










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.71 no.10 Johannesburg Nov. 2016
RESEARCH
Clinical and radiological features of 90 odontomas diagnosed in the Oral Health Centre at Sefako Makgatho Health Sciences University
V PeranovicI; CEE NoffkeII
IBDS, MDS (Maxillofacial and Oral Radiology). Lecturer, Unit Radiology, School of Oral Health Sciences, Sefako Makgatho Health Sciences University, South Africa
IIBChD, MSc (Maxillofacial and Oral Radiology). Professor, Unit Radiology, School of Oral Health Sciences, Sefako Makgatho Health Sciences University, South Africa
SUMMARY
This paper presents the variations in the clinical and radiological appearances of 90 odontomas diagnosed during routine radiographic examination in a population sample attending an African Dental Hospital. The majority occurred in males (1,4:1) and compound odontomas were more common than the complex type (3,2:1). The most frequent sites recorded were the anterior maxilla for the compound type and the posterior mandible for the complex type. The majority were associated with impacted permanent teeth (57.7%) followed by retention of deciduous teeth (16.6%), displacement of adjacent teeth (11.1%), expansion of the cortical plates (8.9%) and congenitally missing teeth (3.3%). More than 50% of the lesions presented with a radiolucent rim. Early removal is important in order to maintain the chronology of tooth development and to prevent extensive and costly intervention at a later stage.
Odontomas are exclusive to the tooth bearing areas of the jaws and are the most common benign odontogenic tumours.1 They develop from primordial odontogenic tissue. Due to their composition being a combination of odontogenic epithelium and odontogenic ectomesenchyme, odontomas are categorised in the mixed group in the 2005 World Health Organization classification of odontogenic tumours.2 Two types are recognised. Complex odontomas are described as malformations in which the dental tissues are arranged more or less in a disorderly pattern with little or no resemblance to normal teeth on radiographs. The compound type presents with normal dental tissues arranged in an orderly pattern giving rise to multiple small tooth-like structures called odontoids or denticles.3 Histologically, enamel, dentin, cementum and sometimes pulp tissue are present and although the individual tissue types may appear normal, their micro anatomical arrangement is abnormal.4 Due to their limited growth potential, odontomas are not true neoplasms but rather are developmental dental malformations behaving similarly to hamartomas.1
The aim of the present study was to analyse the clinical and radiographic features of odontomas diagnosed in an African population sample and to compare the findings with those of other studies.
MATERIALS AND METHODS
The records of the Unit Maxillofacial and Oral Radiology in the School of Oral Health, SMU were reviewed for odontomas diagnosed between 2013 and 2016 on digital dental radiographs. The unit serves mainly an urban and peri-urban Black population sample in the northern part of South Africa. All panoramic radiographs had been acquired by Sirona extraoral Orthophoss machines and digital software tools (Kodak Carestream) had been used for determining the actual sizes of the lesions. The diagnoses had been made on digital images and all surgically removed lesions had been submitted for microscopic examination. The names and hospital numbers of the patients were not recorded in this study and only the demographic data and radiological appearances were transferred to the data collection sheet to guarantee patient anonymity. The radiographic parameters that were recorded included the actual size, type (compound and complex), border, internal structure and influence on adjacent structures. The sizes were reflected in millimetres, margins were defined as the edge or periphery of the lesion with or without a radiolucent soft tissue capsule. The influence on adjacent structures included the effects on the bone and the teeth in the vicinity of the lesion. The differential diagnoses were recorded and elaborated on where relevant. Approval for the study was formally obtained from the Research and Ethics Committees of the hosting University (Certificate number: SMUREC/D/31/2016:PG).
RESULTS
A total of 90 odontomas were diagnosed during the study period. All images were retrieved from the archives of the Unit of Maxillofacial and Oral Radiology at SMU. Radiographs of diagnostic quality were available in all cases.
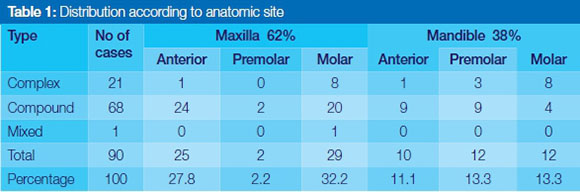
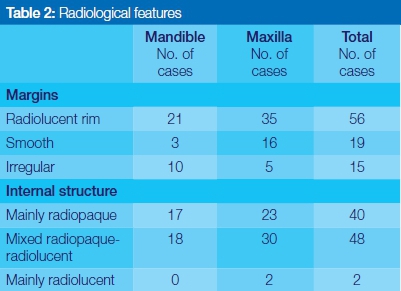
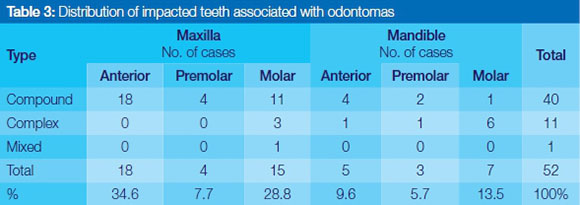
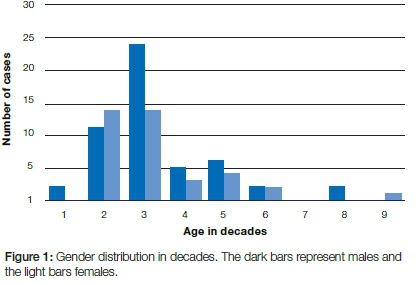
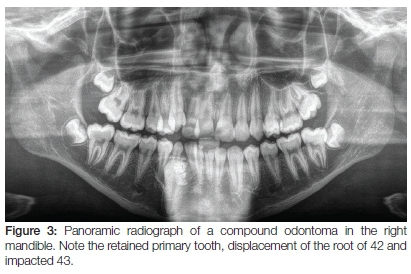
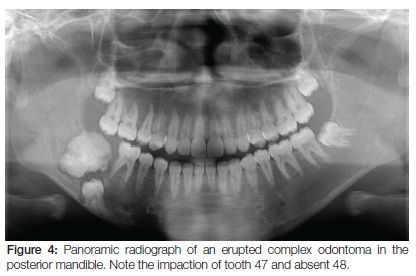
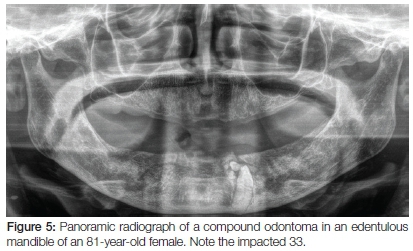
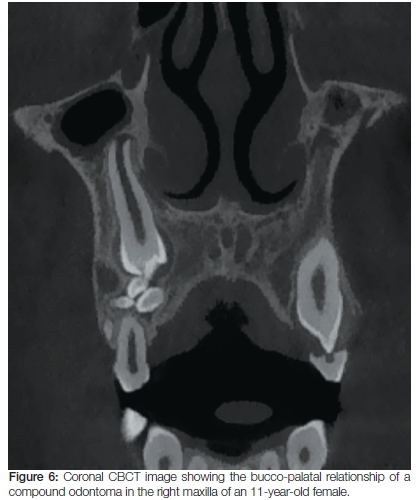
Thirty four compound, seventeen complex and one mixed odontoma occurred in males, while thirty four compound and four complex odontomas occurred in females. The distribution of the odontomas with relation to their anatomical site, radiological features and the distribution of associated impacted teeth are presented in Tables 1 to 3 respectively. The effects on adjacent structures were impaction of permanent teeth (52 cases, 57.7% of the sample), retention of deciduous teeth (15 cases, 16.6%), displacement of roots and/or teeth (10 cases, 11.1%), and congenitally missing teeth (3 cases, 3.3%). Resorption of tooth roots was not seen and expansion occurred in 8 cases (8.9%). Figure 1 shows the gender distribution and Figure 2 the distribution of complex and compound odontomas in the respective decades of life. Two images of typical compound and complex odontomas are shown in Figures 3 and 4 respectively. Figure 5 shows an edentulous mandible with a compound odontoma and Figure 6 presents a coronal CBCT section through a compound odontoma in the right maxilla. Pathological reports were available on 19 cases. The majority of patients were lost for follow-up and surgical removal.

DISCUSSION
Papers on odontomas generally appear in the literature as either case reports or as contributions to studies on larger series of odontogenic tumours. Few studies focus on odontomas only. These include 104 cases reported from Brazil,5 61 cases from Spain,6 73 cases from Korea,7 160- and 22 cases from Turkey,8,9 134 cases from Denmark10 and 39 odontomas in Japanese children.11 The only comprehensive clinico-pathological study on the African continent featured 19 cases reported from Libya in 2013.12
All cases in the present study had single lesions. Reports on multiple odontomas are rare with less than 20 cases recorded in the literature.13,14
In the present study all lesions were diagnosed and sub-classified accurately on radiographs and microscopic examination did not provide additional diagnostic information other than recording the presence of the different types of dental tissues. Compound odontomas were more than three times as common as the complex type, supporting the findings of most other reports.5,9,10,15 In fact only two studies were found which recorded a prevalence for the complex type odontomas.8,16 The tumours develop during childhood and adolescence and are most commonly diagnosed in the second decade of life.12 The ages of our patients at the time of diagnosis ranged between 6 and 81 years, with most odontomas (70%) found in the second and third decade (42.2% were diagnosed in the third decade and 27.8% in the second decade of life). The mean age at diagnosis was 28 years which is in accord with other studies.8,9
Variations in the gender distribution of odontomas are reported in the literature. Some studies show an equal gender distribution,7,12,17 others a predilection for females,6,9,18 while still others support the male predilection found in the present study.11,19 In some studies the compound variety affects the genders equally,12 while White and Pharoah1 found that the majority of complex odontomas occur in women. The equal gender predilection of compound odontomas found in the sample accords with the findings of the Libyan report.12 In the present study, a significantly higher occurrence of complex odontomas was found in males when compared with females. This is contrary to White and Pharoah1 who found that 60% of complex odontomas occur in women. In our study, females presented with significantly more compound odontomas (89.5%) than complex odontomas (10.5%) and males with more compound odontomas (65.4%) than the complex type (32.7%). Overall, 38.8% of all odontomas in the present study were located in the anterior region of the jaws, 62% occurred in the maxilla and 38% in the mandible. Significantly more compound odontomas (75.6%) were diagnosed than the complex type, with only one mixed odontoma in the maxillary molar region. The least frequent location for complex odontoma was the anterior region of both the maxilla and mandible.
Most odontomas are reported as incidental findings on radiographs taken for other indications such as delayed eruption of one or more permanent teeth or the retention of a deciduous tooth.5,7,12 Odontomas are characterized by their slow growth and non-aggressive behaviour. They enlarge during the normal development phase of the dentition and cease to grow after maturation of the associated corresponding teeth.1,2 If odontomas are not surgically removed, they will persist and may cause complications such as pain and tenderness in the associated area, particularly in denture wearers.20 In rare cases, eruption of the odontoma takes place20,21 resulting in trauma or infection and pain. Unerupted permanent teeth, supernumerary teeth or retained deciduous teeth are most commonly associated with odontomas.10,12 Philipsen et al., (1997) reported that an unerupted permanent tooth without a primary precursor is a clinical indication for the presence of an odontoma.10 In 88.7% of cases in the present study, odontomas affected adjacent teeth. It has been reported that 37-78% of all eruption disorders in the dentition are caused by odontomas.22
The most common effect on adjacent structures in this study, which occurred in 52 cases (57.7%), was impaction of an associated permanent tooth. This confirms the studies by Hidalgo-Sanchez et al. (2008) and Maeda (1987) who reported comparable findings.23,24 More impacted teeth were found in the maxilla (71.1%) than in the mandible (28.9%). The most frequently permanent teeth which were prevented from eruption by compound odontomas, were the maxillary incisors and canines. Complex odontomas caused impactions predominantly in the mandibular molar area, a finding which corresponds with the literature. Retention of an associated deciduous tooth was found in 16.6%, tooth displacement in 11.1% and congenital absence of a tooth in 3.3% of the total sample. Resorption of the roots of adjacent teeth was not present.
CBCT (3D Imaging with Cone Beam Computed Tomography) was the technique of choice to determine the borders of the lesions, expansion, thinning of the cortical bone, and perforation. Expansion of bone adjacent to the lesion was clinically observed and then confirmed on CBCT images in 8 cases (8.8%) and was predominantly associated with compound odontomas located in the mandible (5 cases). It is reported that large complex odontomas may also cause expansion of the cortical boundary1 which occurred in three cases in our study. No perforation of the cortical bone was detected on CBCT images in our sample. Radiologically the majority of odontomas in the present study were mixed radiolucent-radiopaque lesions surrounded by a radiolucent rim, as described in the literature.22 Only 15 cases presented with irregular borders. A lesser degree of radiopacity was noted for odontomas associated with the primary dentition.
The odontomas were treated by surgical excision and no recurrences had been reported up to the conclusion of the study. The small percentage of cases on which a pathology report was available indicates that either the specimen was discarded after removal, or patients refrained from returning for the removal due to the asymptomatic nature of the lesion. However, removal of the lesion is essential in preventing impaction and malpositioning of adjacent teeth.
CONCLUSION
Most odontomas in the present study were asymptomatic and were diagnosed as incidental findings during radiographic examination. The compound type occurred more frequently in the anterior maxilla and was more common than the complex type. The complex odontoma occurred more frequently in the posterior mandible. Early detection and excision are curative and prevent complications which may be detrimental to the development of the dentition.
References
1. White SC, Pharoah MJ. Benign tumours. In: White SC, Pharoah MJ, (eds.). Oral Radiology: Principles and Interpretation (7th ed.) Missourie: Mosby; 2014:370-4. [ Links ]
2. Barnes L, Eveson JW, Reichart P, Sidransky D (eds.). Pathology and Genetics of Head and Neck Tumours. Lyon: IARC Press; 2005:284 [ Links ]
3. Praetorius F, Piatelli A. Odontoma: complex type, Odontoma: compound type. In: Barnes L, Eveson JW, Reichart P, Sidransky D (eds.). Pathology and Genetics of Head and Neck Tumours. Lyon: IARC Press; 2005:310-11. [ Links ]
4. Budnick SD. Compound and complex odontomas. Oral Surg Oral Med Oral Pathol 1976; 42:501-6. [ Links ]
5. De Andrade Santos PP, Barroso KMA, de Souza LB, da Costa Miguel M MC, da Silveira EJD. Odontomas: Clinicopathologic study of 104 cases and a case report of compound odontoma associated with an unerupted maxillary central incisor in a child. Int Dent-Afr Ed 2 2012;32:9. [ Links ]
6. Amado Cuesta S, Garqallo AJ, Berini Aytes L, Gay Escoda C. Review of 61 cases of odontoma. Presentation of an erupted complex odontoma. Med Oral 2003;8:366-73. [ Links ]
7. An S-Y, An C-H, Choi K-S. Odontoma: a retrospective study of 73 cases. Imaging Sci Dent 2012;42:77-81. [ Links ]
8. Tekkesin MS, Pehlivan S, Olgac V, Aksakalli N, Alatli C. Clinical and histopathological investigation of odontomas: review of the literature and presentation of 160 cases. J Oral Maxillofac Surg 2012;70:1358-61. [ Links ]
9. Hakan A, Hakan K, Suer TB, Ozturk HP, Piskin B. The prevalence, anatomic locations and characteristics of the odontomas using panoramic radiographs. J Oral and Maxillofac Radiol 2015;3:49-53. [ Links ]
10. Philipsen HP, Reichart PA, Praetorius F. Mixed odontogenic tumours and odontomas. Considerations on interrelationship. Review of the literature and presentation of 134 new cases of odontomas. Oral Oncol 1997:33: 86-99. [ Links ]
11. Tomizawa M, Otsuka Y, Noda T. Clinical observations of odontomas in Japanese children: 39 cases including one recurrent case. Int J Paed Dent 2005;15:37-43. [ Links ]
12. Ingafou MSH, Elmurtadi AM. Clinico-pathological study of odontomas in 19 Libyan patients. J Dent Res 2013;10:592-5. [ Links ]
13. Sun L, Sun Z, Ma X. Multiple complex odontoma of the maxilla and the mandible. Oral Surg Oral Med Oral Pathol Oral Radiol 2015;120:e11-e16. [ Links ]
14. Erdogan O, Keceli O, Oztunc H, Evlice B, Altug HA et al. Compound odontoma involving the four quadrants of the jaws: a case report and review of the literature. Quint Int 2014;45:341-4. [ Links ]
15. Owens BM, Schuman NJ, Mincer HH et al. Dental odontomas: a retrospective study of 104 cases. J Clin Pediatr Dent 1997:21:261-4. [ Links ]
16. Tamme T, Soots M, Kulla A, Karu K, Hanstan S, Hanstein SM et al. Odontogenic tumours, a collaborative retrospective study of 75 cases covering more than 25 years from Estonia. J Cranio-Maxfac Surg. 2004;32:161-5. [ Links ]
17. Ladeinde AL, Ajayi OF, Ogunlewe MO, Adyema WL, Arotiba GT et al. Odontogenic tumors: A review of 319 cases in a Nigerian teaching hospital. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:191-5. [ Links ]
18. Mosqueda-Taylor A, Ledesma-Montes C, Caballero-Sandoval S et al. Odontogenic tumors in Mexico. A collaborative retrospective study of 349 cases. Oral Surg Oral Med Oral Path Oral Radiol Endod 1997;84:672-5. [ Links ]
19. Mamabolo M, Noffke C, Raubenheimer E. Odontogenic tumours manifesting in the first two decades of life in a rural African population sample: a 26 year retrospective analysis. Dentomaxillofac Radiol 2011;40:331-7. [ Links ]
20. Nisha D, Rishabh K, Ashwarya T, Sukriti M, Gupta SD. An unusual case of erupted composite complex odontoma. J Dent Sci Res 2011;2:1-5. [ Links ]
21. More CB, Tilor M, Varma SN, Adalja CJ, Zinzuvadia KG. Erupted compound odontoma- a rare report of two cases. Int J Oral Health Sci Adv 2014;2:42-6. [ Links ]
22. Mortazavi H, Baharvand M, Rahmani S, Jafari S, Parvaei P. Radiolucent rim as a possible diagnostic aid for differentiating jaw lesions. Imaging Sci Dent 2015;45:253-61. [ Links ]
23. Hidalgo -Sanchez O, Leco-Berrocal MI, Martinez-Gonzales JM. Meta-analysis of the epidemiology and clinical manifestations of odontomas. Med Oral Patol Oral Cir Bucal 2008;13:E730. [ Links ]
24. Maeda K. Clinical analysis of odontoma. Oral Radiol 1987;3:55. [ Links ]
 Correspondence:
Correspondence:
Vlasta Peranovic
Email: vlasta.peranovic@smu.ac.za
