independently of the continuum due to their fundamentally different nature and effects on patients during sedation. The dissociative state induced by the use of ketamine renders a patient to a trans-like state that cannot be judged alongside the normal continuum for other drugs.2
The optimal endpoint of any sedation should depend on the predicted level of pain or discomfort associated with the procedure, the level of anxiety of the patient as well as their cardio-respiratory reserve.1
Would it be possible to use the sedation continuum as a measure to keep patients safe, especially when the patients are fluctuating between moderate and deep levels of sedation? It is suggested that the sedation continuum should be a simplified frame of reference that can be used across the board to evaluate patient safety.
Tools that we can use alongside the continuum are sedation scales (Wilson and Michigan sedation scales), capnography and the Bispectral index (BIS) monitor.6 However, to make full use of both the Wilson and Michigan sedation scales to assess sedation depth, the patient's tranquil state is repeatedly disturbed via voice or touch. The use of capnography to monitor end-tidal carbon dioxide permits the sedation practitioner to assess the ventilatory status and provides the earliest indication of respiratory compromise.7 The BIS monitor can be used to follow depth of sedation of adults receiving propofol but further prospective studies need to be done to be able to incorporate the BIS monitor on clinical decision-making regarding differentiation between moderate and deep sedation.6 Other limitations also include children with various levels of developing brain function and with the use of other drugs, like ketamine.
According to Innes et al, who were considering sedation in the emergency department, patients respond differently to drugs and any sedative or analgesic has the possibility of causing cardiorespiratory compromise. Children, the elderly and patients with underlying cardiorespiratory disease carry a higher risk. Therefore, any patient can unexpectedly progress to a deeper level of sedation than intended. Sedation practitioners should not sedate patients unless they are confident in their ability to deal with all the possible complications that may arise.1
How do we, as practitioners, ensure that our patients are safe? Can the current continuum be transformed into a reference sequence that governs the safety of each individual? By accreditation and training of the sedation provider and the staff, by ensuring that the sedation environment and recovery area are properly equipped and by having systems in place to prevent human errors, we can ensure safe sedations to our patients.
The guidelines for sedation for medical and dental practitioners should remain unified and should clarify questions about monitoring modalities and provide updated information from the literature to further improve safety and outcomes for patients.4
Studies looking at the current continuum recommend not abolishing the original precept completely but propose an expansion by incorporating an objective mechanism to predict the ongoing risk of serious adverse events. The different levels in the continuum could be correlated, through research, with reference thresholds for the relevant physiological monitors. For each level could be identified the staff, training and equipment needed to meet the ongoing and escalating risks.8
The question is whether we are making the concept too complex - should it not just be a simple tool that is easy to remember and possible to be applied by all? On the other hand, if it were accurate in stratifying risk it would enable the correlation of sedation levels with associated risks. Such a system could become a very important tool for clinical governance, allowing for clinical practice audits, adverse event reporting and much more.
To put it concisely, any new continuum should be an integrated guideline that provides a standardized and evidence-based approach to base clinical decision-making while planning and proceeding with a sedation.8
The responsibility lies with the sedation providers, who are indeed the gate-keepers of adverse events. The sedation practitioner needs to be able rescue patients who unintentionally slip down the continuum.
New, validated, advances and development in physiological monitoring should be timeously integrated with the current parameters to improve and define the sedation continuum.8 These efforts will further increase patient safety and reduce morbidity as procedural sedation and the continuum of sedation are governed on an international, multidisciplinary front.
CONCLUSION
The current sedation continuum implies that sedatives are capable of inducing graded levels of consciousness anywhere along the spectrum. Implicit in this notion is the responsibility of the practitioner to carefully titrate and administer drugs to achieve the lowest possible level of sedation for the specific procedure planned.
ACRONYM
BIS: Bispectral index monitor
References
1. Innes G, Murphy M, Nijssen-Jordan C, Ducharme J, Drummond A. Canadian Perspectives. Science 1995;13(4):571-5. [ Links ]
2. Society of South African Society of Anaesthesiologists Sedation Guidelines 2015. Guidelines for the safe use of procedural sedation and analgesia for diagnostic and therapeutic procedures. 2015;21(2):1-38. [ Links ]
3. Krauss B, Green SM. Procedural sedation and analgesia in children. Lancet. 2006;367(9512):766-80. [ Links ]
4. Coté CJ, Wilson S, American Academy of Pediatrics, American Academy of Pediatric Dentistry. Law A, Ng D, et al. Guidelines for monitoring and management of pediatric patients before, during, and after sedation for diagnostic and therapeutic procedures: update 2016. Pediatrics [Internet]. 2016;45(2):180-5. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27354454 [ Links ]
5. Mason KP, Green SM. Reformulation of the sedation continuum. J Am Med Assoc. 2010;303(No 9):876. [ Links ]
6. Mason KP, Michna E, Zurakowski D, Burrows PE, Pirich MA, Carrier M, et al. Value of bispectral index monitor in differentiating between moderate and deep Ramsay sedation scores in children. Paediatr Anaesth. 2006;16(12):1226-31. [ Links ]
7. Miner JR, Heegaard W, Plummer D. End-tidal carbon dioxide monitoring during procedural sedation. Acad Emerg Med. 2002;9(4):275-80. [ Links ]
8. Green SM, Mason KP. Stratification of sedation risk - a challenge to the sedation continuum. Paediatr Anaesth. 2011;21(9):924-31. [ Links ]
 Correspondence:
Correspondence:
James A Roelofse
Private Bag X1, Tygerberg 7505
Tel: 021 937 3085,
Cell: 083 458 2427.
E-mail: jar@sun.ac.za

{kind=link}