










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.71 n.10 Johannesburg Nov. 2016
RESEARCH
Trends in the seasonal variation of dry socket at Medunsa Oral Health Centre
SR MthethwaI; BF MabhozaII
IBDS, MPH, PhD. Senior lecturer/Stomatologist, Department of Oral Pathology & Oral Biology. School of Oral Health Sciences, Sefako Makgatho Health Sciences University
IIBDS. Lecturer/Dentist. Department of Maxillofacial & Oral Surgery, School of Oral Health Sciences, Sefako Makgatho Health Sciences University
SUMMARY
INTRODUCTION: The multifactorial aetiology of dry socket is firmly established. A probable seasonal variation was recently explored - the results indicated a significantly lower risk in spring.
AIMS AND OBJECTIVES: This study sought to further explore the hypothesis of seasonal variation by describing trends in the occurrence of dry socket over three years at Medunsa Oral Health Centre.
DESIGN: This was a repeated cross sectional analytical study in which existing medical records were reviewed.
METHODS: Treatment records of 13615 adult patients who underwent routine tooth/teeth extraction(s) between January 2010 and December 2012 were reviewed. Data related to demographic characteristics, date of extraction, and diagnosis of dry socket were acquired. Dry socket odds were calculated. A Chi-squared test for trend was performed.
RESULTS: Females accounted for 66.4% of the dry socket cases. The mean age of the occurrence of dry socket was 36 years (SD 11years). The risk for dry socket was lowest during spring (September - November) throughout the years 2010 to 2012. Statistically significant seasonal variation was found in the years 2010 and 2011. Other significant risk factors included younger age and female gender.
CONCLUSIONS: The findings suggest a seasonal variation in the risk of dry socket.
INTRODUCTION AND BACKGROUND
Dry socket, a common painful complication of dental extraction, with an onset varying between one to four days after tooth extraction, is well-researched.1,2 A Medline database search covering the period from 1966 to 2007 conducted by Noroozi and Philbert (2009) using the term "dry socket" produced 317 records of original research and reviews in the English language.1 A few dozen more studies have since been conducted - the latest published in May 2016.3
Several terms have been used in referring to dry socket, amongst these being: alveolar osteitis, localised osteitis, postoperative alveolitis, alveolalgia, alveolitis sicca dolorosa, septic socket, necrotic socket, localized osteomyelitis, and fibrinolytic alveolitis.4,5 A recent review found twice as many clinical definitions of dry socket.4 Blum's definition is gaining wide acceptance -"postoperative pain in and around the extraction site, which increases in severity at any time between one and three days after the extraction, accompanied by a partially or totally disintegrated blood clot within the alveolar socket, with or without halitosis".4
Localised fibrinolysis occurring within the socket and subsequently leading to loss of the blood clot is believed to underlie the pathogenesis of dry socket.4,6
The occurrence of dry socket has been the subject of several studies.2,3,6,10 The incidence has been established for large and small patient groups mainly over study periods less than a year and has been reported to range between 1% and 4% for all routine non-surgical dental extractions and between 5% and 38% for removal of impacted mandibular third molars.3,4,7-13 The incidence of dry socket for routine dental extractions at Medunsa Oral Health Centre, a dental school and referral hospital in Garankuwa on the outskirts of Pretoria, was reported in a prospective study conducted over an eight-month period, to be 2%.14 The prophylactic and symptomatic management of dry socket has been thoroughly reviewed - the management guidelines were found to be based on expert opinions and clinical experience6 although the level of evidence for effectiveness of most guidelines was found to be low to moderate.6,15
The multifactorial aetiology of dry socket is firmly established, with numerous risk factors having been identified. Common amongst these are female gender, young adult, lower molars, traumatic extractions and smoking.16 Additional risk factors which have been implicated include pericoronitis and high pre- and post-operative bacterial counts seen in patients with poor oral hygiene and inadequate irrigation.17-19 The possibility of a seasonal variation in the incidence of dry socket has also long been suspected.20 This hypothesis was recently explored in a retrospective review of the records of patients spanning a period of one year at Medunsa Oral Health Centre.21 The results indicated a significantly lower risk in spring (September - November).21
The current study sought to further explore over a longer study period the hypothesis of seasonal variation of the incidence of dry socket at Medunsa Oral Health Centre
OBJECTIVES OF THE STUDY
To determine period prevalences and describe trends in the seasonally related occurrence of dry socket over three years, 2010 to 2012.
To evaluate the independent effects of gender, age, and season on the incidence of dry socket using logistic regression.
MATERIALS AND METHODS
Study design
This was a repeated cross sectional analytical study in which existing medical records were reviewed. Data was collected from three different time periods: between January 2010 and December 2010; between January 2011 and December 2011, and between January 2012 and December 2012 - to enable the assessment of trends over time.
Study population
The target population consisted of the treatment records of adult (18 years and older) patients who underwent routine non-surgical tooth/teeth extraction(s) at the Minor Oral Surgery clinic of Medunsa Oral Health Centre between January 2010 and December 2012. A total of 13615 records made up the population.
Study sample
Every available record was studied.
MEASUREMENTS
Medical records
Treatment records of 13615 adult patients who underwent routine non-surgical tooth/teeth extraction(s) at the Minor Oral Surgery clinic of Medunsa Oral Health Centre between January 2010 and December 2012 were reviewed. Data related to demographic characteristics, date of tooth/teeth extraction(s), and presence/absence of a diagnosis of dry socket were acquired and then captured in Microsoft Excel software.
Definition of variables
Age and Gender refer to patient age and sex as recorded in treatment records.
Seasons of diagnosis were determined according to Southern Hemisphere seasonal calendar: December - February (summer); March - May (autumn); June -August (winter); September - November (spring).22
Blum's definition4 was used to identify the symptoms recorded in the patient files as indicative of"dry socket".
Ethical considerations
Ethical approval for the study was granted by the Ethics Committee of the Sefako Makgatho Health Sciences University. Permission to conduct the study was granted by the Chief Executive Officer (CEO) of Medunsa Oral Health Centre.
STATISTICAL ANALYSIS/HYPOTHESIS TESTING
Data was coded and cleaned in Microsoft Excel software and was then transferred to Statistical Analysis Software (SAS) software for analysis.
Means, frequencies and proportions (percentages) were calculated. Analysis of Variance (ANOVA) was performed to determine whether the mean age differed in any patient groups.
The Chi-squared test (two-sided) was performed to test for statistical significance of the gender difference in dry socket occurrence and for the association between dry socket and seasonal variation.
A multivariable logistic regression analysis was performed to identify patient factors associated with dry socket in the study population. The binary outcome of interest was dry socket (Present/Absent). The determinants investigated included season, age, and gender. The estimated odds of dry socket for each season were compared to the data for winter. The deviances (-2log likelihood values) of two models, either excluding or including season, were compared to assess the significance of season. The chosen significance level of the tests was a p-value less than 0.05.
RESULTS
Data extracted from the study population of 13615 treatment records were analysed.
The mean ages of patients in the three groups in the population ranged between 40.19 and 42.82. There was substantial evidence (p< 0.001) that at least one group mean in the population differed from others. Pairwise post-hoc comparisons of the mean ages of patients in the three groups were all statistically significant. A significantly higher proportion of female patients had tooth/teeth extraction(s) (53.3% female vs 46.7% male: p< 0.001).


The period prevalences of dry socket throughout the years 2010 to 2012 were similar. There was insufficient evidence (p= 0.731) to reject the null hypothesis that the proportions of patients with dry socket would be equal in the three patient groups in the population.

The mean age of patients diagnosed with dry socket was the same (36 years) throughout the period investigated. There was insufficient evidence to reject the null hypothesis that the mean ages of patients in the three groups in the population would be the same.

Dry socket was diagnosed significantly more frequently among female than male patients (66.4% female vs 33.6% male: p< 0.001).
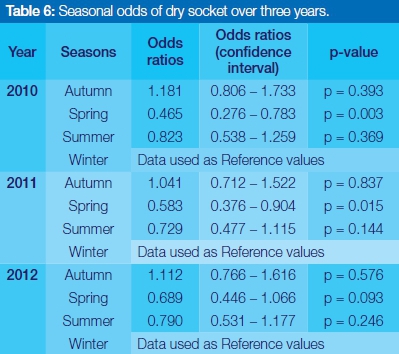
The prevalence of dry socket was highest in Autumn and lowest in Spring throughout the years 2010 to 2012. There was strong evidence (p= 0.003 and 0.030 respectively) of seasonal variation in the incidence of diagnoses of dry socket over the years 2010 and 2011. However, there was insufficient evidence (p= 0.117) to reject the null hypothesis that the proportions of patients diagnosed with dry socket were equal for all seasons in the year 2012.
The risk for dry socket was lower in Spring. The decline in risk was significant (p= 0.003, and p = 0.015 respectively) in Spring of the years 2010 and 2011.
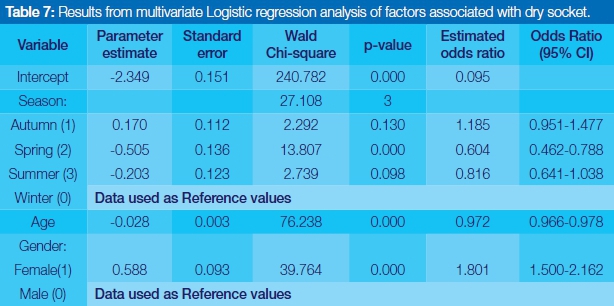
The results of this study indicated that the Spring season and older age were independently associated with lower odds, while the female gender was independently associated with higher odds of dry socket diagnosis.
Patients who had tooth/teeth extraction(s) in Spring had 0.604 times the odds of having dry socket as those who had tooth/teeth extraction(s) in Winter after adjusting for age and gender. In other words, the odds of developing dry socket in these patients in Spring were decreased by 40%.
Female patients had 1.801 times the odds of having dry socket as male patients after adjusting for age and season. In other words, the odds of developing dry socket in these patients were increased by 80%.
The incidence of dry socket decreased with age. For every year older than 18 years the odds were decreased by 2.8% after adjusting for season and gender.
The relationship between season and the occurrence of dry socket was significant
DISCUSSION
This study set out to describe trends in the occurrence of dry socket over a three year period at Medunsa Oral Health Centre in order to explore the hypothesis of a possible seasonal variation in the development of this condition.
Demographic characteristics
The results also showed that more women than men had a tooth or teeth extracted. This observation might be a reflection of higher attendance by females, which would be consistent with other research which found a large number of female patients at dental clinics.14,24 Indeed, the current study indicates that there were differences in the mean ages and gender of patients studied over the three years.
Trends in the prevalence of dry socket
The results of this study confirmed those of previous studies, indicating the frequency of dry socket to range between 0.5- 5% following routine extraction.1,3,6,25
These results differed from those published in 2008 (Singh and Bouckaert 2008),which estimated the incidence of dry socket at this facility to be only 2%.14 This variation could be attributed to sampling differences, in particular differences in the age composition of the study populations. The ages of patients in the previous study included children below 18 years (12-79 years with a mean age of 35 years). Children younger than 18 years were excluded from the current study. Furthermore, data in the previous study was collected over an eight-month period only, whilst data was collected continuously over a full year period in the current study.14 Results suggest that the prevalence of dry socket at Medunsa Oral Health Centre had been stable throughout the years 2010 to 2012.
The results further indicate a higher incidence of dry socket in female patients. These results are consistent with those of other studies and suggest a possible influence of hormonal differences between male and female.4,6,16
The mean age of patients diagnosed with dry socket was 36 years throughout the years 2010 to 2012 which is also consistent with previous reports that dry socket occurs most frequently between 20 and 40 years of age.6,16,25
The results of this study found strong evidence of seasonal variation in the years 2010 and 2011. However, no significant seasonal differences in the occurrence of dry socket were seen in 2012.
The most pertinent finding was the reduced risk of dry socket associated with the spring season as asserted by statistical tests of significance applied individually to the risk of dry socket between every other season compared with winter. This finding suggests that the association between the occurrence of dry socket and seasonal occurrence was not due to chance. These results however, need to be interpreted with caution as the association between the occurrence of dry socket and seasonal occurrence observed in this study may be due to measurement bias and confounding problems. For instance, the seasonal variation could also just be a reflection of seasonal differences in patient load that could conceivably influence how much time and thus care is spent on each extraction and thus the possibility of a traumatic extraction. Indeed, traumatic extractions have been associated with increased risk for dry socket. In addition the data in this study showed the patient load during Spring was consistently lower than the numbers seen in Winter (see Table 5)

Measurement bias could have arisen from inter-observer variation as an indeterminate number of clinicians were involved in the diagnosis of dry socket and possibly used non-standardized diagnostic criteria. It can be however be argued that the diagnostic criteria used in this study are highly sensitive since they are contained in most definitions used in the literature for the clinical assessment of the condition.
Many of the other relevant confounding variables i.e. site of extraction, traumatic extractions, smoking, pericoronitis, high pre and postoperative bacterial counts seen in patients with poor oral hygiene and inadequate irrigation, were not adjusted for in the multivariable regression model as data were not available.
It is difficult to explain the seasonal variation in the occurrence of dry socket, but it might be related to tea consumption patterns. Oldewage Theron and colleagues (2002) reported that tea was the third most consumed beverage in summer and the first most consumed beverage in winter.26 Hot tea may interfere with the healing process through loosening the scab that is forming over the socket. However, more research on this topic needs to be undertaken before the association between seasonal occurrence and dry socket is more clearly understood.
Factors associated with dry socket
In the current study the Spring season and older age were independently associated with a lower occurrence of dry socket, while being of female gender was independently associated with a higher occurrence of dry socket.
These results are consistent with those of other studies as they relate to gender.4,6,16 One of the issues that emerge from these findings is that the risk of dry socket decreased by 2.8% for every year older than 18 years. This finding suggests that older age played a protective role in the occurrence of dry socket in the current study. The association between dry socket and seasonal variation has not previously been described.20
Limitations of the study
Data were not available for many of the relevant confounding variables.
A potential threat to the internal validity of this study was the large number of tests of statistical significance which were carried out. This increases the type 1 error rate, which leads to risk for spurious relationships and thus the conclusions that can be reached. Accepting these limitations, the strength of this study nevertheless was the large sample size and the fact that it covered a three year period.
CONCLUSION
The current study findings, while preliminary, suggest a seasonal variation in the risk of incurring dry socket.
Conflict of interest: None declared.
References
1. Noroozi AR, Philbert RF. Modern concepts in understanding and management of the "dry socket" syndrome: comprehensive review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009; 107:30-5. [ Links ]
2. Cardoso CL, Rodrigues MT, Ferreira Júnior O, Garlet GP, de Carvalho PS. Clinical concepts of dry socket. J Oral Maxillofac Surg 2010; 68:1922-32. [ Links ]
3. Mudali V, Mohamed O. Incidence and predisposing factors for dry socket following extraction of permanent teeth at a regional hospital in Kwa-Zulu Natal. South African Dental Journal 2016; 71(4):166-9. [ Links ]
4. Blum IR. Contemporary views on dry socket (alveolar osteitis): a clinical appraisal of standardization, aetiopathogenesis and management: a critical review. Int. J. Oral. Maxillofac. Surg 2002; 31:309-17. [ Links ]
5. Torres-Lagares D, Serrera-Figallo MA, Romero-Ruiz MM, Infante-Cossío P, García-Calderón M, Gutiérrez-Pérez JL. Update on dry socket: A review of the literature. Med Oral Patol Oral Cir Bucal 2005; 10:77-85. [ Links ]
6. Bowe DC, Rogers S, Stassen LFA. The management of dry socket/alveolar osteitis. Journal of the Irish Dental Association 2011; 57(6): 305-10. [ Links ]
7. Butler DP, Sweet JB. Effect of lavage on the incidence of localized osteitis in mandibular third molar extraction sites. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1977; 44:14-20. [ Links ]
8. Turner PS. A clinical study of "dry socket." Int J Oral Surg 1982; 11:226. [ Links ]
9. Fridrich KL, Olson RA. Alveolar osteitis following surgical removal of mandibular third molars. Anesthesia Progress. 1990; 37(1):32-41. [ Links ]
10. Triegger N, Schlagel GD. Preventing dry socket: a simple procedure that works. J Am Dent Assoc 1991; 122:67-8. [ Links ]
11. Al-Khateeb TL, el-Marsafi AI, Butler NP. The relationship between the indications for the surgical removal of impacted third molars and the incidence of alveolar osteitis. Oral Maxillofac Surg 1991; 49:141-5. [ Links ]
12. Bloomer CR. Alveolar osteitis prevention by immediate placement of medicated packing. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000: 90: 282-4. [ Links ]
13. Kolokythas A, Olech E, Miloro M. Alveolar Osteitis: A Comprehensive Review of Concepts and Controversies. International Journal of Dentistry. 2010:249073 Epub 2010. [ Links ]
14. Singh AS, Mohamed A, Bouckaert MM. A clinical evaluation of dry sockets at the Medunsa Oral Health Centre. South African Dental Journal 2008; 63(9):490,492-3. [ Links ]
15. Sharif MO, Dawoud BES, Tsichlaki A, Yates JM. Intervention for the prevention of dry socket: an evidence-based update. British Dental Journal 2014; 217(1): 27-30. [ Links ]
16. MacGregor AJ. Aetiology of dry socket: a clinical investigation. Br J Oral Surg 1968; 6:49-58. [ Links ]
17. MacGregor AJ, Hart P. Bacteria of the extraction wound. J Oral Surg 1970; 28:885-7. [ Links ]
18. Brown LR, Merrill SS, Allen RE. Microbiologic study of intraoral wounds. J Oral Surg 1970; 28:89-95. [ Links ]
19. Larsen PE. The effect of a chlorhexidine rinse on the incidence of alveolar osteitis following the surgical removal of impacted third molars. J Oral Maxillofac Surg 1991; 49:932-7. [ Links ]
20. Carter. Dental question on seasonal correlation of dry socket symptomology. In: Letter to the Tom Bearden Website 31 Oct 2001. Available http://www.cheniere.org/correspondence/index.html [Accessed 04 April 2014]. [ Links ]
21. Maboza BJ, Mthethwa SR. Seasonal variation of dry socket at Medunsa Oral Health Centre. Proceedings of the 46th Scientific Meeting of the South African Division; Pretoria: International Association of Dental Research, 2015. [ Links ]
22. South African Weather Service. How are the dates of the four seasons worked out? Available http://www.weathersa.co.za/learning/weather-questions/82-how-are-the-dates-of-the-four-seasons-worked-out?recache=1 [Accessed 04 April 2014]. [ Links ]
23. Petrie A, Sabin C. Medical Statistics at a Glance, 2nd ed. Massachusetts: Blackwell Publishing, 2005: 125. [ Links ]
24. Lesolang RR, Motloba DP, Lalloo R. Patterns and reasons for tooth extraction at the Winterveldt Clinic: 1998-2002. SADJ June 2009; 64 (5): 214-8. [ Links ]
25. Momeni H, Shahnaseri S, Hamzeheil Z. Evaluation of relative distribution and risk factors in patients with dry socket referring to Yazd dental clinics. Dental Research Journal 2011; 8(5): S84-7. [ Links ]
26. Oldewage Theron W H, Dicks E, Selepe, M. Tea consumption patterns of 13-25 year-olds in the Vaal Triangle, South Africa. African Journal of Food, Agriculture, Nutrition and Development 2002; 2(1): 38-45. [ Links ]
 Correspondence:
Correspondence:
Sibusiso Rockfort Mthethwa
Medunsa Campus
PO Box D24
Sefako Makgatho Health Sciences University 0204
Tel: 012 521 5888
Fax: 012 512 4274
Email: rocky.mthethwa@smu.ac.za

{kind=link}
{kind=link}