










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.71 no.10 Johannesburg Nov. 2016
RESEARCH
Mandibular third molar and angle fractures: a meta-analysis
DP MotlobaI; LN MakwakwaII; A KhanIII; ML MacheteIV
IBDS, MPH (Epid), MDent (Comm.Dent), MBL. Head, Department of Community Dentistry. School of Oral Health Sciences, Sefako Makgatho Health Sciences University
IIBDT, BDS, Postgraduate Dip in Clinical Dentistry, MPH. Registrar: Community Dentistry. School of Oral Health Sciences, Sefako Makgatho Health Sciences University
IIIBDS, Msc, DHSM, Mchd (Comm.Dent). Senior Specialist: Community Dentistry. School of Oral Health Sciences, Sefako Makgatho Health Sciences University
IVBDS, ITLAR, Lecturer: Community Dentistry. School of Oral Health Sciences, Sefako Makgatho Health Sciences University
ABSTRACT
OBJECTIVE: To use a quantitative systematic review of available, credible literature to enable an estimation of the risk of mandibular angle fracture in the presence of mandibular third molars (M3s).
METHODS: Data were obtained through a systematic search of PubMed, Embase, and a thorough hand search of eligible references. Papers were included with: (i) acceptable methodological rigor; (ii) complete and accurate data. Details were recorded on the presence of third molars among the reported cases with or without angle fractures. Two calibrated researchers used a specially designed data abstraction form to independently populate information from the selected studies. Comprehensive Meta-Analysis software ver. 3.3.070 was used to calculate relative risk (RR) as the estimate of risk in this study.
RESULTS: Nineteen (19) retrospective cohort studies were analysed, comprising of 9888 patients with 3254 mandibular angle fractures. In the presence of mandibular third molars, the risk of mandibular angle fractures increases by 44% when compared with the risk in the absence of third molars.
CONCLUSION: The presence of mandibular third molars increases the risk of mandibular angle fracture. Clinicians should be discerning in identifying patients at increased risk, or those likely to benefit from appropriate prophylactic removal of wisdom teeth.
Keywords: mandibular fracture, third molar, meta-analysis
INTRODUCTION
The influence of the presence of mandibular third molars on the occurrence of angle fractures is imprecisely estimated, despite boundless research on this subject. This dearth of conclusive evidence has resulted in the inability of science to resolve the debate over whether there is ethical justification for prophylactic removal of asymptomatic mandibular third molars.1 Approximately half of all mandibular fractures affect the angle.2,3 This anatomical site is associated with the eruption of mandibular third molars, leading to the hypothesis that these teeth play a role in angle fractures.4,5 Significant consensus holds that the third molars act as space occupying organs, resulting in a weakening of the mandible, thereby contributing to an increased risk of fractures. The removal of wisdom teeth allows for bone deposition in the socket, resulting in a reduction in the occurrence of angle fractures.6
Epidemiological findings show that there is an increased risk of mandibular angle fractures among males, 30 years and younger.4,7 Other risk factors include: type of trauma, nature and direction of force and characteristics of the aetiological agent. Physical activities like contact sport events may involve low intensity impact, which if applied to the weakened mandibular angle could result in fractures. Automotive accidents, in contrast, may transfer high intensity force directly to the lesioned areas of the mandible, leading to a greater incidence of fractures.5
The quality of currently available literature on the relevance of third molars in mandibular angle fractures has been challenged in recent times. To date, no prospective cohort study has been conducted to ascertain the extent of temporal causality of fracture due to the presence of third molars. Methodological difficulties and ethical considerations do not justify such prospective research, hence the need to collate available evidence to reach conclusions. A recently published meta-analysis of retrospective cohort studies estimated a three times higher risk of angle fractures in the presence of third molars.6 While this result repeats previous findings reported in the literature, serious concerns persist regarding the validity of the conclusions, attributed to a significant degree of heterogeneity among included studies, and weak design factors.5,6
Understanding the role of third molars in mandibular fractures is paramount as this evidence could provide insight to the clinical approach and management of patients at "risk". Furthermore, research findings add value to the longstanding question about the prophylactic removal of asymptomatic wisdom teeth in the prevention of mandibular angle fractures.
Using available published literature, this study sought to estimate the relative risk of mandibular angle fracture in patients presenting with or without M3s.
METHODOLOGY
a. Search strategy and identification of studies
(i) Electronic databases, namely PubMed and Embase, were searched during the month of June 2016. General text terms and medical English keywords "angle fracture" or "mandibular angle fracture", "third molar" or "wisdom teeth", were used to locate articles that had been published between 1966 and 2016. The search was limited to original articles, reviews and meta-analyses. Gray literature, conference proceedings and other obscure publications were not considered for the purpose of this study. Instead, Cochrane reviews and references of retrieved studies were used to generate additional literature.
(ii) The inclusion criteria for this meta-analysis were based on the following study design properties: (a) Cohort studies: providing information on the incidence of fractures among cohort (presence of third molars) and controls (absence of third molars); (b) Case-control studies reporting the prevalence of third molars among cases (patients with mandibular fractures) and control (without mandibular fractures); (c) Cases (series): cumulated cases of patients with mandibular fractures, and diagnosis of third molars. (d) English language studies with complete and accurate information. Studies were excluded from this meta-analysis based on the following factors: (a) non-English; (b) inaccurate and incomplete data for quantitative analysis.
The principal researcher reviewed the titles and abstracts of retrieved studies in an initial determination of their inclusion into the meta-analysis. The final decision for inclusion was ratified by two more authors, and in case of disagreement, a full article was interrogated in order to reach a conclusion.
b. Appraisal and selection of studies
Full articles were thoroughly reviewed by two authors using a predetermined quality assessment tool. The components of each article were assigned a score of 1 to 3 with 1= poor; 2=moderate, and 3=good. Study characteristics, namely: study design; methodological rigor; how validity and reliability were addressed; sample size and completeness of data were scored. Articles achieving a cumulative score of 10 or more were included in the analysis.
c. Data collection and analysis
A Data abstraction form was used to collect information on (i) mandibular third molars (impacted or not), (ii) mandibular angle fractures, (iii) sample size, (iv) publication date and other related information. Collected data allowed for a computation of relative risk, with a 95% confidence for all studies and subgroups.
Cochran's test of homogeneity was undertaken based on inverse variance weights. Data from individual studies were pooled to estimate overall effect size. Subgroup analyses were undertaken to establish group differences with respect to the outcomes of interest. Two groups were created based firstly on sample size differences (more and less than 300 participants) and the second on assessed outcomes (angle fractures only; angle and condylar fracture). Comprehensive Meta-Analysis software ver. 3.3.070 was used for computation of the overall and subgroup magnitude of risk. Publication bias was assessed through funnel plots.
RESULTS
Results from all conducted searches were merged and duplicates removed, resulting in 91 abstracts and titles that were assessed for eligibility. Fifty three (53) studies were excluded and 38 full articles evaluated as eligible for inclusion into the systematic review. Of these, seven studies were excluded as they did not address the research question; five studies did not report the use of controls or comparisons8-12; two were meta-analyses2,6; two provided incomplete and non- extractable data8,13; one study had a data base used in a previous analysis14 other studies had sample sizes considered too small.15,16 A total of nineteen studies were included in the final analysis (Table 1).
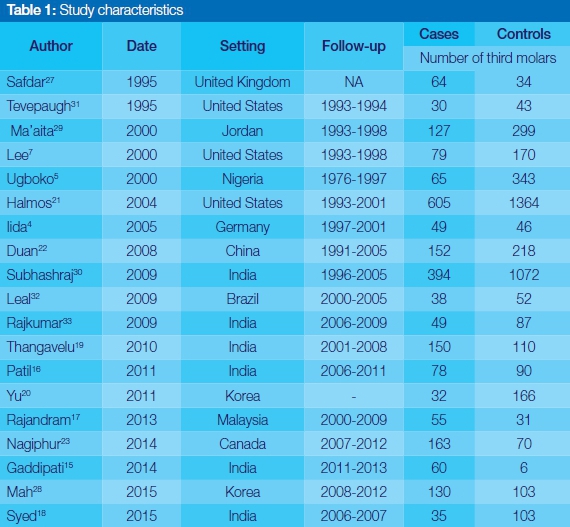
Most of the studies selected were from Asia8,15-20 (India and China), North America,7,14,21 with a few from Europe4 and Africa.5 All studies incorporated in this systematic review were retrospective cohort studies, with no prospective cohort study, or case control studies being eligible for inclusion in the meta-analysis. Based on the descriptive analysis, 3254 cases of angle fractures were reported from 9888 patients, whose records were collected over study periods ranging from a few months to 10 years. The mean (sd) age of the patients was 28.91 (2.27), and proportionally more males than females (82%:18%) had been enrolled.
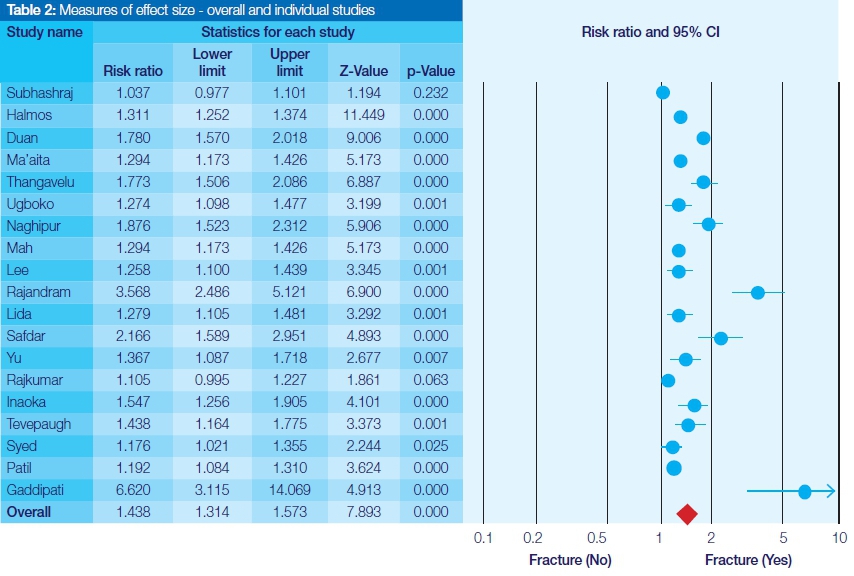
Statistical tests of heterogeneity revealed significant variability across studies and subgroups (Cochran Q, df, p, I2 = 179,18,0.00, 89.49). Based on this finding, the random effects model was adopted over the fixed effects model as the most appropriate estimate of the overall measure of risk. The overall relative risk for this meta-analysis was 1.44 (95% CI = 1.31 to 1.57). Subgroup analyses by sample size and outcome groups did not yield significantly different estimations of risk (Table 2). The researchers conclude that there is a 44% increase in the risk of mandibular angle fractures in patients with mandibular third molars, than in those without.
DISCUSSION
Validity of study findings - Role of chance, bias and confounding
This sample represents the largest number of studies included in a meta-analysis to date, with significantly more studies (n=19) from 11 countries being included in the final analysis. Chance or random error can be excluded as a possible explanation for the findings, because the study can be regarded as providing an unbiased and comprehensive estimation of risk.
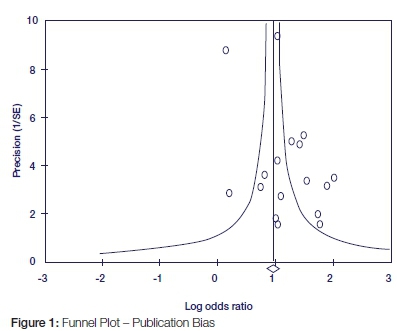
The funnel plot clearly indicates the paucity of negative studies in published literature. Such studies, if included in the meta-analysis, would attenuate the overall relative risk of 1.44 towards 1.00, thereby providing an alternative explanation of the association between third molars and mandibular fractures. On the contrary, the overwhelming absence of negative studies could indicate a true cause and effect relationship between angle fractures and third molars, and not a systematic error. Equally the effect of non-English or grey publications can be assumed to be negligible (Figure 1).
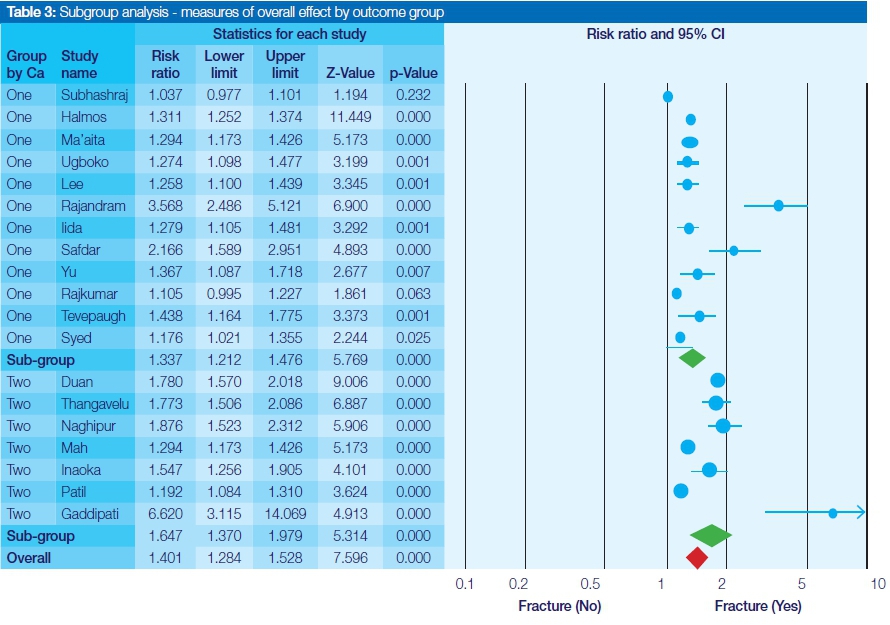
Subgroup analysis, according to the study outcome, indicates that there is a quantitative interaction between third molars and condylar and angle fractures. This is evidenced by a different yet positive magnitude of association between the two groups. The overall estimate, RR (95% CI) for two outcomes group versus one outcome group were 1.67 (95% CI = 1.37 to 1.98) and 1.33 (95% CI = 1.21 to 1.48) respectively (Table 3). This significant risk difference between the two groups is suggestive of the presence of interaction or confounding, suggestive that the presence of third molars modifies the risk of condylar fractures relative to angle fractures. Several authors emphasized the role of mandibular angle fractures in reducing the risk, and hence the incidence, of condylar fractures.10,15,22,23
According to Kober's biomechanical model,24 when force is applied to the mandible, it is transmitted along the entire structure. Therefore, when there is disruption of integrity of the mandible, due to fracture at the angle, forces will be dissipated and not be transmitted further. In the same way, the occurrence of a condylar fracture will reduce the risk of angle fractures.
Subgroup analysis by sample size shows that large studies are more precise in risk estimation than small studies. Relative risk (95% CI) for two groups were 1.39 (95% CI=1.24 to 1.56) versus 1.55 (95% CI = 1.31 to 1.83). (Table 4). Observed heterogeneity due to sample size is correlated with study duration and setting. Studies with longer follow-up and conducted in multiple sites reported larger sample sizes and less variance.
While evidence of bias and heterogeneity in this meta-analysis is minimal, these findings should be interpreted with caution, as there could be alternative explanations of the cause and effect. Overall the results are consistent with available best literature, and hence can be regarded as reasonable evidence.
Comparison of study findings
The majority of studies included in this meta-analysis report a mean sample age of 30 years or less, a statistic close to the average age of 29.81 in the current study. A preponderance of the studies reviewed highlight that over six times more males to females were treated for mandibular fracture. In corroboration, this study recorded that a preponderance of males were treated (82% to 18% females). These findings indicate the influence of age and gender in the epidemiology of mandibular fracture. It is hypothesized that male gender and youth predispose patients to risky behaviour resulting in an increase in cases of trauma.5-6
This meta-analysis study confirms a 1.44 times increased risk of mandibular fractures in the presence of third molars. This outcome is qualitatively similar, but quantitatively different in magnitude to the risk estimates in published meta-analyses and retrospective cohort studies. Bezerra et al2 found the relative risk to be 1.94, Hanson,6 2.4, and Syed,18 2.28, respectively. These results support the hypothesis that third molars reduce the resistance of the mandibular angle to fractures. While the relative risk of 1.44 is low compared with 1.94 and 2.4, we believe that this finding is more precise, providing better evidence due to the comparatively larger sample size.
The relative risk of mandibular angle to condylar fractures is 1.67 in the presence of third molars, while comparison with 'no fracture' gives a risk ratio of 1.33. This translates into a 34% reduction in the risk of mandibular angle fracture given the presence of condylar fractures and vice versa. Therefore, as the risk of angle fractures increases, there is a concomitant decrease in the likelihood of condylar fractures in the same patients.
CONCLUSION AND RECOMMENDATIONS
Based on the findings of this meta-analysis, we conclude that the presence of third molars increases the risk of mandibular angle fracture. We further note that the study did not assess the specific effects of the various types of impactions on the outcomes. Future studies should be well designed to provide valid evidence which could assist clinicians in making decisions about the management of third molars in populations at risk of fractures.
IMPLICATIONS FOR CLINICAL PRACTICE
This study provides consolidated evidence that the presence of mandibular third molars increases the risk of angle fractures. At the same time, these findings cannot be regarded as conclusive evidence in support of prophylactic removal of pathology free or impacted third molars. The low incidence (1-2%) of mandibular angle fractures as a result of the removal of third molars makes justification of these extractions very difficult, especially on grounds of possible future risk.25 Unfortunately, between 18% and 60% of patients undergo extraction of third molars for no valid reasons.26 Many clinicians still rely on untested beliefs, biases and unverifiable anecdote. In mitigation of this established practice, clinicians have to seek adequate consent from patients, given the greater risks than benefits of this elective procedure. Patients need to be made aware of the risks, and be part of decision-making. It is important for dentists to be discerning before referring patients for prophylactic removal of third molars. Evidence profiles patients who might benefit from removal of asymptomatic third molars to have the following characteristics: - (i) younger than 30 years of age; (ii) male gender; (iii) comorbidities such as osteoporosis and related bone density disorders; (iv) history of trauma especially facial fractures, and (v) high risk activities, such as contact sports, physical work, and strenuous recreation. Dentists should take thorough medical and dental histories in order to evaluate the degree of risk of mandibular angle fracture and refer appropriately.
ACRONYM
RR: relative risk
References
1. Kandasamy, S, Jerrold, L, Friedman, JW. Asymptomatic third molar extractions: Evidence-based informed consent. Journal of the World Federation of Orthodontists 1, e135-e138 (2012). [ Links ]
2. Bezerra, T, Silva, F, Scarparo, H, Costa, FWG, Studart-Soares, E. Do erupted third molars weaken the mandibular angle after trauma to the chin region? A 3D finite element study. International Journal of Oral and Maxillofacial Surgery 2013;42:474-80. [ Links ]
3. Meisami, T, Sojat, A, Sandor, G, Lawrence, H, Clokie, C. Impacted third molars and risk of angle fracture. International Journal of Oral and Maxillofacial Surgery 2002;31:140-4. [ Links ]
4. Iida, S, Hassfeld, S, Reuther, T, Nomura, K, Mühling, J. Relationship between the risk of mandibular angle fractures and the status of incompletely erupted mandibular third molars. Journal of Cranio-Maxillofacial Surgery 2005;33, 158-63. [ Links ]
5. Ugboko, V, Oginni, F, Owotade, F. An investigation into the relationship between mandibular third molars and angle fractures in Nigerians. British Journal of Oral and Maxillofacial Surgery 2000;38:427-9. [ Links ]
6. Hanson, BP, Cummings, P, Rivara, FP, John, MT. The association of third molars with mandibular angle fractures: a meta-analysis. Journal-Canadian ental Association 2004;70:39-43. [ Links ]
7. Lee, JT, Dodson, TB. The effect of mandibular third molar presence and position on the risk of an angle fracture. Journal of Oral and Maxillofacial Surgery 2000;58:394-8. [ Links ]
8. Abbasi, MM, Abbas I, Khan,N, Shah, SM, Hameed, H. Frequency of unerupted mandibular third molar in mandibular angle fractures. J Ayub Med Coll Abbottabad 2012; 24-9. [ Links ]
9. Yadav, S, Tyagi, S, Puri, N, Kumar, P, Kumar, P. Qualitative and quantitative assessment of relationship between mandibular third molar and angle fracture on North Indian population: A clinico-radiographic study. European Journal of Dentistry 2013;7:212-7. [ Links ]
10. Zhu, SJ, Choi, B, Kim, HJ, Park, WS, Huh, JY, Jung, JH. Relationship between the presence of unerupted mandibular third molars and fractures of the mandibular condyle. International Journal of Oral and Maxillofacial Surgery 2005;34:382-5. [ Links ]
11. Ashraf, N, Rehman, B, ud Din, Q. Mandibular third molar-a risk factor for angle fracture. JKCD 2013;4:25-8. [ Links ]
12. Vivek, G. The role of mandibular third molars on the incidence of condylar fractures-a clinical study. IOSR J Dental Med Sci 2014;13:27-30. [ Links ]
13. Dodson, TB. Impacted third molar and mandibular angle fractures. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology 1996;81:264. [ Links ]
14. Fuselier, JC, Ellis, EE, Dodson, TB. Do mandibular third molars alter the risk of angle fracture? Journal of Oral and Maxillofacial Surgery 2002;60:514-8. [ Links ]
15. Gaddipati, R, Ramisetty, S, Vura, N, Kanduri, RR, Gunda, VK. Impacted mandibular third molars and their influence on mandibular angle and condyle fractures-A retrospective study. Journal of Cranio-Maxillofacial Surgery 2014;42:1102-5. [ Links ]
16. Patil, PM. Unerupted lower third molars and their influence on fractures of the mandibular angle and condyle. British Journal of Oral and Maxillofacial Surgery 2012;50:443-6. [ Links ]
17. Rajandram, R, nABIL, S, Shareif, MS et al. Mandibular third molar and angle of mandible fractures. Sains Malaysiana 2013;42:39-43. [ Links ]
18. Syed, KB, Kota, Z, Ibrahim, M, Bagi, MA, Assiri, MA. Prevalence of impacted molar teeth among Saudi population in Asir region, Saudi Arabia-a retrospective study of three years. Journal of International Oral Health 2013;5:43. [ Links ]
19. Thangavelu, A, Yoganandha, R, Vaidhyanathan, A. Impact of impacted mandibular third molars in mandibular angle and condylar fractures. International Journal of Oral and Maxillofacial Surgery 2010;39:136-9. [ Links ]
20. Yu, S, Lee, H, Moon, J, Sohn, DA. Correlation between mandibular angle fracture and the mandibular third molar. J Koran Maxillofac Plast Reconstr Surg 2011;33:505-11. [ Links ]
21. Halmos, DR, Ellis, E, Dodson, TB. Mandibular third molars and angle fractures. Journal of Oral and Maxillofacial Surgery 2004;62:1076-81. [ Links ]
22. Duan, D, Zhang, Y. Does the presence of mandibular third molars increase the risk of angle fracture and simultaneously decrease the risk of condylar fracture? International Journal of Oral and Maxillofacial Surgery 2008;37:25-8. [ Links ]
23. Naghipur, S, Shah, A, Elgazzar, RF. Does the presence or position of lower third molars alter the risk of mandibular angle or condylar fractures? Journal of Oral and Maxillofacial Surgery 2014;72:1766-72. [ Links ]
24. Kober, C, Sader,R, Thiele, H, Baure, HI et al. Stress analysis of the human mandible in standard trauma situations with numerical simulation. Mund-, Kiefer-und Gesichtschirurgie: MKG 2001;5:114-9. [ Links ]
25. Adeyemo, WL. Do pathologies associated with impacted lower third molars justify prophylactic removal? A critical review of the literature. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology 2006;102:448-52. [ Links ]
26. Mettes, DT, Nienhuijs, MM, van der Sanden, WJ, Verdonschot, EH, Plasschaert, A. Interventions for treating asymptomatic impacted wisdom teeth in adolescents and adults. The Cochrane Library 2005. [ Links ]
27. Safdar, N, Meechan, J. Relationship between fractures of the mandibular angle and the presence and state of eruption of the lower third molar. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology 1995;79:680-4. [ Links ]
28. Mah, DH, Kim, SG, Moon, SY, Oh, JS, You, JS. Relationship between mandibular condyle and angle fractures and the presence of mandibular third molars. Journal of the Korean Association of Oral and Maxillofacial Surgeons 2015;41:3-10. [ Links ]
29. Ma'aita, J, Alwrikat, A. Is the mandibular third molar a risk factor for mandibular angle fracture? Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology 2000;89:143-6. [ Links ]
30. Subhashraj, K. A study on the impact of mandibular third molars on angle fractures. Journal of Oral and Maxillofacial Surgery 2009;67:968-72. [ Links ]
31. Tevepaugh, DB, Dodson, TB. Are mandibular third molars a risk factor for angle fractures?: A retrospective cohort study. Journal of Oral and Maxillofacial Surgery 1995;53:646-9. [ Links ]
32. Leal, J, Porto, GG. Relationship between mandibular fracture and impacted lower third molar. Med Oral Patol Oral Cir Bucal 2009;14:E349-354. [ Links ]
33. Rajkumar, K, Ramen, S, Chowdhury, R, Chattopadhyay, P. Mandibular third molars as a risk factor for angle fractures: a retrospective study. Journal of Maxillofacial and Oral surgery 2009;8:237-40. [ Links ]
 Correspondence:
Correspondence:
D Pagollang Motloba
E-mail: Pagollang.motloba@smu.ac.za

{kind=link}
{kind=link}
{kind=link}